Download presentation
Presentation is loading. Please wait.

1
Faculty of Health Sciences Dr. Laila Akhu-Zaheya Faculty of Nursing/ Jordan University of Science & Technology Dr. Shannon Doocy; Emily Lyles; Timothy Roberton School of Public Health/ Johns Hopkins National Survey of Syrian Refugees' Access To Health Care In Jordan

2
Organizational Partners This is survey is a joint effort of the following organizations: Johns Hopkins University (JHU) – Lead Research Organization – responsible for development of the study design & questionnaire, technical support & management of data collection, data analysis & preparation of findings. Jordan University of Science & Technology (JUST) – Implementing Partner – responsible for supporting development of the study, including ensuring appropriateness of the local context, attaining local ethical approval, providing interviewers & team leaders & logistics support during implementation, & review of findings. World Health Organization (WHO)—Study Funder & Technical Partner – responsible for technical input on study design & questionnaire content, logistics support & review of findings. UNHCR—Technical partner – responsible for technical input on study design & questionnaire content, support with sampling & review of findings.
 – Implementing Partner – responsible for supporting development of the study, including ensuring appropriateness of the local context, attaining local ethical approval, providing interviewers & team leaders & logistics support during implementation, & review of findings. World Health Organization (WHO)—Study Funder & Technical Partner – responsible for technical input on study design & questionnaire content, logistics support & review of findings. UNHCR—Technical partner – responsible for technical input on study design & questionnaire content, support with sampling & review of findings..")
3
Background Syrian Civil War, 2011 Since then, number of Syrian refugees is escalating This creates a burden on the Jordanian Health System, who is struggling to meet current demands. However, there is no clear picture of the Syrian refugees' access to health care in Jordan.

4
Purpose

6
Sampling High precision was not a major concern A power of.80 & a design effect of 2.0 to account for a cluster sample design were used Account for 10% attrition Minimum sample size identified: 900 refugee households However, it was increased to 1500

7
Sampling Two stage- Cluster Design 125 cluster / 12 Households Probability proportional to size sampling was used using UNHCR registration data In each cluster, UNHCR randomly selected five registered refugee households that were listed as living in that cluster’s assigned sub-district

8
Questionnaire Design The questionnaire was developed by consensus between WHO, UNHCR & JHSPH The questionnaire completed on tablets using Magpi software The questionnaire was organized into the following sections: – Section 1. Interview Background Information – Section 2. Respondent information & Household Characteristics – Section 3. Healthcare Access – Section 4. Child Healthcare Seeking – Section 5. Children’s Vaccination – Section 6. Adult Healthcare Seeking – Section 7. Antenatal care – Section 8. Hospitalization – Section 9. Hypertension – Section 10. Cardiovascular disease – Section 11. Diabetes – Section 12. Chronic Respiratory Disease – Section 13. Arthritis – Section 14. Household Economy – Section 15. Syrian Refugee Questions

9
Ethical Consideration This study was approved by: – Ethics review committees at JUST & WHO-Geneva – JHSPH Institutional Review Board – Jordan Ministry of Health

10
Survey Implementation Conducted by faculty & graduate students at JHSPH & JUST/FON A total of 48 JUST faculty & graduate students interviewers & six team leaders were trained to collect the data The team received two days of classroom training focused on the questionnaire, e-data collection using tablets, interview techniques, basic principles of human subjects’ protections & sampling methods A pilot survey of 67 households in Amman was conducted to finalize the questionnaire & understand potential logistical challenges that might arise An additional day of training was then held to provide the full interviewer team with the opportunity to practice locating households & conducting interviews with the target population

