Download presentation
Presentation is loading. Please wait.

1
Newer approaches to treatment of disseminated disease Matteo Landriscina, MD PhD Assistant Professor of Clinical Oncology University of Foggia UNKNOWN PRIMARY TUMORS: NEWER CONCEPTS AND APPROACHES Rome, March 5-6, 2010

2
DEFINITION Carcinoma of unknown primary (CUP) is a biopsy- proven metastatic malignant tumor whose primary site can not be identified during pretreatment evaluation including: 1.Thorough history and physical exam 2.Laboratory and radiographic studies 3.Detailed histological evaluation
 is a biopsy- proven metastatic malignant tumor whose primary site can not be identified during pretreatment evaluation including: 1.Thorough history and physical exam 2.Laboratory and radiographic studies 3.Detailed histological evaluation")
3
EPIDEMIOLOGY CUP constitutes 2-4% of all malignacies Annual age-adjusted incidence in US is 7-12 cases per 100,000 population Median age at presentation is 60 years Slightly more prevalent in males 5-10% of case are characterized by a relatively favourable prognosis

4
FAVORABLE SUBSETS 1.Women with isolated axillary adenopathy 2.Women with papillary serous adenocarcinoma of the peritoneal cavity 3.Squamous cell carcinoma involving cervical lymph nodes 4.Isolated inguinal adenopathy from squamous cell carcinoma 5.Men with bone metastases, elevated serum PSA, or PSA positive on tumor staining 6.Men with poorly differentiated carcinoma of midline distribution 7.Poorly differentiated neuroendocrine carcinoma 8.Single, small and potentially resectable metastatic site

5
UNFAVOURABLE SUB-SETS Adenocarcinoma metastatic to the liver or other organs Non-papillary malignant ascites (adenocarcinoma) Multiple cerebral metastases (adeno or squamous carcinoma) Multiple lung/pleural metastases (adenocarcinoma) Multiple metastatic bone disease (adenocarcinoma)
 Multiple cerebral metastases (adeno or squamous carcinoma) Multiple lung/pleural metastases (adenocarcinoma) Multiple metastatic bone disease (adenocarcinoma)")
6
TREATMENT UNFAVORABLE SUBSETS With the exception of the favorable subsets, most patients with CUP have a tumor that is resistant to chemotherapy The prognosis is very poor, with median survival of 2 to 3 months in unselected patients and 6 to 10 months in those enrolled into clinical trials Patients with good performance status may benefit from systemic chemotherapy

7
Chemotherapy for unfavorable subsets Open Questions Which chemotherapy regimen? Is the combination of Platinum and Taxane the standard of care? Is there any role for a third agent?

