Download presentation
Presentation is loading. Please wait.

1
Carotid Artery Revascularization in 2012
James P. Zidar, M.D., F.A.C.C., F.S.C.A.I Clinical Professor of Medicine UNC Health Systems Corporate Chief of Cardiology, Rex Healthcare President, Rex Heart and Vascular Specialists Raleigh, North Carolina

2
Disclosures In the past 5 years, I have been on a scientific advisory board, worked as a consultant for, or conducted clinical research for: Abbott Vascular, Cordis, Medtronic, and Covidien/EV3. All of these companies produce endovascular products including carotid stents, proximal and/or distal filters, and guiding catheters

3
Stroke Carotid arterial disease accounts for a significant minority of CVA Consider other etiologies Rx has improved on all fronts Medical Rx Surgery- CEA Endovascular- CAS

4
Risk of Stroke in Asymptomatic Patients
6 5 4 3 2 1 0-19% 20-29% 30-39% 40-49% 50-59% 60-69% 70-79% 80-89% 90-99% Stroke Incidence (%) Asymptomatic Carotid Artery Stenosis Ulceration increases risk of stroke. 80% of pts with known carotid stenosis will not have warning TIA before stroke. Chambers New England Journal of Medicine. 315(14):860-5, 1986 Norris Stroke. 22(12): , 1991 Mendelsohn & Yadav, Management of Atherosclerotic Carotid Disease, Remedica Publishing, 2000
 Asymptomatic Carotid Artery Stenosis. Ulceration increases risk of stroke. 80% of pts with known carotid stenosis will not have warning TIA before stroke. Chambers New England Journal of Medicine. 315(14):860-5, Norris Stroke. 22(12): , Mendelsohn & Yadav, Management of Atherosclerotic Carotid Disease, Remedica Publishing,")
5
ACE Inhibition Prevents Recurrent Stroke The Progress Trial
6105 subjects with previous stroke randomly assigned to perindopril (n=3051) or placebo (n=3054) PROGRESS Collaborative Group. Lancet 2001:358; 1033 5
 or placebo (n=3054) PROGRESS Collaborative Group. Lancet 2001:358;")
6
SPARCL: High Dose Atorvastatin vs Placebo
In Patients with Prior CVA/TIA Stroke or TIA N Engl J Med 2006;355: 6

7
Asymptomatic carotid stenosis Medical Management
SMART Study 221 patients with >50% carotid stenosis, 5 years <0.5% stroke risk per year Goessens et al. Stroke, 2007 Oxford Vascular Study 101 patients with >50% carotid stenosis, 3 years Marquardt et al. Stroke, 2010

8
Carotid Endarterectomy
Level 1 evidence. Most common major vascular operation. Index vascular procedure. Long-term stroke free survival. LOS, complications, and cost minimized. Established benchmarks.

9
Macro-evolution in CEA outcomes over the past 4 decades
Symptomatic Asymptomatic

10
ACST benefit of intervention with Med Rx over Med Rx alone
Asymptomatic Carotid Surgery Trial Early vs. Deferred CEA in 3120 Asymptomatic Pts with ICA Stenosis Use of Medical Rx ACST benefit of intervention with Med Rx over Med Rx alone Time (years) Lancet 2004;363
 Lancet 2004;363.")
11
Carotid Endarterectomy has improved Perioperative Stroke and Death Reduced
Statins, antiplatelet agents, ace inhibitors, beta blockers, arterial patching Asymptomatic: ACAS 2.7% ACST 2.8% CREST <2% Symptomatic: NASCET 6.5% SPACE 6.3% EVA 3S 3.9% CREST<3.5%

12
SAPPHIRE 723 patients with high risk for CEA RANDOMIZED
>50% stenosis in symptomatic patients >80% stenosis in asymptomatic patients >1 co-morbid condition Team of vascular surgeon, neurologist and interventionalist determined if patient was too high risk for randomization; these patients were entered in a registry and not randomized RANDOMIZED Stenting with protection CEA REGISTRY Surgical Refusal Stent Refusal (n=156) (n=151) (n=409) (n=7) Primary Endpoint 30 day Death, Stroke or MI Yadav et al, NEJM 2004
 (n=151) (n=409) (n=7) Primary Endpoint. 30 day Death, Stroke or MI. Yadav et al, NEJM")
13
SAPPHIRE Randomized events at 30 days
Stent (156) CEA (151) Death 0.6% 2.0% Stroke 3.8% 5.3% 0.6% 2.0% Major 3.2% 3.3% Minor MI 2.6% 7.3% Death/Stroke 4.5% 6.6% Death/ MI/ Stroke 5.8% 12.6% P=0.047 Yadav et al, NEJM 2004
 CEA (151) Death. 0.6% 2.0% Stroke. 3.8% 5.3% 0.6% 2.0% Major. 3.2% 3.3% Minor. MI. 2.6% 7.3% Death/Stroke. 4.5% 6.6% Death/ MI/ Stroke. 5.8% 12.6% P= Yadav et al, NEJM")
15
Carotid Stent Evolution 15 year history
Initial results were discouraging – high morbidity and mortality Technology evolution Embolic protection Better patient selection Large clinical experience Evolution of Clinical Outcomes continues

