Download presentation
Presentation is loading. Please wait.

2
Cortically OriginatedMovement Cortically Originated Movement I. Motor Tract (corticospinal tractus) Extrapyramidal System (basal ganglia) Cerebellum Praxis Circuits II. Motor Tract : Alpha motor neurons of spinal cord Neurons of the brain stem cranial nerve nuclei Peripheral nerve Neuromuscular junction Muscle
 Extrapyramidal System (basal ganglia) Cerebellum Praxis Circuits II. Motor Tract : Alpha motor neurons of spinal cord Neurons of the brain stem cranial nerve nuclei Peripheral nerve Neuromuscular junction Muscle.")
3
B Basal ganglia: caudate putamen & globus pallidus caudate, putamen (collectively called striatum), globus pallidus (and putamen collectively called nucleus lentiformis) corpus striatum refers to the caudate putamen & globus pallidus caudate putamen globus pallidus Thalamus Subthalamic nucleus interna externa
, globus pallidus (and putamen collectively called nucleus lentiformis) corpus striatum refers to the caudate putamen & globus pallidus caudate putamen globus pallidus Thalamus Subthalamic nucleus interna externa")
4
Substantia nigrareticulatacompacta Substantia nigra is a dopaminergic structure in the mesensephalon Striatum is a “primary input” Gpi & SNr are “Output” structures c r

5
Functions of the Basal Ganglia Motor function: Motor & oculomotor circuits play an important role in the regulation and coordination of cortically originated movement Cognitive function: Prefrontal circuits Emotional function: Limbic circuits

6
somatomotor işlevler somatomotor işlevler göz küresi hareketleri bilişsel işlevler emosyonel işlevler

8
Disorders of the Basal Ganglia and the Extrapyramidal System Manifested by contralateral involuntary movements that characteristically disappears in sleep (except tics) Two types of movements are associated with BG: Hyperkinetic, characterized by excessive involuntary movements such as seen in chorea, athetosis, ballism, dystonia, and motor tics Hypokinetic (bradykinetic), characterized by paucity of movement, or by difficulty in initiation of movement (akinesia) as seen in Parkinson’s Disease
 Two types of movements are associated with BG: Hyperkinetic, characterized by excessive involuntary movements such as seen in chorea, athetosis, ballism, dystonia, and motor tics Hypokinetic (bradykinetic), characterized by paucity of movement, or by difficulty in initiation of movement (akinesia) as seen in Parkinson’s Disease")
9
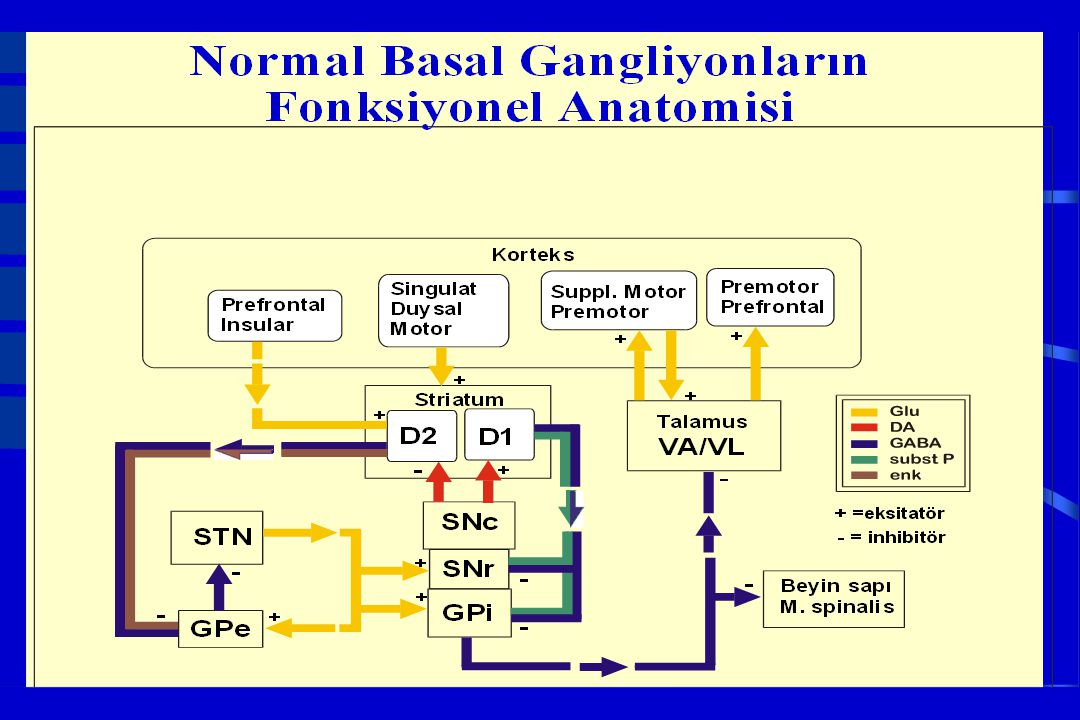
Parkinson Hastalığı Fonksiyonel Anatomisi + + + + + - -