8
TREATMENT UNFAVORABLE SUBSETS Platinum/Taxane chemotherapy regimens Author/yearChemotherapyPatientsRR (%)MS (months) Voog (2000)CpE23328 Briasoulis (2000)PCb773913 Greco (2000)DCb47228 Greco (2000)DCp26 8 Park (2004)PCp374211 Berry (2007)PCb (weekly)42188.5 Pentheroudakis (2008) DCb4732 (46)16.2 (22.6) Cb –Carboplatin; Cp – Cisplatin; D – Docetaxel, E – Etoposide, P – Paclitaxel
MS (months) Voog (2000)CpE23328 Briasoulis (2000)PCb Greco (2000)DCb47228 Greco (2000)DCp26 8 Park (2004)PCp Berry (2007)PCb (weekly) Pentheroudakis (2008) DCb4732 (46)16.2 (22.6) Cb –Carboplatin; Cp – Cisplatin; D – Docetaxel, E – Etoposide, P – Paclitaxel")
9
TREATMENT UNFAVORABLE SUBSETS Triplet chemotherapy regimens Author/yearChemotherapyPatientsRR (%)MS (months) Greco (2000)PCbE714811 Greco (2002)PCbG120259 Greco (2004)PCbE132309 Schneider (2007)CbGCAP33397.6 Cb –Carboplatin; E – Etoposide, G – Gemcitabine; P – Paclitaxel Pentheroudakis (2009) Platinum conining regimens 918329
MS (months) Greco (2000)PCbE Greco (2002)PCbG Greco (2004)PCbE Schneider (2007)CbGCAP Cb –Carboplatin; E – Etoposide, G – Gemcitabine; P – Paclitaxel Pentheroudakis (2009) Platinum conining regimens")
10
TREATMENT UNFAVORABLE SUBSETS Anthracycline and Gastrointestinal-type chemotherapy regimens Author/yearChemotherapyPatientsRR (%)MS (months) Piga (2005)CbEA10226.59 Briasoulis (2008)IrOx47139.5 Sprenger (2008)CAPOx51127.3 Holtan (2008)GIr31127.3 Cb –Carboplatin; E – Etoposide, G – Gemcitabine; A – doxorubicin; Ir – irinotecan; CAP – capecitabine; Ox - oxaliplatin Pentheroudakis (2009) Anthracyclin- conining regimens 401227
MS (months) Piga (2005)CbEA Briasoulis (2008)IrOx Sprenger (2008)CAPOx Holtan (2008)GIr Cb –Carboplatin; E – Etoposide, G – Gemcitabine; A – doxorubicin; Ir – irinotecan; CAP – capecitabine; Ox - oxaliplatin Pentheroudakis (2009) Anthracyclin- conining regimens")
11
TREATMENT UNFAVORABLE SUBSETS Gemcitabine or Irinotecan containig doublets Author/yearChemotherapyPatientsRR (%)MS (months) Pouessel (2004)DG354010 Pittman (2006)CbG51308.5 Ando (2008)CbIr434011.4 Yonemari (2009)CbIr454212.2 Cb –Carboplatin; D – Docetaxel, G – Gemcitabine; Ir - irinotecan
MS (months) Pouessel (2004)DG Pittman (2006)CbG Ando (2008)CbIr Yonemari (2009)CbIr Cb –Carboplatin; D – Docetaxel, G – Gemcitabine; Ir - irinotecan")
12
Phase II randomized trials Author/yearChemotherapyPatientsRR (%)MS (months) Dowell (2001)PFU CbE 3219 8.4 6.5 Coline (2003)CpGEM CpIR 8055 38 8686 Assersohn (2003)FUPVI FUMit 8811.6 20 6.6 4.7 Palmieri (2006)Cp/CbP Cp/CbVI 6648 42 9.6 13.6 Huebner (2009)PCb GEMVI 9023.8 20 11 7 Hainsworth (2010)PCbE GEMIr 19818 7.4 8.5 Cb –Carboplatin; Cp – Cisplatin; GEM – gemcitabine; FU – 5-fluorouracil; Mit – Mitomycin; Ir – irinotecan; VI – vinorelbine; E – Etoposide, P – Paclitaxel
MS (months) Dowell (2001)PFU CbE Coline (2003)CpGEM CpIR Assersohn (2003)FUPVI FUMit Palmieri (2006)Cp/CbP Cp/CbVI Huebner (2009)PCb GEMVI Hainsworth (2010)PCbE GEMIr Cb –Carboplatin; Cp – Cisplatin; GEM – gemcitabine; FU – 5-fluorouracil; Mit – Mitomycin; Ir – irinotecan; VI – vinorelbine; E – Etoposide, P – Paclitaxel")
13
Randomized phase III comparison of paclitaxel/carboplatin/etoposide versus gemcitabine/irinotecan, both followed by gefitinib, in patients (pts) with carcinoma of unknown primary site (ASCO 2009, Abs 4931) 198 pts were randomized to paclitaxel, carboplatin, etoposide (PCE, 93 pts) or gemcitabine, irinotecan (GI, 105 pts). Responding/stable pts then received gefitinib until tumor progression. Median progression-free survival for PCE versus GI was 3.2 months versus 5.3 months, p=0.19 Median overall survivals were 7.4 months (PCE) versus 8.6 months (GI), p=0.34 2-year survivals were 16% (PCE) and 19% (GI) Response rates were similar (PCE 19%, GI 20%) GI was less toxic, with lower rates of grade 3/4 neutropenia (11% vs. 35%; p< 0.01), febrile neutropenia (0% vs. 9%; p<0.01), thrombocytopenia (3% vs. 8%; p=.05), anemia (3% vs. 9%; p=0.05), and RBC transfusions (10% vs. 24%; p<0.01).
 versus 8.6 months (GI), p= year survivals were 16% (PCE) and 19% (GI) Response rates were similar (PCE 19%, GI 20%) GI was less toxic, with lower rates of grade 3/4 neutropenia (11% vs. 35%; p< 0.01), febrile neutropenia (0% vs. 9%; p<0.01), thrombocytopenia (3% vs. 8%; p=.05), anemia (3% vs. 9%; p=0.05), and RBC transfusions (10% vs. 24%; p<0.01)..")
14
CONCLUSIONS Clinical trials evaluated a group of heterogeneous tumors sharing the unique characteristic of metastatic disease without identifiable origin at the time of initial therapy Only phase II trials, few randomized No randomized phase III trials designed to establish the efficacy of combination chemotherapy over BSC or Platinum single agent Among unfavourable subsets, patients with good performance status may benefit from systemic chemotherapy There is no chemotherapy of choice although the most commonly used regimens use the combination of a platinum and a taxane The role for a third agent such as gemcitabine, irinotecan or etoposide remains unclear