16
Carotid Artery Stenting in 2012
Early 2000s - Device industry Cordis, Guidant, Boston Scientific, EV3, Medtronic, Abbott Vascular. Developed carotid stent systems including filters and nitinol stents Strategy for approval Patients at high-risk or ineligible for CEA FDA-approved indication versus CMS-approved indications CMS-approved indications don’t match criteria in SAPPHIRE or high-risk registries

17
FDA Approved CAS/EPD systems: 2012
Abbott Acculink stent Accunet filter Abbott EXACT stent Emboshield filter Cordis Precise stent Angioguard filter BSC Next stent EPI Filterwire EV3 Protégé stent Spider filter

18
Carotid Stent Issues AHA guidelines for CEA:
Symptomatic pts : 6% risk of death or major stroke Asymptomatic pts: 3% risk of death/ major stroke High risk vs. low risk for CEA Symptomatic vs asymptomatic pts Initial strategy by multiple companies with various devices targeted CAS for the high risk CEA pt - Clinical – USA, CHF(EF <30%), AS, MR, sev COPD, CABG w/in 6 wks, age >80 yrs. Anatomic – prior CEA, high ICA lesion, prior neck XRT, contralateral occlusion, contralateral laryngeal nerve palsy, severe tandem lesions.
, AS, MR, sev COPD, CABG w/in 6 wks, age >80 yrs. Anatomic – prior CEA, high ICA lesion, prior neck XRT, contralateral occlusion, contralateral laryngeal nerve palsy, severe tandem lesions.")
19
Carotid stent with EPD

20
Debris in filter 12 hr after 6Fr Perclose

21
Abbott Vascular ARCHeR Trial
CAPTURE 1 and 2 CHOICES CREST CANOPY

22
Xact™ Carotid Stent Tapered and Straight
Stent Structure: Closed Cell Shortening: 5-8% Material: Nitinol 0.014” Wire compatible 6F sheath compatible Crossing Profile: 5.7F Stent Matrix Straight: 7, 8, 9, 10 X 20, 30 mm Tapered: 10-8, 9-7, 8-6 X 30, 40 mm TM

23
Shuttle Select Introducer and Slip Cath

24
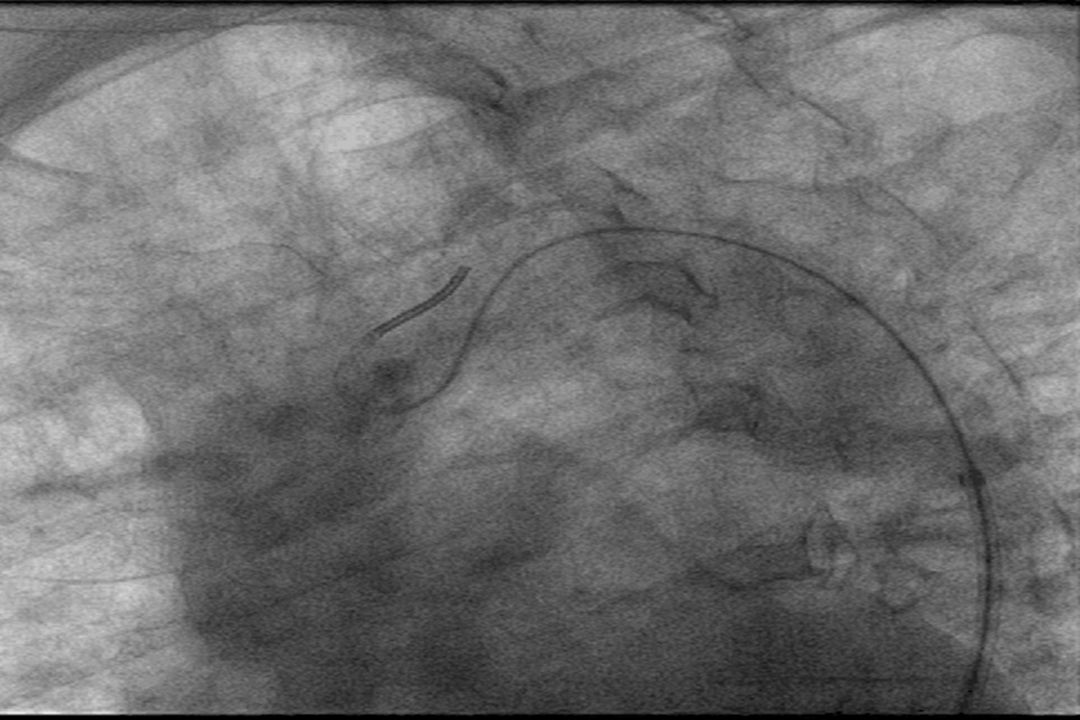
Baseline image 76 wm with mod AS Enrolled in Capture II registry
Lateral or 45 degree ipsilateral oblique are best and/or working view