11
STRIATUM CEREBRAL CORTEX Glutamate D1 Substance P D2ENKEPHALINE Acetyl Choline SS GABA Glutamate GPi/SNr GABA SNc Spinal cord & Brain Stem GABA Glutamate Glutamate DOPAMINE GPe GABA GABA STN Glutamate PPN VA/VL THALAMUS Glutamate Glutamate GABA Glutamate GABA Glutamate Glutamate Glutamate NORMAL MOTOR CIRCUIT

12
Signs & Symptoms of Parkinson’s Disease Cardinal Characteristics Cardinal Characteristics Resting tremor Resting tremor Bradykinesia Bradykinesia Rigidity Rigidity Postural instability Postural instability At least two of the first three Absence of a secondary cause Definitive diagnosis by autopsy Response to levodopa Masked face Masked face Hypophonic speech Hypophonic speech Sialorrhea Sialorrhea Micrographia Micrographia Slowing of Activities of Daily Livings Slowing of Activities of Daily Livings Difficulty arising from a chair Difficulty arising from a chair Stooped, shuffling gait with Stooped, shuffling gait with decreased arm swing decreased arm swing Difficulty turning in bed Difficulty turning in bed Loss of the sense of smell Loss of the sense of smell Foot dystonia Foot dystonia

15
SEREBRAL KORTEKS Glu D1 Substance P D2/ENKEPHALINEDYNORPHINE Acetylcholine SS GABA Glu GPi/SNr GABA SNc Spinal cord Spinal cord& Brain stem GABA Glutamate GPe STN GABA VA/VLTHALAMUS Glu GABA Glutamate GABA GABA DOPAMINE BASAL GANGLIA MOTOR CIRCUIT IN PARKINSON’S DISEASE STRİATUM

16
At death, DOPAMINE loss > 90% At death, DOPAMINE loss > 90% <50% DOPAMINE loss: asymptomatic ~70% DOPAMINE loss: symptom manifestations Severity of DA loss best correlates with bradykinesia in PD