15
Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis Golfinopoulos et al, 2009 Meta-analysis of 10 randomized controlled trials comparing at least two different systemic regimens or a systemic regimen to no treatment Data on favorable subset CUP were excluded Overall 683 subjects were randomly assigned No trials compared systemic treatment to BSC

16
Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis Golfinopoulos et al, 2009

17
Multiple-treatment meta-analysis for death Golfinopoulos et al, 2009

18
Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis Golfinopoulos et al, 2009 Multiple-treatments meta-analysis showed no significant benefit for any treatment group over others No type of chemotherapy has been solidly proven to prolong survival in patients with CUP Regimens using either platinum or taxanes or both show some trends for prolongation of survival, but the data a limited. Taxane regimens seem to have the best results Median OS is 8-12 months for the trial published after the year 2000, but this gain may not necessary depend on systemic chemotherapy A taxane/platimun combination may prolong survival by 1.5 months BSC may be considered for old or unfit unfavorable CUP

19
Open Issues Molecular assignment of tissue of origin and response to chemotherapy Molecular-targeted agents in unknown primary carcinomas Liver metastases of unknown origin

20
Autopsy-found primaries, N = 644 (%) Lung 27 Pancreas 24 Liver/bile duct 8 Kidney/adrenals 8 Bowel 7 Genital system 7 Stomach 6 Bladder/ureter 0.01 Breast 0.007 Other 10 DNA-assigned primaries, N > 500 (%) Lung 11.5 Pancreas 12.5 Liver/bile duct 8 Kidney/adrenals 6 Bowel 12 Genital system 9 Stomach 3 Bladder/ureter 5 Breast 15 Other 18
 Lung 27 Pancreas 24 Liver/bile duct 8 Kidney/adrenals 8 Bowel 7 Genital system 7 Stomach 6 Bladder/ureter 0.01 Breast Other 10 DNA-assigned primaries, N > 500 (%) Lung 11.5 Pancreas 12.5 Liver/bile duct 8 Kidney/adrenals 6 Bowel 12 Genital system 9 Stomach 3 Bladder/ureter 5 Breast 15 Other 18")
21
N RR (%) MS (months) CUP-PlatinumAdvanced NSCLC N RR (%) MS (months) 5895 30-45 8-11 918 32 9 Adv Pancreas 4465 10-25 5-9 CUP-Anthra or GI 401 22 7 Adv breast 3953 40-70 18-24 Adv colon 13875 35-55 15-20 Chemotherapy activity and patients outcome in CUP and metastatic tumors of known primary
 MS (months) CUP-PlatinumAdvanced NSCLC N RR (%) MS (months) Adv Pancreas CUP-Anthra or GI Adv breast Adv colon Chemotherapy activity and patients outcome in CUP and metastatic tumors of known primary")
22
Molecule Ras HER2 EGFR C-KIT PDGFR BCL2 P53 VEGF VEGFR Therapeutic modulation Farnesyl-transferase inhibitors Antibodies, tyrosine kinase inhibitors Tyrosine kinase inhibitors Antisense oligonucleotides Gene therapy, degradation inhibitors Antibodies Tyrosine kinase inhibitors Developed agents Tipifarnib, lonafarnib Trastuzumab, lapatinib Cetuximab, gefitinib, erlotinib Imatinib, sunitinib Oblimersen G3139 ONYX015, INGN201, MI63 Bevacizumab ZD6474, sorafenib, sunitinib Promising molecular targets and targeting compounds in CUP Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006