25
Cranial lateral and Towns views

26
Circle of Willis Anatomy
ACA ACA Left ICA Right ICA Circle w/ aberrant anatomy Right P-Com patent Left P-Com ABSENT (Congenital) A-Com patent When LICA occluded, L MCA territory ischemic supplied only by the RICA via A-Com Therefore, protecting flow in RICA paramount A-COM RMCA LMCA R P-Com patent L P-Com Absent PCA Basilar
 A-Com patent. When LICA occluded, L MCA territory ischemic supplied only by the RICA via A-Com. Therefore, protecting flow in RICA paramount. A-COM. RMCA. LMCA. R P-Com patent. L P-Com Absent. PCA. Basilar.")
27
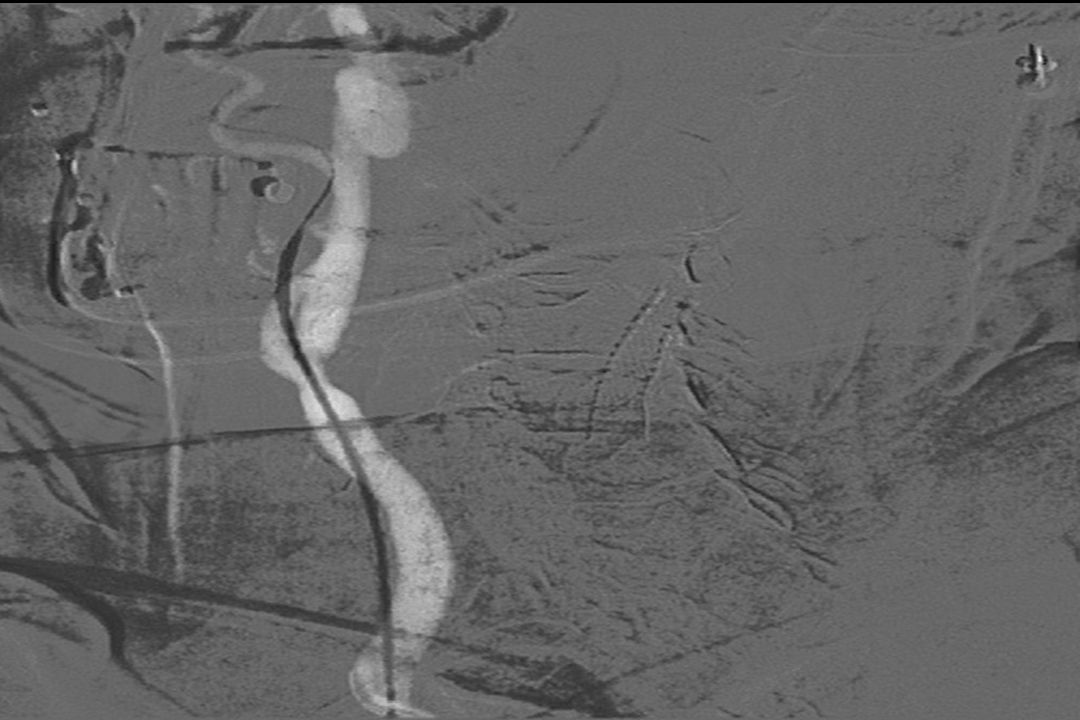
Cerebral Perfusion Post RICA Stent

29
EPDs/ Filters Dominate
Scion BSX/Rubicon MedNova MDT/Interceptor Guidant AccuNet BSX/FilterWire Gen I BSX/FilterWire Gen II MicroVena - Trap Kensey Nash MDT/PercuSurge Abbot/Rubicon - Guardian

30
Emboshield NAV6 Wire moves independent of the filter
Only other filter with this advantage is EV3 Spider filter Improved profile, deliverability Redesigned guide wires Enhanced radiopacity Filter used in the PROTECT Trial Is our data telling us something? Steps in procedure? Timing? USA? Are we focusing in on the right step of the procedure to impact stroke rates the most? Should we be focusing on symptomatics? Elderly? Or is Access prohibiting us from treating these patients effectvely? Training? Access? EPD? Balloon? Stent? Post-Procedural care? Late Strokes?

31
Optimal case selection
Age < 80 Simple, non-calcified aortic arch Lack of lesion Calcification Thrombus String sign No recent major stroke (< 4 weeks) Minimal tortuosity
 Minimal tortuosity.")
32
Carotid Artery Stenting - Procedure
Heparin to ACT >250 sec or bivalirudin Wire lesion and deploy filter Pre-dilate lesion to assess length and diameter – be ready with Atropine…pre-treat if HR <50-60 pre-dilation Neosynephrine ug boluses and drip prn Deploy stent Post-dilate with 5-6 mm balloon Retrieve filter (if slow flow – aspirate filter with Export or long MPA2 prior to retrieval

33
Carotid Artery Stenting - Procedure
May give nitroglycerin if pressure can tolerate for spasm around filter May Buddy wire to preserve lumen if needed when removing filter Neuro checks during and after the procedure (“squeeze ducky”) Monitor blood pressure and HR Aggressive hydration Rx hypotension with Neosynephrine drip and po midodrine
 Monitor blood pressure and HR. Aggressive hydration. Rx hypotension with Neosynephrine drip and po midodrine.")
34
Nervous environment

35
Complications of Carotid Stenting
Access site complications Hypotension/bradycardia Dissection Distal ICA spasm Slow-flow Cerebral embolism, stroke Hyperperfusion syndrome

36
Carotid body stimulation: procedural planning
Recognition of carotid body stimulation aids in management. Occur more frequently at the bifurcation/ostial internal carotid artery in: elderly women heavily calcified vessels Denervation from prior endarterectomy significantly reduces the likelihood of hemodynamic perturbation during stenting. Although not standard outside the cardiovascular laboratory setting, invasive hemodynamic and heart rate monitoring is essential during carotid stent procedures. Intermittent brachial cuff pressures are not satisfactory.