17
Cause of PD Cause of PD Unknown in most cases; not accelerated aging Unknown in most cases; not accelerated aging Genes Genes AD inheritance very rare; mutation ? AD inheritance very rare; mutation ? Mutation of Alpha synuclein gene (chr 4q) identified in one large Italian (Contursi) and 5 Greek AD families Mutation of Alpha synuclein gene (chr 4q) identified in one large Italian (Contursi) and 5 Greek AD families Mutation of parkin gene in AR juvenile parkinsonism Mutation of parkin gene in AR juvenile parkinsonism Environment Environment Majority of cases believed caused by environmental factor (s) but none identified so far Majority of cases believed caused by environmental factor (s) but none identified so far Genes plus environment? Genes plus environment?
 identified in one large Italian (Contursi) and 5 Greek AD families Mutation of Alpha synuclein gene (chr 4q) identified in one large Italian (Contursi) and 5 Greek AD families Mutation of parkin gene in AR juvenile parkinsonism Mutation of parkin gene in AR juvenile parkinsonism Environment Environment Majority of cases believed caused by environmental factor (s) but none identified so far Majority of cases believed caused by environmental factor (s) but none identified so far Genes plus environment. Genes plus environment .")
18
AdıLokusGenKalıtım şekliSıklığı Fenotip PARK1*4q21-23 A53T E46K A30P -sinuklein SNCA dominant15 aile HBY<45, demans HBY>45 PARK26q25.20-27Parkin, PRKN resesif%10-20 ;<50y Jüvenil, DT, uyku! PARK32p13?dominantbirçok aile Tipik PH PARK4*4q21-23 -sinuklein dup/triplik. dominantIowa ailesi PH, ET, LCD PARK54p14UCH-L1dominant1 aile PH PARK61p35-36PINK1resesifbirçok aile HBY erken, PH PARK71p36DJ-1resesif% 2; < 45 yaş HBY erken PARK8* 12p11.2-q13.1 LRRK2dominantbirçok aile Tipik PH PARK9*1p36ATP13A2dominant1 aile PARK101p32?dominantbirçok aile PARK 112q36-37?dominant65 aile PARK 12X q21-25?X’e bağlı, sporadik Mizuno,2008 PARK 132p13Omi/HtrA2dominant *: Lewy cisimciği saptanır

19
Hypotheses of SN Pathogenesis Apoptosis; mitochondrial? Apoptosis; mitochondrial? oxidative stress, antioxidant capacity oxidative stress, antioxidant capacity iron in neuromelanin, free radical formation iron in neuromelanin, free radical formation complex I and glutathione in SNc complex I and glutathione in SNc Slow or weak excitotoxicity Slow or weak excitotoxicity ATP loss Membrane potential decline persistent activation of NMDA receptors Ca influx, NO, superoxide, peroxynitrite formation ATP loss Membrane potential decline persistent activation of NMDA receptors Ca influx, NO, superoxide, peroxynitrite formation Inadequate neurotrophic factor(s) Inadequate neurotrophic factor(s)
 Inadequate neurotrophic factor(s).")
20
Preclinical Parkinson’s Disease No specific clinical markers known No specific clinical markers known PET studies may identify preclinical cases PET studies may identify preclinical cases 4-13% of autopsies in elderly showing incidental Lewy bodies are regarded as preclinical cases 4-13% of autopsies in elderly showing incidental Lewy bodies are regarded as preclinical cases Increased risk of neuroleptic parkinsonism Increased risk of neuroleptic parkinsonism Duration of preclinical phase unknown (several years to several decades?) Duration of preclinical phase unknown (several years to several decades?)
 Duration of preclinical phase unknown (several years to several decades )")
21
Clues Suggesting Atypical Parkinsonism Early onset of, or rapidly progressing, dementia Early onset of, or rapidly progressing, dementia Rapidly progressive course Rapidly progressive course Supranuclear gaze palsy Supranuclear gaze palsy Upper motor neuron signs Upper motor neuron signs Cerebellar signs—dysmetria, ataxia Cerebellar signs—dysmetria, ataxia Urinary incontinence Urinary incontinence Early symptomatic postural hypotension Early symptomatic postural hypotension

22
Parkinson’s disease Parkinson-plus syndrome Drug-induced parkinsonism Nigral Dopaminergic Neuron Terminals and Striatal Receptors

23
Causes of Parkinsonism Neurodegenerative disorders with Parkinsonism Neurodegenerative disorders with Parkinsonism Hereditary disorders associated with parkinsonism Hereditary disorders associated with parkinsonism Secondary Parkinsonism Secondary Parkinsonism Drug-Induced Parkinsonism Drug-Induced Parkinsonism Metabolic, Infectious and Toxic Causes of Parkinsonism Metabolic, Infectious and Toxic Causes of Parkinsonism Structural Lesions Causing Parkinsonism Structural Lesions Causing Parkinsonism Vascular Parkinsonism Vascular Parkinsonism