11
Survey Implementation Data collected between June 8 th & 22 nd, 2014 Six teams; each consists of team leader & 6-8 interviewers Team leader a head of time arranged for the starting household interview in each cluster using a list of phone numbers of registered Syrian refugees in the designated sub-district provided by UNHCR Team leader asked about other Syrian households living in the area Sample size was limited to 12 households per cluster with each team completing two clusters per day (a total of 24 full interviews per day per team) In sub-districts with fewer registered refugees or areas more geographically difficult to access, teams were scheduled to complete only one cluster per day
 In sub-districts with fewer registered refugees or areas more geographically difficult to access, teams were scheduled to complete only one cluster per day")
12
Interviews Took an average of 45 minutes (R: 30-60 min.) Conducted in a place that allowed confidentiality of responses No information was recorded on the survey to protect the anonymity of respondents Verbal informed consent from all participants was obtained Potential respondents assured that the decision to take part or to refuse would not influence on access to assistance
 Conducted in a place that allowed confidentiality of responses No information was recorded on the survey to protect the anonymity of respondents Verbal informed consent from all participants was obtained Potential respondents assured that the decision to take part or to refuse would not influence on access to assistance")
13
Results A total of 1634 households were approached. Of these, – 2.9% (n=47) were not at home – 0.8% (n=14) were already interviewed for this survey – 1.4% (n=23) declined to be interviewed – The final sample was 1550 households 94.7% response rate
 were not at home – 0.8% (n=14) were already interviewed for this survey – 1.4% (n=23) declined to be interviewed – The final sample was 1550 households 94.7% response rate.")
14
Demographic Characteristics A total of 1550 households participated in the survey with 9580 household members Predominant respondents were female (61.7%) Mean age of 38 years (Med=36, R: 15-95) Less than a quarter completing secondary education The average household size was 6.2 (R=1 - 20) Syrian refugees in the North of Jordan had a significantly larger household size (6.7), while in the Center (5.7) & Southern regions (5.4)(p< 0.001) 64.6% of households had one or more children in the 0-5 age range & 89.6% had children between 6-17 years of age
 Mean age of 38 years (Med=36, R: 15-95) Less than a quarter completing secondary education The average household size was 6.2 (R=1 - 20) Syrian refugees in the North of Jordan had a significantly larger household size (6.7), while in the Center (5.7) & Southern regions (5.4)(p< 0.001) 64.6% of households had one or more children in the 0-5 age range & 89.6% had children between 6-17 years of age")
15
Living Conditions The majority of households (87.1%) lived in apartments or houses Other types of accommodations included: – Additions to houses (8.5%) – Tent, shacks or other temporary structures (2.7%) – Unfinished buildings or construction sites (1.5%) – Almost all households rented their accommodations (96.1%) A small proportion were hosted by families without making payments (2.5%) One percent reported other types of arrangements. These included: – Occupying accommodations in exchange for work – Paying to occupy, & staying without permission – No significant differences in residence type were observed by region within Jordan

16
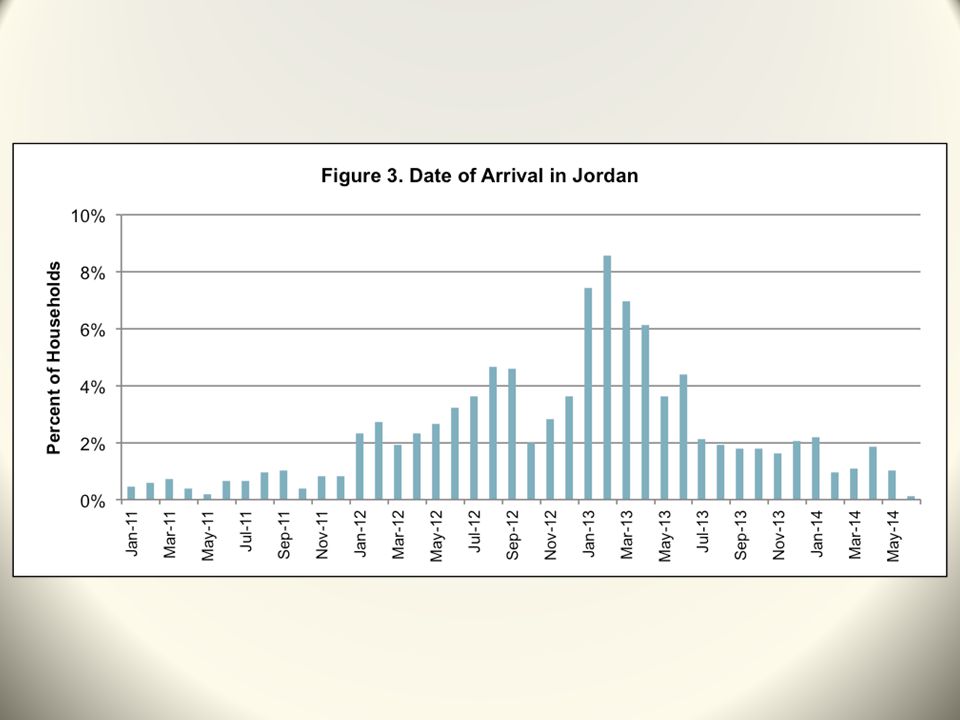
Time of Arrival Only Syrian households arriving in Jordan in 2011 or after were eligible to participate in the survey Of the households included in the survey: – 7.8% arrived in 2011 – 36.5% arrived in 2012 – 48.5% arrived in 2013 & – 7.3% arrived the first six months of 2014