37
Management of carotid body stimulation: bradycardia
Bradycardia is usually transient, even if profound (asystole), and usually resolves quickly with balloon depressurization. Atropine (up to 2 mg) is occasionally required to support further balloon dilation Temporary pacemaker placement---prophylactic or otherwise---is only rarely necessary. Although some operators prefer to pre-treat all patients with atropine, this may occasionally be problematic in the patient with significant coronary disease, and is generally unpleasant. Clues to the need for atropine therapy can usually be discerned by observing the effects of pre-dilation balloon angioplasty
, and usually resolves quickly with balloon depressurization. Atropine (up to 2 mg) is occasionally required to support further balloon dilation. Temporary pacemaker placement---prophylactic or otherwise---is only rarely necessary. Although some operators prefer to pre-treat all patients with atropine, this may occasionally be problematic in the patient with significant coronary disease, and is generally unpleasant. Clues to the need for atropine therapy can usually be discerned by observing the effects of pre-dilation balloon angioplasty.")
38
Management of carotid body stimulation: hypotension
Hypotension can be both rapid and profound during carotid stenting, which can be ameliorated by: Withholding scheduled anti-hypertensive medications that morning Assuring adequate hydration prior to the procedure Avoiding late-day procedures with a patient who has been NPO Using this approach, pre-procedural SBP >180 mmHg are not unusual, and allow a margin of safety during carotid body activation. Hypotension is especially problematic in patients with: Critical AS Severe LV dysfunction Severe/unrevascularized coronary ischemia

39
Management of carotid body stimulation: hypotension
The management of hypotension is straightforward, and should not result in complication Fluid bolus Rapid, albeit brief (5-10 minutes) blood pressure support can be obtained using boluses of: Neosynephrine ( mcg) Metaraminol (Aramine, 0.5 mg) If hypotension is prolonged: Dopamine or other pressor drips Most patients will require no more than hours of support Midodrine 5-10mg po TID for persistent hypotension Early ambulation appears to be helpful in improving blood pressure and restoration of autonomic function.
 blood pressure support can be obtained using boluses of: Neosynephrine ( mcg) Metaraminol (Aramine, 0.5 mg) If hypotension is prolonged: Dopamine or other pressor drips. Most patients will require no more than hours of support. Midodrine 5-10mg po TID for persistent hypotension. Early ambulation appears to be helpful in improving blood pressure and restoration of autonomic function.")
40
Management of neurologic events Know your neuro-interventionalist
Embolic stroke Major stroke/proximal vessel occlusion Intra-arterial thrombolysis (device and pharmacy preparation) Emboli retrieval PTA
 Emboli retrieval. PTA.")
41
Complex Aortic Arch and Vascular Anatomy CAS cases to avoid
Calcified aortic arch Elongated aortic root (Type III) Bovine arch Tandem lesions Tortuous common carotid Poor “landing zones” for EPD’s – think proximal protection Tortuous iliacs
 Bovine arch. Tandem lesions. Tortuous common carotid. Poor landing zones for EPD’s – think proximal protection. Tortuous iliacs.")
42
Type 3 Arch Vitek & Shuttle Select sheath

