Download presentation
Presentation is loading. Please wait.

1
PULP CAP KAMLOOPS APRIL 14, 2012

4
RETROSPECTIVE STUDIES 1. Bogan G et al JADA 2008:39 (3) 305-315 97% 2. Fuks AB, Pediatr Dent 1982,4: 240-244 81% success on permanent incisors 3. Barthel CR,J Endod 2000; 26: 525-528 37% @ 5 years, 13% @10 years

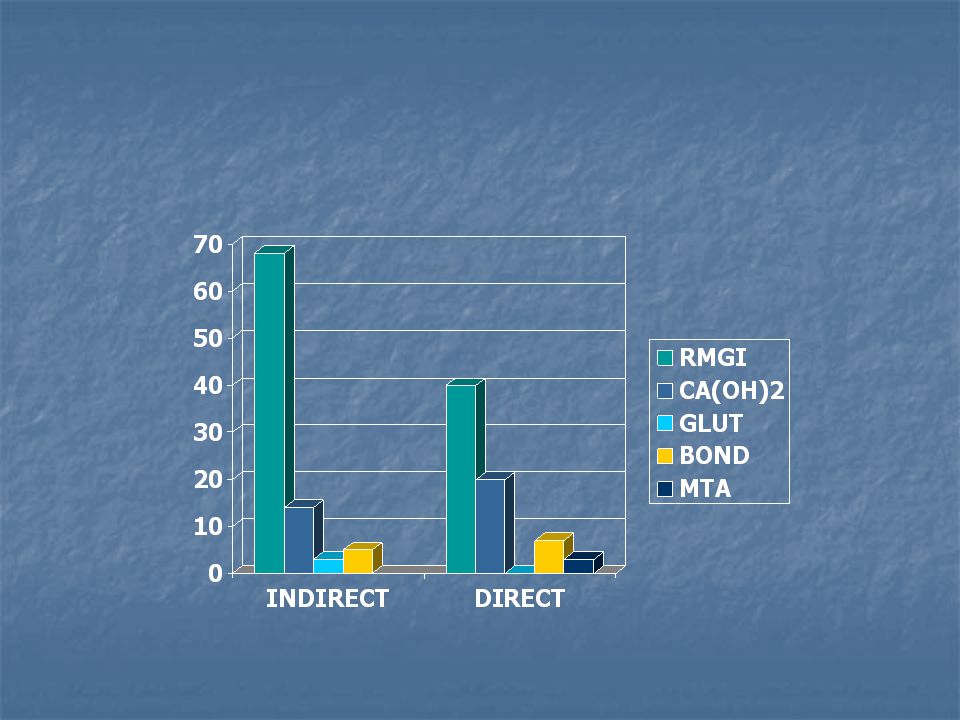
5
PULP CAP MATERIALS ? CR NEWS Jan 2010 RMGI Vitrebond Plus or GC Fuji Lining LC RMGI Vitrebond Plus or GC Fuji Lining LC Indirect 40% Indirect 40% Indirect 68% Indirect 68% Calcium Hydroxide Calcium Hydroxide 28% Direct, 28% Direct, 14% Indirect 14% Indirect Bonding agent Bonding agent Direct 7% Direct 7% Indirect 5% Indirect 5% Laser 2% Direct Laser 2% Direct Gluteraldehyde Indirect 3% Gluteraldehyde Indirect 3% MTA 3% Direct MTA 3% Direct Polycarboxylate – no mention Polycarboxylate – no mention Glass Ionomer – no mention Glass Ionomer – no mention English sparrow poop English sparrow poop

6
CR News Jan 2010 vol 3 issue 1 1. CR respondents; success rates 1. 3 years: Direct 58%, Indirect 70% 2. 5 years: Direct 48%, Indirect 61%

7
MTA Bogan G et al JADA 2008:39 (3) 305-315 Bogan G et al JADA 2008:39 (3) 305-315 Direct pulp capping with Mineral Trioxide aggregate – an Observational Study. Direct pulp capping with Mineral Trioxide aggregate – an Observational Study. Over an observation period of nine years, the authors followed 49 of 53 teeth and found that 97.96% percent had favorable outcomes on the basis of radiographic appearance, subjective symptoms and cold testing. Over an observation period of nine years, the authors followed 49 of 53 teeth and found that 97.96% percent had favorable outcomes on the basis of radiographic appearance, subjective symptoms and cold testing.