23
AuthorN Clinicopathologic parameters and outcome Pavlidis, 199526 Results Method: IHC HER2 expression 65%, overexpression 27% None Hainsworth, 2000100HER2 overexpression 11%None Fizazi, 200356HER2 overexpression 4%None Rashid, 200576HER2 expression 68%, Overexpression 24% Co-expression of EGFR, HER2 and VEGF or Cox-2 in 54%. Superior survival on co-expession of EGFR, HER2 and Cox-2. HER2 signalling in CUP Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006

24
AuthorN Clinicopathologic parameters and outcome Fizazi, 200356 Results Method: IHC, PCR, qPCR EGFR overexpession 4% None Rashid, 200576EGFR expression 75%, overexpression 61% Co-expression of EGFR, HER2 and VEGF or Cox-2 in 54%. Superior survival on coexpession of EGFR, HER2 and Cox-2 Dova, 200550EGFR expression 74%, overexpression 12% Wild-type exons 18,19,21 EGFR gene in 96%. No exons 18, 19, 21 EGFR gene amplification None EGFR signalling in CUP Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006

25
EGFR expression and response to chemotherapy Massard, Br J Cancer, 2007

26
AuthorN Clinicopathologic parameters and outcome Fizazi, 200356 Results Method: IHC, PCR, qPCR C-KIT overexpression 11% None Rashid, 200576C-KIT expression 12%, overexpression 4% None Dova, 200550C-KIT expression 81%, overexpression 13% No exon 11 C-KIT gene mutations None cKIT signalling in CUP Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006

27
AuthorN Clinicopathologic parameters and outcome Van de Wouw, 2004 48 Results Method: IHC CD34 microvessel density median 56/mm 3. VEGF expression 39%, overexpression 26% None Hillen, 1997 69No difference in CD34 microvessel density between 39 CUP liver metastases and 30 known primary liver metastases CD34 microvessel density with adverse prognostic significance for survival Karavasilis, 2005 80CD34 microvessel density median 59 microvessels/mm 2 Positive correlation of VEGF with microvessel density. Angiogenesis in CUP (1) Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006 VEGF expression 100%, overexpression 83% Increased microvessel density in unfavourable group CUP
 Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006 VEGF expression 100%, overexpression 83% Increased microvessel density in unfavourable group CUP.")
28
AuthorN Clinicopathologic parameters and outcome Karavasilis, 2005 75 Results Method: IHC MMP2 expession 69%, overexpression 49% MMP9 expession 49%, overexpression 36% TIMP1 expession 79%, overexpression 44% Correlation of MMP2 and MMP9 expression. Adverse prognostic significance of TIMP1 expression Rashid, 2005 75VEGF expression 49%, Overexpression 29% Co-expression of EGFR, HER2 and VEGF or Cox-2 in 54% Angiogenesis in CUP (2) Pentheroudakis and Pavlidis, Cancer Treat Rev, 2006
 Pentheroudakis and Pavlidis, Cancer Treat Rev,")
29
Phase II trial which evaluated the combined inhibition of VEGF and EGFR with bevacizumab and erlotinib. Patients who either had received previous chemotherapy or were previously untreated with poor- prognosis clinical features. All patients received bevacizumab 10 mg/kg every 2 weeks, along with erlotinib 150 mg orally daily. 47/51 patients received at least 8 weeks of treatment. 10% PR, 61% SD Median survival for the entire group was 7.4 months, with 33% of patients alive at 1 year. This regimen was well tolerated by most patients.

30
Hainsworth, J. D. et al. J Clin Oncol; 25:1747-1752 2007

32
The Community Oncologist Paclitaxel/Carboplatin plus Bevacizumab/Erlotinib in the First-Line Treatment of Patients with Carcinoma of Unknown Primary Site John D. Hainswortha, David R. Spigela, Dana S. Thompson, Patrick B. Murphy, Cassie M. Lane, David M. Waterhouse, Yuval Naot, F. Anthony Greco Phase II trial with the combination of paclitaxel, carboplatin, bevacizumab, and erlotinib in the first- line treatment of patients with CUP 49/60 patients completed 4 cycles of therapy, and 44 received maintenance bevacizumab and erlotinib. 53% with major responses to treatment; 18 patients with SD. Median PFS was 8 months, with 38% of patients progression-free at 1 year. Median survival 12.6 months; 2-year overall survival rate 27%. Treatment was generally well tolerated.