50
30 Day Event Rates (2000--->2008)
All Stroke - Stenting Trials for High Risk Surgical Patients This is the Bulleted List slide. To create this particular slide, click the NEW SLIDE button on your toolbar and choose the BULLETED LIST format. (Top row, second from left) The Sub-Heading and footnote will not appear when you insert a new slide. If you need either one, copy and paste it from the sample slide. If you choose not to use a Sub-Heading, let us know when you hand in your presentation for clean-up and we’ll adjust where the bullets begin on your master page. Also, be sure to insert the presentation title onto the BULLETED LIST MASTER as follows: Choose View / Master / Slide Master from your menu. Select the text at the bottom of the slide and type in a short version of your presentation title. Click the SLIDE VIEW button in the lower left hand part of your screen to return to the slide show. (Small white rectangle) Factors: embolic protection, experience, case selection 50
 The Sub-Heading and footnote will not appear when you insert a new slide. If you need either one, copy and paste it from the sample slide. If you choose not to use a Sub-Heading, let us know when you hand in your presentation for clean-up and we’ll adjust where the bullets begin on your master page. Also, be sure to insert the presentation title onto the BULLETED LIST MASTER as follows: Choose View / Master / Slide Master from your menu. Select the text at the bottom of the slide and type in a short version of your presentation title. Click the SLIDE VIEW button in the lower left hand part of your screen to return to the slide show. (Small white rectangle) Factors: embolic protection, experience, case selection. 50.")
51
PROTECT: 30-day major adverse events
PROTECT (N=274) Death, Stroke and MI* 1.8% Death 0.4% All Stroke 1.5% Major Stroke Minor Stroke 1.1% MI All Stroke and Death Major Stroke and Death From Lugene: These are confirmed as the correct hierarchy label. The section below is from the statistics discussions From PROTECT sample size decision. The 30-day MAE rate from this trial will be compared to a pre-specified value of 12.0%. The pre-specified level for comparison is based on an examination of the peer-reviewed literature in a similar high-risk patient population (ref. 30-day MAE rates reported from the following trials: SECuRITY, SAPPHIRE, ARCHeR, BEACH, and MAVErIC). Relative to the range of reported 30-day MAE rates from the literature, the pre-specified level of 12.0% is 3.74 percentage points above the maximum reported rate. The difference of 3.74 percentage points represents ~45% of the maximum reported 30-day MAE rate from the literature, and approximately 58% of the arithmetic average 30-day MAE rate reported among all 5 studies. High Risk patients
 Death, Stroke and MI* 1.8% Death. 0.4% All Stroke. 1.5% Major Stroke. Minor Stroke. 1.1% MI. All Stroke and Death. Major Stroke and Death. From Lugene: These are confirmed as the correct hierarchy label. The section below is from the statistics discussions. From PROTECT sample size decision. The 30-day MAE rate from this trial will be compared to a pre-specified value of 12.0%. The pre-specified level for comparison is based on an examination of the peer-reviewed literature in a similar high-risk patient population (ref. 30-day MAE rates reported from the following trials: SECuRITY, SAPPHIRE, ARCHeR, BEACH, and MAVErIC). Relative to the range of reported 30-day MAE rates from the literature, the pre-specified level of 12.0% is 3.74 percentage points above the maximum reported rate. The difference of 3.74 percentage points represents ~45% of the maximum reported 30-day MAE rate from the literature, and approximately 58% of the arithmetic average 30-day MAE rate reported among all 5 studies. High Risk patients.")
52
Cerebral Protection Strategies
Distal Filter Distal flow blockage by ICA Occlusion Flow reversal by proximal CCA and ECA Occlusion, blood shunting into the vein Flow suspension by proximal CCA and ECA Occlusion Filters, Antegrade flow Reverses flow from ICA into femoral vein A-V Shunt Distal flow blockage Flow suspension during CAS 52

56
Advantages of Proximal Protection
Protection starts before crossing lesion & exists during all parts of procedure 24-49% carotid lesions have thrombus TCD HITS during wiring Use any 0.014” wire Less contrast and air to brain No restriction on ICA distal anatomy May be safer for highly embolic lesions

57
(Relative) Requirements for Proximal Protection
Intact ECA on ipsilateral side Collateral support to the Treated Hemisphere CCA and arch anatomy for 9F OD device

58
CREST: Study design Prospective, multicenter, randomized, controlled trial with blinded endpoint adjudication CAS vs. CEA in patients with symptomatic and asymptomatic stenosis 108 US and 9 Canadian sites Rigorous credentialing for CAS operators 427 applicants/ 224 selected (52%) at 110 sites ~1500 patients in lead-in phase
 at 110 sites. ~1500 patients in lead-in phase.")
59
Major Endpoints in CREST
CAS CEA p Periop death/stroke/MI 5.2% 4.5% 0.38 Periop stroke 4.1% 2.3% 0.01 Periop MI 1.1% 0.03 Major periop stroke 0.9% 0.6% 0.52 Cranial nerve palsy 0.3% 4.7% 0.0001

60
CREST Spin Cardiologists: Surgeons: CREST used obsolete technology.
Early in learning curve for CAS. Cranial nerve injuries and MI’s are extremely morbid. Surgeons: Strokes are more likely with CAS than CEA and patients care more about stroke than MI. Most MI’s were minor. Most cranial nerve injuries resolve.

61
30-Day Outcome (Death/Stroke)
Multicenter randomized trials of CAS vs. CEA 30-Day Outcome (Death/Stroke) EVA-3S (30 days) CEA: 3.9% CAS: 9.6% p=0.01 SPACE (30 days) CEA: 6.3% CAS: 6.8% p=0.09 ICSS (120 days) CEA: 4.7% CAS: 8.5% p=0.001 CREST (Symptomatic Only) CEA: 5.4% CAS: 6.7% p=0.30 Trial 61
 EVA-3S (30 days) CEA: 3.9% CAS: 9.6% p=0.01. SPACE (30 days) CEA: 6.3% CAS: 6.8% p=0.09. ICSS (120 days) CEA: 4.7% CAS: 8.5% p= CREST (Symptomatic Only) CEA: 5.4% CAS: 6.7% p=0.30. Trial. 61.")
62
Critical trial construct and conduct issues severely limit the value of EU CEA and CAS outcomes
EPD Use MI Ascertainment Operator Experience EVA-3S + SPACE ½+ ++ ICSS CREST Trial 62