24
Multiple system atrophy Multiple system atrophy Shy-Drager syndrome: MSAa Shy-Drager syndrome: MSAa Autonomic insufficiency: orthostasis, impotence Striatonigral degeneration: MSAp Striatonigral degeneration: MSAp Tremor less prominent Olivopontocerebellar atrophy: MSAc Olivopontocerebellar atrophy: MSAc Cerebellar signs Neurodegenerative disorders with Parkinsonism

25
Progressive supranuclear palsy Progressive supranuclear palsy Supranuclear downgaze palsy, square wave jerks Supranuclear downgaze palsy, square wave jerks Upright posture/frequent falls Upright posture/frequent falls Pseudobulbar emotionality Pseudobulbar emotionality Furrowed brow/stare Furrowed brow/stare Corticobasal degeneration Corticobasal degeneration Unilateral, coarse tremor Unilateral, coarse tremor Limb apraxia/limb dystonia/alien limb Limb apraxia/limb dystonia/alien limb

27
Diffuse Lewy body disease Diffuse Lewy body disease Early onset of dementia Early onset of dementia Delusions and hallucinations Delusions and hallucinations Agitation Agitation Alzheimer’s disease Alzheimer’s disease Dementia is the primary clinical syndrome Dementia is the primary clinical syndrome Rest tremor is rare Rest tremor is rare Neurodegenerative disorders with Parkinsonism

28
Hereditary Disorders Associated with Parkinsonism Wilson’s disease Wilson’s disease Huntington’s disease Huntington’s disease Dentatorubro-pallidoluysian atrophy (DRPLA) Dentatorubro-pallidoluysian atrophy (DRPLA) Machado-Joseph disease (SCA-3) Machado-Joseph disease (SCA-3)
 Dentatorubro-pallidoluysian atrophy (DRPLA) Machado-Joseph disease (SCA-3) Machado-Joseph disease (SCA-3)")
29
Drug-Induced Parkinsonism Most cases are reversible Careful medication history—list drug names Careful medication history—list drug names Treatment: Stop offending medication Treatment: Stop offending medication Common offending drug types Common offending drug types Antipsychotics Antipsychotics haloperidol, chlorpromazine, thioridizine, perphenazine haloperidol, chlorpromazine, thioridizine, perphenazine risperidone, olanzapine risperidone, olanzapine Antiemetics metoclopramide, prochlorperazine Antiemetics — metoclopramide, prochlorperazine Dopamine depletors methyldopa, reserpine, tetrabenazine Dopamine depletors — methyldopa, reserpine, tetrabenazine Combination drugs amitriptyline, perphenazine Combination drugs — amitriptyline, perphenazine

30
Metabolic, Infectious and Toxic Causes of ParkinsonismMetabolic, Infectious and Toxic Causes of Parkinsonism Metabolic Metabolic Often reversible Often reversible Hypo- or hyper-thyroidism Hypo- or hyper-thyroidism Hypo- or hyper-parathyroidism Hypo- or hyper-parathyroidism Liver failure Liver failure Central pontine myelinolysis Central pontine myelinolysis Infectious Infectious Post-encephalitic Post-encephalitic Creutzfeldt-Jakob disease Creutzfeldt-Jakob disease Infectious masses Infectious masses HIV HIV MPTP Carbon monoxide Manganese Cyanide Toxin-induced Toxin-induced

31
Structural Lesions Causing Parkinsonism Acute or subacute onset Acute or subacute onset Other signs: hemiparesis, hyperreflexia, aphasia, sensory loss, seizures Other signs: hemiparesis, hyperreflexia, aphasia, sensory loss, seizures Brain tumor Brain tumor Infectious mass Infectious mass Aneurysm Aneurysm Hydrocephalus: Hydrocephalus: gait disorder/dementia urinary/fecal incontinence urinary/fecal incontinence

32
Vascular Parkinsonism Abrupt onset, usually unilateral Abrupt onset, usually unilateral Step-wise or no progression Step-wise or no progression Other signs—hemiparesis, aphasia, hyperreflexia Other signs—hemiparesis, aphasia, hyperreflexia Infarcts on neuroimaging helpful in confirming diagnosis Infarcts on neuroimaging helpful in confirming diagnosis