33
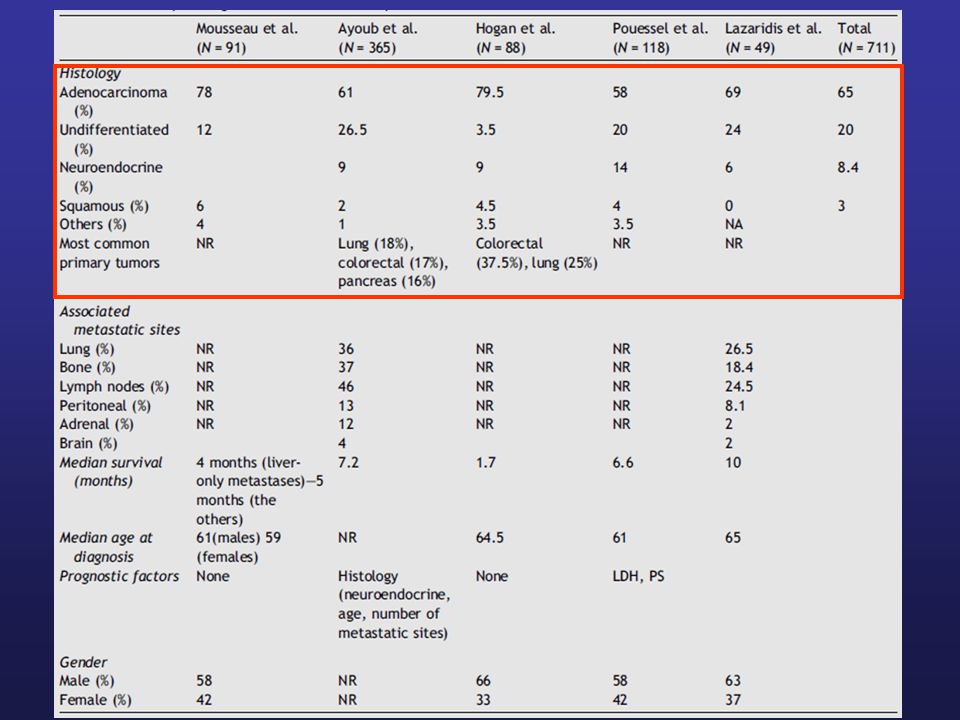
CUPL is an unfavourable subset of cancer of unknown primary site Male/female ratio 2:1. Median age at diagnosis: 61–65. Lung, pancreatic and colorectal primary tumors are most commonly identified in the setting of CUP patients presenting with liver metastases The most commonly involved metastatic sites in addition to hepatic involvement are lymph nodes, bone and lung. Adenocarcinoma is the prevalent histology (64%), followed by undifferentiated carcinoma (20%), neurondocrine (8.4%) and squamous (3%). Liver Metastasis subgroup
, followed by undifferentiated carcinoma (20%), neurondocrine (8.4%) and squamous (3%). Liver Metastasis subgroup.")
35
Liver Metastasis subgroup Response to chemotherapy Lazaridis et al, Cancer Tret Rev, 2008