63
CREST outcomes: CEA and CAS are no different for the primary endpoint

64
Any material differences between CEA and CAS in CREST composite endpoints are in minor stroke and MI: PP FDA analysis Per protocol CAS N = 1,131 CEA N = 1,176 Difference Unadjusted p-value* All Death, Stroke, or MI 5.8% (65) 5.1% (60) 0.7% 0.5200 Death 0.53% (6) 0.26% (3) 0.27% 0.3335 Any Stroke 4.1% (46) 1.9% (22) 2.2% 0.0019 Major Stroke 0.9% (10) 0.4% (5) 0.5% 0.2005 Minor Stroke 3.2% (36) 1.5% (18) 1.7% 0.0088 MI 2.0% (22) 3.4% (40) -1.5% 0.0387 * Fisher’s exact p-values were not adjusted for multiple comparisons; p-values for descriptive purposes only Gray et al. Circulation. In press
 5.1% (60) 0.7% Death. 0.53% (6) 0.26% (3) 0.27% Any Stroke. 4.1% (46) 1.9% (22) 2.2% Major Stroke. 0.9% (10) 0.4% (5) 0.5% Minor Stroke. 3.2% (36) 1.5% (18) 1.7% MI. 2.0% (22) 3.4% (40) -1.5% * Fisher’s exact p-values were not adjusted for multiple comparisons; p-values for descriptive purposes only. Gray et al. Circulation. In press.")
65
NIHSS neurological residual deficits from CEA and CAS minor strokes occur with very low frequency and are equal at 6 months ∆ = 0.50% ∆ = 0.02% Gray et al. Circulation. In press 65

66
HR Confidence Interval
Long-term mortality in CREST: No association with minor stroke but strong association with MI Comparison HR HR Confidence Interval Log Rank P-value MI vs. Control 2.81 [ ] 0.0005 Minor Stroke vs. Control 0.52 [0.13 – 2.09] 0.34 MI vs. Minor Stroke 5.18 [1.15 – 23.4] 0.02 Gray et al. Circulation. In press 66

67
No difference between CEA and CAS for the primary composite endpoint by symptomatic or octogenarian status in CREST 95% CL CAS CEA N=599 N=620 N=532 N=556 N=1,025 N=1,073 N=106 N=103 Gray et al. Circulation. In press 67

68
CREST: Fate of CEA cranial nerve injury
CAS N = 1,131 CEA N = 1,176 p-value Procedure related cranial nerve injury 0.0% 5.3% (62/1176) <0.0001 Unresolved at one month 3.6% (42/1176) Unresolved at six months 2.1% (25/1176) Gray et al. Circulation. In press 68
 < Unresolved at one month. 3.6% (42/1176) Unresolved at six months. 2.1% (25/1176) Gray et al. Circulation. In press. 68.")
69
50% Symptomatic Patients Enrollment
Evolutionary outcome improvement for CAS within CREST (not seen with CEA within CREST): Death or any stroke in symptomatic patients 50% Symptomatic Patients Enrollment March 2006 Gray et al. Circulation. In press 69 69
: Death or any stroke in symptomatic patients. 50% Symptomatic Patients Enrollment. March Gray et al. Circulation. In press")
70
Evolutionary outcome improvement for CAS within CREST: Death or major stroke in symptomatic patients
50% Symptomatic Patients Enrollment March 2006 No major strokes or deaths among symptomatic CAS patients in the last half of CREST Gray et al. Circulation. In press 70

71
CAS achieves AHA guidelines in symptomatic patients Large, prospective, multicenter neurologically-audited/independent adjudication single arm studies in high-surgical risk patients N=589 5.3 2.2 1.0 1.4 3.1 1 2 3 4 5 6 7 8 Death/Stroke Death/Major Stroke Death Stroke Minor (3.1%) Stroke Major (1.4%) (%) Subjects EXACT/CAPTURE 2 (>180 sites and 400 operators): 30-day major adverse events symptomatic patients <80 years 6% AHA guideline Hierarchical- Includes only the most serious event for each patient and includes only each patient first occurrence of each event. Gray et al. Circ Cardiovasc Interv Jun;2(3):159-66 71
 Stroke Major (1.4%) (%) Subjects. EXACT/CAPTURE 2 (>180 sites and 400 operators): 30-day major adverse events symptomatic patients <80 years. 6% AHA guideline. Hierarchical- Includes only the most serious event for each. patient and includes only each patient first occurrence of each event. Gray et al. Circ Cardiovasc Interv Jun;2(3):")
72
CEA vs. CAS in symptomatic patients Summary
CAS and CEA are equivalent in primary outcomes and long-term stroke prevention in CREST Large, controlled single arm studies of high surgical risk patients achieve AHA guideline standards European trials flawed and therefore interpretation of primary results limited Significant rapid and continued improvement in outcomes in CAS over past decade; CEA outcomes excellent, plateau’d More wound complication/re-op and cranial nerve injury with CEA