8
MTA BOGAN PEDO FUKS PULP CAP SUCCESS RATES

11
SUCCESSFUL PULP CAPS Inflammation management

12
SUCCESSFUL PULP CAPS Inflammation management

13
SUCCESSFUL PULP CAPS Inflammation management

14
RADIOGRAPHIC CONTRAINDICATIONS RADIOGRAPHIC CONTRAINDICATIONS APICAL RADIOLUCENCY APICAL DETERIORATION - CONDENSING OSTEITIS THREADLIKE PULP PULP STONES CLASS V PROBABLE FUTURE PULP OCCLUSION E.G. CLASS V RADIOGRAPHICLY EVIDENT CARIOUS INVASION OF PULP CHAMBER

15
DIAGNOSTIC CONTRAINDICATIONS = HISTORY OF ++ PAIN APICAL TENDERNESS APICAL TENDERNESS SPONTANEOUS SPONTANEOUS LONG STANDING LONG STANDING NOCTURNAL NOCTURNAL THROBBING THROBBING ENDURING ENDURING SICKENING SICKENING CONSTANT NEED OF MEDICATIONS CONSTANT NEED OF MEDICATIONS

16
OPERATIVE OBSERVATIONS CONTRAINDICATIONS AT EXPOSURE EXUDATE – SEROUS EXUDATE – SEROUS PUS PUS PROLONGED CLOTTING TIME > 5 MINS PROLONGED CLOTTING TIME > 5 MINS >3MM EXPOSURE >3MM EXPOSURE EXPLORER INTO THE PULP (OPERATOR ERROR) EXPLORER INTO THE PULP (OPERATOR ERROR)
 EXPLORER INTO THE PULP (OPERATOR ERROR)")
17
SUCCESSFUL PULP CAPS Inflammation management

18
FORMULA FOR CARIES DETECTOR ACID RED 52 2% IN PROPYLENE GLYCOL ACID RED 52 2% IN PROPYLENE GLYCOL COMPOUNDING PHARMACY COMPOUNDING PHARMACY $30 FOR 200 CC.= 5 YEARS’ SUPPLY $30 FOR 200 CC.= 5 YEARS’ SUPPLY ref

20
CARIES DETECTOR - NO EFFECT ON BOND STRENGTH El-Housseiny and Jamjoum, J Clin Pediat Dent 200 El-Housseiny and Jamjoum, J Clin Pediat Dent 200 Kazemi et al, Oper Dent 2002 Kazemi et al, Oper Dent 2002

21
AFFECTED DENTIN INFECTED DENTIN

22
SETTING THE STAGE FOR PULPAL HEALING EXPOSURE ZONE: EXPOSURE ZONE: LOW/NIL BACTERIAL COUNT LOW/NIL BACTERIAL COUNT CONTIGUOUS ZONE CONTIGUOUS ZONE BIOCOMPATIBLE AND BIOCOMPATIBLE AND CALCIGENIC AGENT CALCIGENIC AGENT VISIBLE DELINEATION FOR VISIBLE DELINEATION FOR FUTURE INTERVENTIONS FUTURE INTERVENTIONS PERIPHERAL ZONE PERIPHERAL ZONE SEAL (ZERO MICROLEAKAGE) SEAL (ZERO MICROLEAKAGE)
 SEAL (ZERO MICROLEAKAGE)")
24
TUBULES TUBULES % AREA % AREA NUMBER/ MM 2 NUMBER/ MM 2 DIAMETER DIAMETER PRESSURENILPOSITIVE PRESSURENILPOSITIVE SE BONDS LESS EFFECTIVE THAN ETCH AND RINSE IN DEEP DENTIN SE BONDS LESS EFFECTIVE THAN ETCH AND RINSE IN DEEP DENTIN 20 K 58K 1u 3u 10% 88%

25
SUCCESSFUL PULP CAPS Inflammation management

26
LEAVING CARIES? REFERENCE REFERENCE

27
2 APPLICATIONS ONE MINUTE EACH ref CR JAN 2010

28
CR News Jan 2010 vol 3 issue 1 CR News Jan 2010 vol 3 issue 1 http://www.cliniciansreport.org/products/d ental-reports/january-2010-volume-3- issue-1.php http://www.cliniciansreport.org/products/d ental-reports/january-2010-volume-3- issue-1.php http://www.cliniciansreport.org/products/d ental-reports/january-2010-volume-3- issue-1.php http://www.cliniciansreport.org/products/d ental-reports/january-2010-volume-3- issue-1.php Subscription required Subscription required