36
Liver Metastasis subgroup Lazaridis et al, Cancer Tret Rev, 2008

37
Liver Metastasis subgroup Prognostic factors for OS Lazaridis et al, Cancer Tret Rev, 2008

38
Histology (neuroendocrine differentiation) Liver Metastasis only/Number of metastatic sites Age Performance Status Liver Metastasis subgroup Prognostic Factors
 Liver Metastasis only/Number of metastatic sites Age Performance Status Liver Metastasis subgroup Prognostic Factors")
39
TREATMENT FAVORABLE SUBSETS 1. Women with isolated axillary adenopathy Lymph nodes should be tested for ER, PR, and HER-2/neu In cases of negative mammogram, the primary may be seen on MRI or after mastectomy Prognosis is similar to lymph node positive breast cancer Mobile lymph nodes (N1) - Treat as stage IIA breast cancer Fixed lymph nodes (N2) - Treated as stage IIIA breast cancer MRM + AND chemotherapy ± hormonal therapy/RT Neoadjuvant chemotheray for N2 disease
 - Treat as stage IIA breast cancer Fixed lymph nodes (N2) - Treated as stage IIIA breast cancer MRM + AND chemotherapy ± hormonal therapy/RT Neoadjuvant chemotheray for N2 disease.")
40
TREATMENT FAVORABLE SUBSETS 2. Women with papillary serous adenocarcinoma of the peritoneal cavity The germinal epithelium of the ovary and peritoneal mesothelium share the same embryological origin More common in women with BRCA-1 mutation and may also be seen after prophylactic oophorectomy Outcomes are similar to ovarian cancer at equivalent stage Patients should be treated as stage III ovarian carcinoma Surgical debulking followed by chemotherapy

41
TREATMENT FAVORABLE SUBSETS 3. Squamous cell carcinoma of the cervical lymph nodes Despite aggressive diagnostic approach, the primary site is not found in the majority of patients Ipsilateral tonsilectomy is often performed since the primary can be found in 10 to 25% of cases - Small tumors may originate in the deep crypts and not be detected by superficial biopsy Treat as locally advanced head and neck cancer Low stage (N1) – Surgery RT or RT alone High stage (N2-N3) - Chemoradiotherapy
 – Surgery RT or RT alone High stage (N2-N3) - Chemoradiotherapy.")
42
TREATMENT FAVORABLE SUBSETS 4. Isolated inguinal squamous cell carcinoma Tumor is usually located in the genital or anorectal area Patients without an identifiable primary tumor may benefit from inguinal lymphadenectomy, with or without adjuvant radiation therapy The role for chemotherapy in the adjuvant setting is not well defined Surgery ± RT, ? chemotherapy

43
TREATMENT FAVORABLE SUBSETS 5. Men with bone metastases, elevated serum PSA, or PSA positive on tumor staining Prostate cancer is the most likely diagnosis 1. Elderly men with adenocarcinoma of unknown primary and predominantly blastic bone metastases 2. Patients with increased PSA or positive PSA staining on the biopsy specimen despite atypical presentation Hormonal therapy

44
TREATMENT FAVORABLE SUBSETS 6. Men with poorly differentiated carcinoma of midline distribution Young males with tumors of predominant midline distribution (mediastinum and retroperitoneum) should be treated as extragonadal germ cell tumors Cisplatin-based chemotherapy (BEP)
 should be treated as extragonadal germ cell tumors Cisplatin-based chemotherapy (BEP).")
45
TREATMENT FAVORABLE SUBSETS 7. Poorly differentiated neuroendocrine carcinoma IHC usually stains positive for chromogranin or NSE Patients frequently present with diffuse metastases to the liver or bones Platinum-based chemotherapy (platinum + etoposide)
.")
46
TREATMENT FAVORABLE SUBSETS 8. Single metastatic site Although other metastatic sites may become evident within a short period, some patients may achieve a prolonged disease- free interval with local therapies such as surgery or radiotherapy Adjuvant chemotherapy may also be considered Surgery or RT

47
CONCLUSIONS Potential roles for DNA microarray technology 1.Identify the primary site 2.Identify clinically relevant subsets of tumors with similar gene expression profiles 3.Identify specific and novel targets for treatment Targeted therapies such as EGFR inhibitors and anti- angiogenesis agents may have a role in the treatment of CUP, particularly in patients with unfavorable subsets –PR 10%, SD 61%, Median survival 7.4 months in 2 nd line –RR 53%, PFS 8 months, median survival 12.6 months in 1 st line

48
Current Clinical Practice Diagnosis of metastatic carcinoma Search for primary site Rule out non-carcinoma histology Lymphoma, melanoma, sarcoma Identify favorable subgroups Unfavorable subgroup Poor PS BSC Good PS ●Clinical trial ● Platinum-taxane chemotherapy AND

Similar presentations





 Baselga.>")


 and N+, chemotherapy should be added.>")

 Alone or in Combination with Carboplatin/Paclitaxel (CP) in Never or Light Former Smokers with Advanced Lung.>")
 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")


 Scientific Achievements.>")