18
Household Welfare Household Economy – Mean & median monthly household incomes were 228 JD & 100 JD respectively (No significant differences in monthly income were observed by region) – The mean monthly expenditure was 472 JD (Med 416 JD) – Significant differences in mean household expenditures were observed by region(p<0.001) The North reporting the highest expenditures (M=490 JD) The Center average expenditures (M=461 JD) The South reporting the lowest expenditures (M=415 JD) – Highest proportion of spending included: Housing (30.9%) Food (29.4%) Health (9.7%) Transportation (7.4%) Non-specific spending (22.6%)
 – The mean monthly expenditure was 472 JD (Med 416 JD) – Significant differences in mean household expenditures were observed by region(p<0.001) The North reporting the highest expenditures (M=490 JD) The Center average expenditures (M=461 JD) The South reporting the lowest expenditures (M=415 JD) – Highest proportion of spending included: Housing (30.9%) Food (29.4%) Health (9.7%) Transportation (7.4%) Non-specific spending (22.6%)")
19
Perceptions of Health Access in Jordan Five different components of access to medical care were assessed: 1.Perceived ability to access medical care 2.Perceived ability to access medical specialists (challenging) 3.Affordability of medical care (Perceived negatively) 4.Affordability of medications (Perceived negatively) 5.Receipt of health information
 3.Affordability of medical care (Perceived negatively) 4.Affordability of medications (Perceived negatively) 5.Receipt of health information")
20
Perceptions of Health Access in Jordan

21
Household Health Facility Utilization Majority of households (84.5%) reported seeking care at public sector facilities; while less than half (45.7%) sought care at private facilities since their arrival in Jordan Majority of care seekers (58.2%) accessed public health facilities using public transportation No significant differences between regions in the proportion of households that ever used a government or private health facility However, there were marginally significant differences in frequency of use of public facilities within the six months preceding the survey (p=0.062) – South visited (M= 7.8 times); Northern (M= 6.2) & Central regions (M=5.6) Also significant differences in frequency of private facility use (p=0.04) – South visited (M=3.8 times); Northern (M=4.4) & Central regions (M=4.5)
 reported seeking care at public sector facilities; while less than half (45.7%) sought care at private facilities since their arrival in Jordan Majority of care seekers (58.2%) accessed public health facilities using public transportation No significant differences between regions in the proportion of households that ever used a government or private health facility However, there were marginally significant differences in frequency of use of public facilities within the six months preceding the survey (p=0.062) – South visited (M= 7.8 times); Northern (M= 6.2) & Central regions (M=5.6) Also significant differences in frequency of private facility use (p=0.04) – South visited (M=3.8 times); Northern (M=4.4) & Central regions (M=4.5)")
22
Health Seeking & Service Utilization Among Adults No significant differences in reasons for needing medical care for an adult household member were observed by region The majority of households reported needing medical care for an adult within the month preceding the survey The primary reasons reported by adults for needing medical care: – Infection or communicable disease (21.2%) – Chronic medical conditions & non-communicable diseases (19.4%) – Injuries (9.4%) – Dental care (7.8%)
 – Chronic medical conditions & non-communicable diseases (19.4%) – Injuries (9.4%) – Dental care (7.8%)")
23
Health Seeking & Service Utilization Among Adults 13.9% of households did not seek care for an adult last time it was needed No significant differences in reasons for not seeking care were observed by region