29
OTHER INTRAORAL DISINFECTANTS ENDODONTIC ENDODONTIC SILVER NITRATE SILVER NITRATE IODINE IODINE FORMOCRESOL FORMOCRESOL CA(OH)2 CA(OH)2 PULPAL PULPAL HYPOCHLORITE - KANCA HYPOCHLORITE - KANCA CHLORHEXEDINE- MANY CHLORHEXEDINE- MANY ref
2 CA(OH)2 PULPAL PULPAL HYPOCHLORITE - KANCA HYPOCHLORITE - KANCA CHLORHEXEDINE- MANY CHLORHEXEDINE- MANY ref")
30
CHLORHEXEDINE NO EFFECT ON BOND STRENGTH Santos et al, JOE, 2006 Santos et al, JOE, 2006 Perdiao et, Am J Dent 1994 Perdiao et, Am J Dent 1994

31
WHAT ABOUT SURFACE DISINFECTANTS? 70% ALCOHOL WITH PHENOLS 70% ALCOHOL WITH PHENOLS 70% ALCOHOL WITH CHX 70% ALCOHOL WITH CHX ACCELERATED PEROXIDE ACCELERATED PEROXIDE HYPOCHLORITE HYPOCHLORITE ref

32
NaOCl IS A STRONG OXIDIZING AGENT IS A STRONG OXIDIZING AGENT REDUCES BOND STRENGTH OF DENTIN BONDING AGENTS REDUCES BOND STRENGTH OF DENTIN BONDING AGENTS Ari et al, JOE, 2003 Ari et al, JOE, 2003 Erdemir et al, JOE, 2004 Erdemir et al, JOE, 2004 Santos eta l JOE, 2006 Santos eta l JOE, 2006 Lai et al, J Deny Res 2001 Lai et al, J Deny Res 2001

33
REVERSING NaOCl EFFECTS ON DBAS A reducing agent, such as ascorbic acid, or sodium ascorbate, can reverse the effect of NaOCl on bonding strength Morris et al, JOE, 2001 Lai et al, J Dent Res, 2001 Yiu et al, J Dent Res, 2002 Weston et al JOE, 2007: 10% Na ascorbate for 1 min restored the origonal bond strenghts

34
EDTA reverses effect of NaOCl Doyle t al, JOE, 2006 Doyle t al, JOE, 2006 A final rinse with EDTA reversed the effects of NaOCl on bonding A final rinse with EDTA reversed the effects of NaOCl on bonding

35
H2O2 reduces bond strength of DBAs Erdemir et al JOE, 2004 Erdemir et al JOE, 2004 Nikaido et al, Am J Dent 1999 Nikaido et al, Am J Dent 1999

36
DEEP CARIES DISINFECTION Optim 33TB Sci Can Optim 33TB Sci Can One minute kill One minute kill =10 Log -6 =10 Log -6 TB effective TB effective CR tested April 2007 CR tested April 2007 Excellent surface cleaner Excellent surface cleaner Tissue compatible Tissue compatible

37
WALFORD DEEP CARIES / EXPOSURE PROTOCOL GET CLOSE GET CLOSE OPTIM 33TB ONE MINUTE OPTIM 33TB ONE MINUTE NO DETECTOR NO DETECTOR CAREFUL ECAVATION CAREFUL ECAVATION SLOW RPMS SLOW RPMS SPOON SPOON SMEAR CLEAR ONE MINUTE SMEAR CLEAR ONE MINUTE REMOVE SMEAR LAYER REMOVE SMEAR LAYER OPTIM 33 ONE MINUTE OPTIM 33 ONE MINUTE PENETRATE TUBULES PENETRATE TUBULES