33
Tremor An involuntary An involuntary Rhythmic Rhythmic Oscillatory Oscillatory Sinusoidal movement of Sinusoidal movement of a part or parts of the body a part or parts of the body Produced by contractions of Alternating or Alternating or Synchronous antagonist muscles Synchronous antagonist muscles

34
Classification of Tremor Rest: PD, PD+, secondary, severe ET, Rest: PD, PD+, secondary, severe ET, myorhytmia, midbrain myorhytmia, midbrain Action: PD, ET, midbrain, dystonic, Action: PD, ET, midbrain, dystonic, neuropathic neuropathic Postural: Physiologic, ET, PD, midbrain, dystonic, stress Postural: Physiologic, ET, PD, midbrain, dystonic, stress Kinetic: (Initial, Dynamic, Terminal) Kinetic: (Initial, Dynamic, Terminal) Cerebellar, midbrain, Wilson Cerebellar, midbrain, Wilson Task- or position-specific: writing Task- or position-specific: writing Isometric Isometric
 Kinetic: (Initial, Dynamic, Terminal) Cerebellar, midbrain, Wilson Cerebellar, midbrain, Wilson Task- or position-specific: writing Task- or position-specific: writing Isometric Isometric")
35
Classification of Tremor Based on Relative Frequency (Hz) Frequency in Hz 2.4 - 4.0 4.0 - 4.5 5.5 - 7.0 7.0 - 12.0 Typical Etiology Cerebellar, “ataxic” (brainstem,MS) PD (rest), rubral, neuroleptic-induced ET, PD (postural), drug (VPA), voluntary Physiological, exaggerated physiologic, drug induced (e.g., epinephrine)
 Frequency in Hz Typical Etiology Cerebellar, ataxic (brainstem,MS) PD (rest), rubral, neuroleptic-induced ET, PD (postural), drug (VPA), voluntary Physiological, exaggerated physiologic, drug induced (e.g., epinephrine)")
36
Criteria for Essential Tremor Criteria for Essential Tremor Bilateral action, but not rest tremor of the hands and forearms Absence of other neurologic signs with the exception of the cogwheel phenomenon May have isolated head tremor with no abnormal posture

37

39
Parkinson’s Disease vs. Essential Tremor Essential tremor consists of tremor in head, hands & voice with no other signs of parkinsonism Essential tremor consists of tremor in head, hands & voice with no other signs of parkinsonism Cogwheel rigidity can be found in ET Cogwheel rigidity can be found in ET Both can have a postural & rest component Both can have a postural & rest component Kinetic tremor can interfere with ADL in ET Kinetic tremor can interfere with ADL in ET (+) family history in 50 % of ET cases (+) family history in 50 % of ET cases
 family history in 50 % of ET cases (+) family history in 50 % of ET cases.")
40
40 Parkinson hastalığıEsansiyel tremor Yaş40-75Her yaş TremorStatik ± postüralPostüral (± statik) Frekans (Hz)4 - 67 - 9 Tutulan uzuvlarEl, kol, ayak, bacak, dil, dudak, çene El, kol, ayak, bacak, baş, ses Mental akt.+- Kalıtım~ % 5% 50 (OD) Alkole yanıt-+ Parkinson bulguları +Senkinetik rijidite Hastalık seyriİlerleyiciStasyoner TedaviAntiparkinson ilaçlar, cerrahi -bloker, pirimidon, benzodiazepin, cerrahi
 Frekans (Hz) Tutulan uzuvlarEl, kol, ayak, bacak, dil, dudak, çene El, kol, ayak, bacak, baş, ses Mental akt.+- Kalıtım~ % 5% 50 (OD) Alkole yanıt-+ Parkinson bulguları +Senkinetik rijidite Hastalık seyriİlerleyiciStasyoner TedaviAntiparkinson ilaçlar, cerrahi -bloker, pirimidon, benzodiazepin, cerrahi")
41
Dystonia Alterations in muscle tone Alterations in muscle tone Sustained abnormal postures Sustained abnormal postures Disruptions of ongoing movement Disruptions of ongoing movement