24
Reasons for Not Seeking Adult Health Care

25
Access to Medicines Among Adults Among adult care seekers, 87.4% reported being prescribed medication at their most recent visit to a health facility in Jordan No significant differences were observed by region Significant differences were observed between provider types(p=0.005): – Greatest proportion of patients receiving a prescription were observed in private facilities (91.6%) – The lowest were in charity facilities (84.3%) Of those prescribed medication: – 89.8% were able to obtain all of prescribed medications – Slightly more than half (58.5%) reported paying for the medications – The average out-of-pocket cost among all households that accessed medications was 14.2 JD (Med=5, R 0-500) The primary reasons of not obtaining medications: – Medication was out of stock at the public facility (51.6%) – Household could not afford the medication (39.8%) – No significant difference in reasons for not obtaining medications was observed by region
: – Greatest proportion of patients receiving a prescription were observed in private facilities (91.6%) – The lowest were in charity facilities (84.3%) Of those prescribed medication: – 89.8% were able to obtain all of prescribed medications – Slightly more than half (58.5%) reported paying for the medications – The average out-of-pocket cost among all households that accessed medications was 14.2 JD (Med=5, R 0-500) The primary reasons of not obtaining medications: – Medication was out of stock at the public facility (51.6%) – Household could not afford the medication (39.8%) – No significant difference in reasons for not obtaining medications was observed by region")
26
Hospitalization 21.2% of households reported one or more hospitalizations of a household member in the year preceding the survey & a mean of 2.1 (Med=1, R=1-20) hospitalizations in the six months preceding the survey No significant differences were observed in the proportion of hospitalization or the average number of hospitalization by region No significant differences in causes for hospitalization by region or facility type Most common reasons for hospitalization: – Injury (20.7%) – Cardiovascular conditions (13.7%) – Respiratory conditions (12.7%)
 hospitalizations in the six months preceding the survey No significant differences were observed in the proportion of hospitalization or the average number of hospitalization by region No significant differences in causes for hospitalization by region or facility type Most common reasons for hospitalization: – Injury (20.7%) – Cardiovascular conditions (13.7%) – Respiratory conditions (12.7%)")
27
Hospitalization by Sector & Region* *Statistically significant differences between Region (p=0.006)
")
28
Hospitalization Cost (41.8%) & health emergency (25.6%) are the main reasons for selecting the hospital where care was sought No significant differences in length of hospital stay were observed by facility sector; However, significant differences were observed in length of stay by region(p=0.04) ; stays were the longest in the North at 6.6 days (Med=3, range 1-120) as compared to 5.4 days (Med=2, range 1-80) in Central Jordan & 3.2 days in South Jordan (Med=2, range 1-16)
 & health emergency (25.6%) are the main reasons for selecting the hospital where care was sought No significant differences in length of hospital stay were observed by facility sector; However, significant differences were observed in length of stay by region(p=0.04) ; stays were the longest in the North at 6.6 days (Med=3, range 1-120) as compared to 5.4 days (Med=2, range 1-80) in Central Jordan & 3.2 days in South Jordan (Med=2, range 1-16)")
29
Hospitalization For the most recent hospitalization, 22.3% reported on an out-of-pocket payment, with a mean cost of 146.3 JD (Med=0, range 0-6000) Significant differences in the amount of out-of-pocket payments were observed by region & provider type; with highest being in Central Jordan (31%) compared to 14.9% in the North & 5.3% in the South Mean out-of-pocket payments for the most recent hospitalization differed significantly by provider sector (p=0.053); private sector (M= 421.3 JD); public sector (M=47.3 JD), & charity (M=137.0 JD)
 Significant differences in the amount of out-of-pocket payments were observed by region & provider type; with highest being in Central Jordan (31%) compared to 14.9% in the North & 5.3% in the South Mean out-of-pocket payments for the most recent hospitalization differed significantly by provider sector (p=0.053); private sector (M= JD); public sector (M=47.3 JD), & charity (M=137.0 JD)")
30
Prevalence of Chronic Health Conditions About 43.4% of all households reported one or more household members that had been previously diagnosed with at least one of the five included chronic health conditions (Hypertension, Arthritis, Diabetes Mellitus, Chronic Respiratory Disease, or Cardiovascular Disease) – Chronic respiratory diseases most prevalent among 0-17 year olds (3.0%) – Chronic respiratory diseases (17.5%) & arthritis (11.8%) were most prevalent among those 18 to 39 years old – Hypertension was most prevalent in the ages between 40 & 59 years (66.8%) & in those 60 years & over (80.9%)
 – Chronic respiratory diseases most prevalent among 0-17 year olds (3.0%) – Chronic respiratory diseases (17.5%) & arthritis (11.8%) were most prevalent among those 18 to 39 years old – Hypertension was most prevalent in the ages between 40 & 59 years (66.8%) & in those 60 years & over (80.9%)")
32
Care Seeking for Chronic Health Conditions Among the 1154 individuals who reported seeking care for one of the included chronic health conditions in Jordan, – 53.9% received care in public facilities including: public hospitals (22.1%), primary health care centers (20.8%), & comprehensive health centers (10.7%) Private facilities were utilized by 29.6% of chronic condition care seekers, including private hospitals (6.8%) & private clinics (12.8%) The remaining care seeking chronic health condition patients sought care from other sources including shops or other informal providers (1.6%), pharmacies (6.1%), charity & NGO facilities (16.6%), & Syrian doctors (2.1%)
, primary health care centers (20.8%), & comprehensive health centers (10.7%) Private facilities were utilized by 29.6% of chronic condition care seekers, including private hospitals (6.8%) & private clinics (12.8%) The remaining care seeking chronic health condition patients sought care from other sources including shops or other informal providers (1.6%), pharmacies (6.1%), charity & NGO facilities (16.6%), & Syrian doctors (2.1%)")
33
Access to Medicines for Chronic Health Conditions Medications were prescribed for 88.9% of chronic health condition cases 85.5% of chronic health condition cases reported currently taking medication for their condition Medication use reportedly stopped, or medication ran out, for longer than two weeks in the past year in 26.5% of cases, most commonly due to high cost (reported by 59.1% of those stopping medication)
")
34
Limitations Sampling bias Questionnaire content Data collection Interviewers’ misunderstanding

35
Thank You

Similar presentations



 Patient-Centered Medical Home (PCMH) by the National.>")

