38
REMOVING SMEAR LAYER & PENETRATING TUBULES EDTA EDTA SmearClear (SybronEndo) SmearClear (SybronEndo) QMix (Tulsa/Dentsply) QMix (Tulsa/Dentsply) Acid etch Acid etch
 SmearClear (SybronEndo) QMix (Tulsa/Dentsply) QMix (Tulsa/Dentsply) Acid etch Acid etch")
39
WALFORD DEEP CARIES / EXPOSURE PROTOCOL GET CLOSE: OPTIM 33TB ONE MINUTE GET CLOSE: OPTIM 33TB ONE MINUTE NO DETECTOR NO DETECTOR CAREFUL ECAVATION CAREFUL ECAVATION SLOW RPMS SLOW RPMS SPOON SPOON SMEAR CLEAR ONE MINUTE SMEAR CLEAR ONE MINUTE REMOVE SMEAR LAYER REMOVE SMEAR LAYER OPTIM 33 ONE MINUTE OPTIM 33 ONE MINUTE PENETRATE TUBULES PENETRATE TUBULES SMEAR CLEAR (as reducer) SMEAR CLEAR (as reducer) EXPOSE if still carious EXPOSE if still carious MTA DIRECT CAP MTA DIRECT CAP OVERSEAL WITH GLASS IONOMER or CA(OH)2 OVERSEAL WITH GLASS IONOMER or CA(OH)2 ALLOW TO SET ALLOW TO SET ETCH PRIME BOND ETCH PRIME BOND OVERSEAL FLOWABLE/CURE OVERSEAL FLOWABLE/CURE FLOWABLE /CURE FLOWABLE /CURE RESTORE FOLLOWING LOW CONTRACTION STRESS PRINCIPLES RESTORE FOLLOWING LOW CONTRACTION STRESS PRINCIPLES
 SMEAR CLEAR (as reducer) EXPOSE if still carious EXPOSE if still carious MTA DIRECT CAP MTA DIRECT CAP OVERSEAL WITH GLASS IONOMER or CA(OH)2 OVERSEAL WITH GLASS IONOMER or CA(OH)2 ALLOW TO SET ALLOW TO SET ETCH PRIME BOND ETCH PRIME BOND OVERSEAL FLOWABLE/CURE OVERSEAL FLOWABLE/CURE FLOWABLE /CURE FLOWABLE /CURE RESTORE FOLLOWING LOW CONTRACTION STRESS PRINCIPLES RESTORE FOLLOWING LOW CONTRACTION STRESS PRINCIPLES")
43
MTA: SUPPLIER CLINICAL RESEARCH DENTAL CLINICAL RESEARCH DENTAL LONDON ONTARIO LONDON ONTARIO 1800 265 3444 1800 265 3444 “MTA ANGELUS WHITE” “MTA ANGELUS WHITE”

46
MTA MECHANISM Silviera CMM et al. Repair of Furcal Perforation with Mineral Trioxide Aggregate: Long-Term Follow-Up of 2 Cases JCDA October 2008 Vol 74 #8 729-732 Silviera CMM et al. Repair of Furcal Perforation with Mineral Trioxide Aggregate: Long-Term Follow-Up of 2 Cases JCDA October 2008 Vol 74 #8 729-732 http://www.cda-adc.ca/jcda/vol-74/issue- 8/729.html http://www.cda-adc.ca/jcda/vol-74/issue- 8/729.html http://www.cda-adc.ca/jcda/vol-74/issue- 8/729.html http://www.cda-adc.ca/jcda/vol-74/issue- 8/729.html