42
Distoninin Fizyopatolojisi PET PET*DYT1taşıyıcılarında lentiform nük. lentiform nük. serebellum serebellum suplemanter motor kortekste artmış aktivite artmış aktivite *DYT1hastalarında talamus talamus serebellum serebellummezensefalonda metabolikgösterir çalışmaları

43
Dystonias by body distribution of symptoms -Focal - Focal - Segmental *Cranial *Axial *Brachial *Crural *Brachial *Crural - Multifocal - Generalized - Hemidystonia

45
kkkk Birçok hastada bu postürler birarada görülür

46
Primary Dystonias by age of onset Childhood Adolescence Childhood Adolescence Adulthood Onset Inherited defect + + + or sporadic Inherited defect + + + or sporadic GeneDYT1 DYT2, DYT4 (9q34, GAG deletion) DYT6, DYT7 GeneDYT1 DYT2, DYT4 (9q34, GAG deletion) DYT6, DYT7 Initially involved parts foot/arm foot/arm upper parts Symptoms during activities: running/walking Progression 50-90 % generalized focal focal Ages <28 30-50 Penetrance %30-40 ~%25
 DYT6, DYT7 GeneDYT1 DYT2, DYT4 (9q34, GAG deletion) DYT6, DYT7 Initially involved parts foot/arm foot/arm upper parts Symptoms during activities: running/walking Progression % generalized focal focal Ages < Penetrance %30-40 ~%25")
47
Dystonia classified by etiology Primary Primary Dystonia plus: Dopa-Responsive, Paroxysmal, X-Linked Dystonia- Parkinsonian, Myoclonic, and Rapid-Onset Dystonia-Parkinsonian Dystonia plus: Dopa-Responsive, Paroxysmal, X-Linked Dystonia- Parkinsonian, Myoclonic, and Rapid-Onset Dystonia-Parkinsonian Secondary (birth injury, trauma, toxins, stroke or in association with Wilson's disease) Secondary (birth injury, trauma, toxins, stroke or in association with Wilson's disease)
 Secondary (birth injury, trauma, toxins, stroke or in association with Wilson s disease)")
48
Secondary forms of dystonia arise from and can be attributed to numerous causes arise from and can be attributed to numerous causes birth injury, trauma, toxins or stroke birth injury, trauma, toxins or stroke can be symptomatic can be symptomatic also occur in association with other also occur in association with other disorders such as Wilson's disease disorders such as Wilson's disease MRI/CAT scans may show structural lesions

50
Merrit’s Neurology, 2000 Sekonder Distoni İşaretleri Merrit’s Neurology, 2000 Etyolojik faktör öyküsü : Etyolojik faktör öyküsü : travma (kafa/periferik), ansefalit, toksine maruz kalma, doğumda anoksi travma (kafa/periferik), ansefalit, toksine maruz kalma, doğumda anoksi Nörolojik anormallik bulgusu: demans, nöbetler, ataksi, parezi, spastisite, amiyotrofi, göz bulgusu, parkinsonizm Nörolojik anormallik bulgusu: demans, nöbetler, ataksi, parezi, spastisite, amiyotrofi, göz bulgusu, parkinsonizm İstirahatte başlama İstirahatte başlama Konuşma bozukluğunun erken başlaması Konuşma bozukluğunun erken başlaması Hemidistoni, erişkinde bacak distonisi Hemidistoni, erişkinde bacak distonisi Anormal beyin görüntülemesi, lab. bulgusu Anormal beyin görüntülemesi, lab. bulgusu Yalancı güçsüzlük vs. gibi psikojen ety. Yalancı güçsüzlük vs. gibi psikojen ety.