73
What role does CAS play in the standard surgical risk asymptomatic patient?

74
Periprocedural outcomes in CREST: No difference between CAS and CEA for Asx

75
CAS achieves AHA guidelines in asymptomatic patients Large, prospective, multicenter neurologically-audited/independent adjudication single arm studies in high-surgical risk patients N=4282 2.9 1.1 0.8 0.6 1.8 1 2 3 4 5 6 7 8 Death/Stroke Death/Major Stroke Death Stroke Minor (1.8%) Stroke Major (0.6%) (%) Subjects EXACT/CAPTURE 2 (combined): 30-day major adverse events asymptomatic patients <80 years 3% AHA guideline Hierarchical- Includes only the most serious event for each patient and includes only each patient first occurrence of each event. Gray et al. Circ Cardiovasc Interv Jun;2(3):159-66 75
 Stroke Major (0.6%) (%) Subjects. EXACT/CAPTURE 2 (combined): 30-day major adverse events asymptomatic patients <80 years. 3% AHA guideline. Hierarchical- Includes only the most serious event for each. patient and includes only each patient first occurrence of each event. Gray et al. Circ Cardiovasc Interv Jun;2(3):")
76
2011 Multi-Society Guideline Document

77
Managing patients with asymptomatic carotid stenosis: Summary
Asymptomatic carotid stenosis is a risk factor for stroke Surgical revascularization therapy is proven beneficial vs. unmonitored (but probably real world) medical therapy CAS outcomes have demonstrated equivalent outcomes to CEA (CREST), achieved AHA guidelines, and now is Class 2b recommendation in asymptomatic patients (CEA Class 2a) The role of medical therapy remains a tantalizing but unproven alternative to revascularization in patients with established severe carotid stenosis. Until such time as this benefit is demonstrated to be superior, the available randomized controlled data support revascularization in suitable patients
 medical therapy. CAS outcomes have demonstrated equivalent outcomes to CEA (CREST), achieved AHA guidelines, and now is Class 2b recommendation in asymptomatic patients (CEA Class 2a) The role of medical therapy remains a tantalizing but unproven alternative to revascularization in patients with established severe carotid stenosis. Until such time as this benefit is demonstrated to be superior, the available randomized controlled data support revascularization in suitable patients.")
78
CREST: Outcomes by treatment received: SF-36 Physical Component Summary
BG Results of DC clinical Component, the CI are tight, why because there are 1200 patients, separate at 2 weeks and 1 month, related to the surgical incision primarily JACC; Vol. 58, No. 15 ; October 4, 2011:

79
Prospective cost comparison: CEA and CAS SAPPHIRE
CREST MITT Population Difference P-value Per-Protocol Population Difference P-value CAS (n=1212) CEA (n=1193) (95% CI) CAS (n=1136) CEA (n=1184) (95% CI) Cumulative to 1 year $ ± 7730.1 $ ± 9029.8 -$267.2 <.0001 $ ±7527.8 $ ± 9022.9 -$197.8 [ ] [ ] (-939.0,404.6) [ ] [ ] (-875.8,480.1) *MI was reported only when it occurred within 30 days of index procedure
 CEA (n=1193) (95% CI) CAS (n=1136) CEA (n=1184) (95% CI) Cumulative to 1 year. $ ± $ ± $ < $ ± $ ± $ [ ] [ ] (-939.0,404.6) [ ] [ ] (-875.8,480.1) *MI was reported only when it occurred within 30 days of index procedure.")
80
Single de novo ICA lesion +/-involvement of the common carotid artery
Asymptomatic Standard risk for CEA Single de novo ICA lesion +/-involvement of the common carotid artery Stenosis 70% and 99% by angiography or duplex ultrasound Carotid stenting is not currently approved by the FDA for asymptomatic patients who are at standard risk for surgery. CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Confidential: This information is confidential and is intended for distribution to ACT I Study Site participants ONLY. This document contains Abbott Laboratories and Abbott Vascular proprietary information and shall not be duplicated, disclosed to others, or used for purposes other than to carry out the intent for which this material is delivered. ©2010
 law to investigational use. Confidential: This information is confidential and is intended for distribution to ACT I Study Site participants ONLY. This document contains Abbott Laboratories and Abbott Vascular proprietary information and shall not be duplicated, disclosed to others, or used for purposes other than to carry out the intent for which this material is delivered. ©2010.")
81
ACT I: Outcomes Lead-In Patients
Event 30 days, N=180 Death, Stroke and MI 1.7% (3/180) All Stroke and Death 1.7% Major Stroke and Death 0.0% Death All Stroke Major Stroke Minor Stroke MI days, N=157 Ipsilateral Stroke
 All Stroke and Death. 1.7% Major Stroke and Death. 0.0% Death. All Stroke. Major Stroke. Minor Stroke. MI days, N=157. Ipsilateral Stroke.")
82
Final perspectives on CEA and CAS
Outcomes in all are evolving to the positive, and most dramatically for CAS The best data available support that the judicious, expert, and selective use of these therapies which can result in overall improved patient outcomes: Fewer strokes, fewer MI’s Less disability and less CV mortality The equivalence of outcomes of CEA and CAS in CREST bestow complementary, not competitive, roles in the patient requiring revascularization