47
MTA MECHANISM Saidon J et al. OSOMOPOR Endod 2003:95:483-489 “ Cell and tissue reactions to mineral trioxide aggregate (MTA) and Portland cement. ” Saidon J et al. OSOMOPOR Endod 2003:95:483-489 “ Cell and tissue reactions to mineral trioxide aggregate (MTA) and Portland cement. ” MTA and Portland cement show comparative biocompatibility when evaluated in vitro and in vivo. The Portland cement was sterilized by ethylene oxide. MTA and Portland cement show comparative biocompatibility when evaluated in vitro and in vivo. The Portland cement was sterilized by ethylene oxide.
 and Portland cement. Saidon J et al. OSOMOPOR Endod 2003:95: Cell and tissue reactions to mineral trioxide aggregate (MTA) and Portland cement. MTA and Portland cement show comparative biocompatibility when evaluated in vitro and in vivo. The Portland cement was sterilized by ethylene oxide. MTA and Portland cement show comparative biocompatibility when evaluated in vitro and in vivo. The Portland cement was sterilized by ethylene oxide..")
48
MTA MENTE ET AL MTA MENTE ET AL Johannes Mente, DMD, et al J. Endo May 2010 806-814 Mineral Trioxide Aggregate or Calcium Hydroxide Direct Pulp Capping: An Analysis of the Clinical Treatment Outcome 5 years, 167 teeth 78% success MTA, 60% Ca(OH) 2 i.e. Twice as much failure with Ca(OH) 2
 2 i.e. Twice as much failure with Ca(OH) 2.")
49
Mente, DMD, et al J. Endo May 2010 Dentin bridge formation with MTA seems to be more homogenous (fewer tunnel defects) and more localized than that formed with Ca(OH)2 (20–24). caries was excavated from the cavity walls. Near to the pulp, except for one carious spot, the removal of which resulted in exposure of the pulp, the cavities were routinely disinfected with 0.12% chlorhexidine solution (Glaxo Smith Kline GmbH, Buhl, Germany). Resolution of bleeding from the exposed pulp in less than 5minutes was considered to be indicative of reversible inflammation The MTA pulp cap was overlaid with a thin protective layer of resin modified glass ionomer cement (Vitrebond; 3M Espe) The reduction in clinical success if a direct pulp capping is not followed immediately with permanent restoration has been shown in other clinical studies (11, 12) The longer the follow-up period, the more evident the trend became to a decline in the success rate of the teeth in the Ca(OH)2 group compared with the MTA group.
 and more localized than that formed with Ca(OH)2 (20–24). caries was excavated from the cavity walls. Near to the pulp, except for one carious spot, the removal of which resulted in exposure of the pulp, the cavities were routinely disinfected with 0.12% chlorhexidine solution (Glaxo Smith Kline GmbH, Buhl, Germany). Resolution of bleeding from the exposed pulp in less than 5minutes was considered to be indicative of reversible inflammation The MTA pulp cap was overlaid with a thin protective layer of resin modified glass ionomer cement (Vitrebond; 3M Espe) The reduction in clinical success if a direct pulp capping is not followed immediately with permanent restoration has been shown in other clinical studies (11, 12) The longer the follow-up period, the more evident the trend became to a decline in the success rate of the teeth in the Ca(OH)2 group compared with the MTA group..")
50
SUCCESSFUL PULP CAPS Inflammation management

51
RESIN BIOCOMPATIBILITY??? Volk,J, Engelmann,J.,Leyhausen,G.,Geurtsen,W. Volk,J, Engelmann,J.,Leyhausen,G.,Geurtsen,W. Dental Materials 2006 22:499-505 Dental Materials 2006 22:499-505 Effects of three resin monomers on the cellular glutathione concentration of cultured human fibroblasts Effects of three resin monomers on the cellular glutathione concentration of cultured human fibroblasts See Website: Home>MODXYZ> Biocompatibility See Website: Home>MODXYZ> Biocompatibility ref