51
Distoniye Yol Açan Heredodejeneratif Hastalıklar Weiner WJ, Lang AE. Mov. Disord 1989 Metabolik Bozukluklar Wilson hastalığı Aminoasidüriler Metakromatik lökodistrofi Seroid lipofüsinozis Jüvenil distonik lipidoz Gangliyosidozlar Lesch-Nyhan sendromu Leigh hastalığı Mitokondriyel hastlalıklar Ailevi bazal gangliyon kalsifik. Dejeneratif Bozukluklar Parkinson hastalığı Mültipl sistem atrofi Huntington hastalığı PSF Kortikobazal gang.dej. Lubag Pallidal dejenerasyon Hallervorden Spatz Nöroakantositoz Ataksi telanjiektazi Hızlı başlayan distoni- parkinsonizm

52
Lesions of Subthalamic Nucleus decreased Gpi/SNr activity decreased inhibition on VA/VL thalamus increased thalamocortical excitation Chorea / Ballismus

53
Korenin Oluş Mekanizması Korteks k Direkt yol T Kaudat / subtalamik çekirdeklerin işlev bozukluğu İndirekt yolda striatum- dan GPe üzerine olan inhibitör etki azalır GPe serbestleşir, STN’u aşırı inhibe eder STN veri çıkış merkezle-rini yeterince uyaramaz ve talamus baskılanamaz Talamus istemsiz hareketleri gereği kadar inhibe edemez Korteks aşırı uyarılır İndirekt yol Hareket örneği jeneratörü

54
Patients with Patients with Huntington’s Disease CHOREA: brief, purposeless involuntary movements of the distal extremities and face, which may merge imperceptibly into purposeful or semipurposeful acts that mask the involuntary motion

55
Huntington’s Disease CORTEX PUTAMEN GP externa STN GP interna VA&VL THALAMUS Glutamat e(+) GABA (-) Glutamate (+) GABA (-) Glutamate(+) +
 GABA (-) Glutamate (+) GABA (-) Glutamate(+) +")
56
Athetosis writhing movements, often with alternating postures of the proximal limbs that blend continuously into a flowing stream of movement writhing movements, often with alternating postures of the proximal limbs that blend continuously into a flowing stream of movement

57
Chorea: etiology Chorea: etiology Sydenham’s chorea Chorea gravidarum Heredodegenerative Huntington’s disease Benign hereditary chorea Wilson’s disease Paroxysismal choreoathetosis Familial chorea-achantositosis Cerebral palsy ( perinatal anoxia, hemorrage, kernicterus,.) Drugs related ( Li, DPH, L-dopa, contraceptives, neuroleptics) Lesions of subthalamic nuc. Cerebrovascular disorders (vasculitis, ischemic/hemorragical stroke, subdural hematoma) Various medical conditions Thyrotoxicosis Hypoparathyroidism Addison’s disease Hypocalcemia Hypomagnesemia Polycitemia vera Hepatic cirrosis SLE Encephalitis lethargica Aminoff, Greenberg, Simon. Clin Neurol,1996
 Various medical conditions Thyrotoxicosis Hypoparathyroidism Addison’s disease Hypocalcemia Hypomagnesemia Polycitemia vera Hepatic cirrosis SLE Encephalitis lethargica Aminoff, Greenberg, Simon. Clin Neurol,1996.")
58
Hemiballismus Hemiballismus Violent, continuous proximal limb flinging movements confined to one side of the body, usually affecting the arm more than the leg Violent, continuous proximal limb flinging movements confined to one side of the body, usually affecting the arm more than the leg It is caused by a lesion, usually an infarct, in the region of the contralateral subthalamic nucleus of Luys It is caused by a lesion, usually an infarct, in the region of the contralateral subthalamic nucleus of Luys