83
Conclusions Carotid stents are a less invasive alternative to CEA
Hemodynamic perturbations are common in carotid stenting and should be anticipated in pre-procedural planning Preparation of staff, pharmacologic, and mechanical solutions Only rarely should result in a clinically relevant outcome Neurologic events are unusual, and evaluation of the specific syndrome directs management and aids in prognosis

84
Summary : CAS should be applied selectively
High risk factors for CAS: Advanced age Recent symptoms Challenging anatomy CANOPY registry will be revealing: Excludes octogenarians Excludes high risk for CAS--protocol defined Interventionalist criteria are strict and verified Standardized protocol: routinely uses embolic protection, optimal medical therapy

86
Events may occur more than once in the same patient.
CREST: Access complications greater with CEA Per Protocol CAS N = 1,131 CEA N = 1,176 p-value Access Site Complication Requiring Treatment 1.1% 3.7% 0.0001 Patients requiring re-operation Events may occur more than once in the same patient. Other includes pain requiring IV analgesics (5), incision complication (3), pseudoaneurysm (2), occlusion (1) Gray et al. Circulation. In press 86
, incision complication (3), pseudoaneurysm (2), occlusion (1) Gray et al. Circulation. In press. 86.")
87
CREST 4 year primary outcome by age: does the “best fit” line tell the real story?
87

88
Gray et al. Circulation. In press
No age trend in CREST: Hazard Ratio by age group FDA Per protocol analysis CAS=206 CAS=164 CAS=235 CAS=233 CAS=187 CAS=106 CEA=189 CEA=178 CEA=222 CEA=259 CEA=226 CEA=102 Gray et al. Circulation. In press 88

89
Comparative “best fit” line skewed by good CAS outcomes in young patients, and not by poor outcomes in aged 0.39 CAS=206 CAS=164 CAS=235 CAS=233 CAS=187 CAS=106 CEA=189 CEA=178 CEA=222 CEA=259 CEA=226 CEA=102 Gray et al. Circulation. In press 89

90
Be extremely wary of retrospective and meta-analyses of CAS and CEA
Meta-analyses (Murad and others) combining the EU and CREST trials are not possible given the trial conduct issues outlined Retrospective assessments using Medicare and other data bases (McPhee, Sidawy and others) are fatally flawed by virtue of: Selection bias-patients selected for CAS based on high risk qualities Ascertainment bias: only CAS is routinely assessed for neurologic outcomes (almost exclusively done in investigational setting), resulting in 2-3 fold incidence of stroke detection
 combining the EU and CREST trials are not possible given the trial conduct issues outlined. Retrospective assessments using Medicare and other data bases (McPhee, Sidawy and others) are fatally flawed by virtue of: Selection bias-patients selected for CAS based on high risk qualities. Ascertainment bias: only CAS is routinely assessed for neurologic outcomes (almost exclusively done in investigational setting), resulting in 2-3 fold incidence of stroke detection.")
91
Macro-evolution in CAS outcomes demonstrating remarkable progression in past decade
MAE in high risk carotid stent IDE trials: (n>4000)
")
92
Management of hypertension
Howell et al. J Endovasc Ther 2002 Dec; 9(6): 810-6 Cerebral hemorrhage may result from uncontrolled BP, which may result from withholding medication to allow for carotid body stimulation Data from one small (n=60) study suggests that both the absolute degree of BP drop, as well as a higher opening pressure, are predictive of instability TCD increases in flow (>150% baseline) are related to increased risk of hemorrhage (CEA data) Aggressive control of BP with IV/PO medication (e.g., beta-blockers, nitroprusside, nicardipine) is important post-procedure, especially in at risk patients. Headache from IV NTG may confound the issue of cerebral hemorrhage
: Cerebral hemorrhage may result from uncontrolled BP, which may result from withholding medication to allow for carotid body stimulation. Data from one small (n=60) study suggests that both the absolute degree of BP drop, as well as a higher opening pressure, are predictive of instability. TCD increases in flow (>150% baseline) are related to increased risk of hemorrhage (CEA data) Aggressive control of BP with IV/PO medication (e.g., beta-blockers, nitroprusside, nicardipine) is important post-procedure, especially in at risk patients. Headache from IV NTG may confound the issue of cerebral hemorrhage.")
93
Receptor activation in carotid sinus stimulation
Hypotension Chen-Scarabelli, C. et al. BMJ 2004;329:

94
CREST: Quality of life by event
Impact of peri-procedural events (stroke/MI) on SF-36 at 1 year adjusting age, sex, symptomatic cerebrovascular disease and baseline SF-36 measures – Growth Curve Modeling 94
 on SF-36 at 1 year adjusting age, sex, symptomatic cerebrovascular disease and baseline SF-36 measures – Growth Curve Modeling. 94.")
Similar presentations












, PhD(Lond.), FEBVS Professor of Vascular Surgery Chairman, Dept. of Vascular Surgery,>")



 Programme (project number 06/301/233) and.>")







>")