52
DYRACT AND DYRACT-CEM AND VITREBOND J Dent Res. 1998 Dec;77(12):2012-9. J Dent Res. 1998 Dec;77(12):2012-9. Residual monomer/additive release and variability in cytotoxicity of light-curing glass-ionomer cements and compomers. Geurtsen W, Spahl W, Leyhausen G. Severe cytotoxic effects were observed in response to both of these materials Mutat Res. 1996 Jul 5;368(3-4):181-94. Mutat Res. 1996 Jul 5;368(3-4):181-94. Genotoxicity of dental materials. Heil J, Reifferscheid G, Waldmann P, Leyhausen G, Geurtsen W. Genotoxic effects were found for Vitrebond and AH 26 (since upgraded to AH26 Plus) Genotoxicity of dental materials. Heil J, Reifferscheid G, Waldmann P, Leyhausen G, Geurtsen W. Genotoxic effects were found for Vitrebond and AH 26 (since upgraded to AH26 Plus)
: Residual monomer/additive release and variability in cytotoxicity of light-curing glass-ionomer cements and compomers. Geurtsen W, Spahl W, Leyhausen G. Severe cytotoxic effects were observed in response to both of these materials Mutat Res Jul 5;368(3-4): Mutat Res Jul 5;368(3-4): Genotoxicity of dental materials. Heil J, Reifferscheid G, Waldmann P, Leyhausen G, Geurtsen W. Genotoxic effects were found for Vitrebond and AH 26 (since upgraded to AH26 Plus) Genotoxicity of dental materials. Heil J, Reifferscheid G, Waldmann P, Leyhausen G, Geurtsen W. Genotoxic effects were found for Vitrebond and AH 26 (since upgraded to AH26 Plus).")
53
GLASS IONOMER BIOCOMPATIBILITY Biomaterials. 1998 Mar;19(6):559-64. Biocompatibility of various light-curing and one conventional glass-ionomer cement. Leyhausen G, Abtahi M, Karbakhsch M, Sapotnick A, Geurtsen W. Two GIs was found to be very biocompatible, while Vitrebond was found to be cytotoxic. Biomaterials. 1998 Mar;19(6):559-64. Biocompatibility of various light-curing and one conventional glass-ionomer cement. Leyhausen G, Abtahi M, Karbakhsch M, Sapotnick A, Geurtsen W. Two GIs was found to be very biocompatible, while Vitrebond was found to be cytotoxic.
: Biocompatibility of various light-curing and one conventional glass-ionomer cement. Leyhausen G, Abtahi M, Karbakhsch M, Sapotnick A, Geurtsen W. Two GIs was found to be very biocompatible, while Vitrebond was found to be cytotoxic..")
54
MTA THERAPIES Indirect Pulp cap (Pink Dentin) Indirect Pulp cap (Pink Dentin) Direct pulp cap (Direct Exposure) Direct pulp cap (Direct Exposure) Pulpotomy (Coronal extirpation) Pulpotomy (Coronal extirpation) Pulpectomy (Coronal and radicular extirpation) Pulpectomy (Coronal and radicular extirpation) Root canal therapy Root canal therapy Perforation repair Perforation repair Apicoectomy Apicoectomy
 Indirect Pulp cap (Pink Dentin) Direct pulp cap (Direct Exposure) Direct pulp cap (Direct Exposure) Pulpotomy (Coronal extirpation) Pulpotomy (Coronal extirpation) Pulpectomy (Coronal and radicular extirpation) Pulpectomy (Coronal and radicular extirpation) Root canal therapy Root canal therapy Perforation repair Perforation repair Apicoectomy Apicoectomy")
55
NEW - BIODENTINE SEPTODONT SEPTODONT $17 PER APPLICATION $17 PER APPLICATION REQUIRES TRITURATOR REQUIRES TRITURATOR IS MEANT TO BE A COMPLETE TEMPORARY FILLING IS MEANT TO BE A COMPLETE TEMPORARY FILLING STICKY HANDLING STICKY HANDLING INDEPENDENT REVIEW YET TO BE SEEN INDEPENDENT REVIEW YET TO BE SEEN

56
PEDODONTIC PULPOTOMY

57
SUCCESSFUL PULP CAPS Seal

58
SEALING THE PULP CAP IMMEDIATE RESTORATION improves prognosis 30% (Mente et al) IMMEDIATE RESTORATION improves prognosis 30% (Mente et al) PROTECT THE CAP from shrinkage PROTECT THE CAP from shrinkage FINAL RESTORATION with low sensitivity technique FINAL RESTORATION with low sensitivity technique CAREFUL OCCLUSION CAREFUL OCCLUSION
 IMMEDIATE RESTORATION improves prognosis 30% (Mente et al) PROTECT THE CAP from shrinkage PROTECT THE CAP from shrinkage FINAL RESTORATION with low sensitivity technique FINAL RESTORATION with low sensitivity technique CAREFUL OCCLUSION CAREFUL OCCLUSION")
59
CAREFUL AND ACCURATE OCCLUSION CAREFUL AND ACCURATE OCCLUSION

60
SUCCESSFUL PULP CAPS Inflammation management

61
INFLAMMATION MANAGEMNT MEDICATION MEDICATION Disciplined use of Ibuprofen 400 mg for 24 hours q4h 6 tabs Disciplined use of Ibuprofen 400 mg for 24 hours q4h 6 tabs Instruct to use regardless if painful or not Instruct to use regardless if painful or not COMMUNICATION COMMUNICATION 1. Cautious prognosis 2. “Call me I want to know” 3. Next day follow-up call 11 am 4. Not that night! 5. Inform that success may be temporary

62
THE END

Similar presentations


























. All rights reserved. Endodontics Chapter 54 Copyright 2003, Elsevier Science (USA). All rights reserved. No part.>")