60
Myoclonus Myoclonus brief, lightning-like contraction of a muscle or group of muscles Physiological: -Nocturnal myoclonus (falling asleep) -Hiccup (singultus): diaphragmatic muscles affected Metabolic: uremia Neurodegenerative: Alzheimer's disease/ progressive myoclonic epilepsy Slow virus infections: Creutzfeldt-Jakob disease subacute sclerosing panencephalitis Closed head trauma, hypoxic-ischemic brain injury: action myoclonus increases with intended movement Lesion in dentato-olivocerebellar circuit: Palatal mycl due to contraction of posterior pharyngeal muscles
 -Hiccup (singultus): diaphragmatic muscles affected Metabolic: uremia Neurodegenerative: Alzheimer s disease/ progressive myoclonic epilepsy Slow virus infections: Creutzfeldt-Jakob disease subacute sclerosing panencephalitis Closed head trauma, hypoxic-ischemic brain injury: action myoclonus increases with intended movement Lesion in dentato-olivocerebellar circuit: Palatal mycl due to contraction of posterior pharyngeal muscles")
61
TICS Brief, rapid, simple or complex involuntary movements that are stereotypical and repetitive, but not rhythmic Brief, rapid, simple or complex involuntary movements that are stereotypical and repetitive, but not rhythmic Simple tics (eg, blinking) often begin as nervous mannerisms in childhood or later and disappear spontaneously. Complex tics often resemble fragments of normal behavior. Simple tics (eg, blinking) often begin as nervous mannerisms in childhood or later and disappear spontaneously. Complex tics often resemble fragments of normal behavior. Tourette Syndrome (Gilles de la Tourette's Syndrome) Tourette Syndrome (Gilles de la Tourette's Syndrome) An inherited multiple tic disorder that begins in childhood An inherited multiple tic disorder that begins in childhood
 often begin as nervous mannerisms in childhood or later and disappear spontaneously. Complex tics often resemble fragments of normal behavior. Tourette Syndrome (Gilles de la Tourette s Syndrome) Tourette Syndrome (Gilles de la Tourette s Syndrome) An inherited multiple tic disorder that begins in childhood An inherited multiple tic disorder that begins in childhood.")
63
Gilles de la Tourette Bozukluğu Tanı Kriterleri (DSM-IV) Eşzamanlı olmayabilen hem çoğul motor, hem de bir/birden fazla vokal tikler ortaya çıkar Tikler 1yıl< süre aralıklı/~her gün/günde birçok kez oluşur, ardışık 3 ay< tiksiz bir dönem yoktur Tiklerin yeri, sayısı, sıklığı, karmaşıklığı, şiddeti zamanla değişir Başlangıç <18 yaş Psikoaktif bir maddenin (stimülanlar) fizyolojik etkilerine bağlı, Huntington hast./post-viral ansefalit gibi bir MSS hastalığı sırasında değildir Sıkıntıya ve toplumsal, mesleki ve diğer önemli işlevsellik alanlarında belirgin bir bozulmaya neden olur
 Eşzamanlı olmayabilen hem çoğul motor, hem de bir/birden fazla vokal tikler ortaya çıkar Tikler 1yıl< süre aralıklı/~her gün/günde birçok kez oluşur, ardışık 3 ay< tiksiz bir dönem yoktur Tiklerin yeri, sayısı, sıklığı, karmaşıklığı, şiddeti zamanla değişir Başlangıç <18 yaş Psikoaktif bir maddenin (stimülanlar) fizyolojik etkilerine bağlı, Huntington hast./post-viral ansefalit gibi bir MSS hastalığı sırasında değildir Sıkıntıya ve toplumsal, mesleki ve diğer önemli işlevsellik alanlarında belirgin bir bozulmaya neden olur")
64
Wilson’s disease OR OR 13q14.3 yerleşimli gen 13q14.3 yerleşimli gen 27 mütasyon 27 mütasyon P-type Cu transporter ATPase synthesis defect P-type Cu transporter ATPase synthesis defect Prevalance: 30/1 million Prevalance: 30/1 million Age-onset ~21 Age-onset ~21 Liver, neurologic, psychiatric and renal involvement Liver, neurologic, psychiatric and renal involvement Kayser-Fleischer ring Parkinsonism Tremor Rigidity Dysarthria Dysphagia Sialorrhea Dystonia Coordination is disturbed Gait disorder Eye movements dysfunction Renal tubular necrosis (Fanconi syndrome) Gilroy. Basic Neurology, 2000 Adler, Ahlskog. PD&Mov Disord. 2000

Similar presentations















.>")













: Largest, also referred to as Type I. Beta (β): Also referred to as.>")
 frontal lobe. B. Parallel circuits C. Neurotransmitters.>")