Download presentation
Presentation is loading. Please wait.

1
Approach to Pleural Effusion
MED 341 Ahmed BaHammam Professor of Medicine Pulmonary Unit & Sleep Disorders Center KSU

2
Up to 25 ml of pleural fluid is normally present in the pleural space, an amount not detectable on conventional chest radiographs.

3
Development of Pleural Effusion
pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia) pleural membrane permeability (malignancy) lymphatic obstruction (malignancy) diaphragmatic defect (hepatic hydrothorax) thoracic duct rupture (chylothorax)
 capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia) pleural membrane permeability (malignancy) lymphatic obstruction (malignancy) diaphragmatic defect (hepatic hydrothorax) thoracic duct rupture (chylothorax)")
4
Pleural Effusion Pleural effusion is an abnormal accumulation of fluid in the pleural space. The 5 major types of pleural effusion are: Transudate, Exudate, Empyema, Hemorrhagic pleural effusion or hemothorax and Chylous or chyliform effusion.

5
Causes of Pleural Effusion
Other causes of pleural effusion: nephrotic syndrome, TB, collagen vascular disease, urinothorax, SVC syndrome, Meigs syndrome, rheumatoid arthritis, pancreatitis, yellow-nail syndrome, drugs Light. NEJM 2002; 346:1971 Annual incidence in the US

6
Evaluation History: Physical: Dyspnea Pleuritic chest pain Cough Fever
Hemoptysis Wt. loss Trauma Hx. of cancer Cardiac surgery Physical: Dullness to percussion Decreased breath sounds Absent tactile fremitus Other findings: ascites, JVP, peripheral edema, friction rub, unilateral leg swelling

7
Chest X-Ray

8
Lateral Decubitus

9
CT Scan

10
Indications for Thoracocentesis

11
Indications for Thoracentesis
Likely indicated in most patients > 1 cm layering on lateral decubitus No need for thoracentesis for patient with obvious cause may not need further study (CHF with bilateral effusions. However: In heart failure: febrile/pleuritic pain, unilateral, no cardiomegaly, no response to diuresis

12
Pleural fluid analysis
Bloody: Hct <1% not significant 1-20%= CA, PE, Trauma >50% serum Hct = hemothorax Cloudy trig level >110mg/dl = chylothorax Putrid odor stain and culture = infection?

13
Light’s Criteria Pleural fluid is exudate if one or more:
Pleural LDH/Serum LDH > 0.6* -OR- Pleural protein/Serum protein > OR- Pleural LDH > 2/3 upper limit of normal (serum) Usually > 200 IU Absence of ALL: transudate Sensitivity 99%, Specificity 98%
 Usually > 200 IU. Absence of ALL: transudate. Sensitivity 99%, Specificity 98%")
14
Pleural Fluid Tests PORCEL et al. AFP 2006; 73: 1212

15
Pleural Fluid Tests PORCEL et al. AFP 2006; 73: 1212

16
Pleural Fluid Tests PORCEL et al. AFP 2006; 73: 1212

17
Pleural Fluid Tests PORCEL et al. AFP 2006; 73: 1212

18
Exudate Pneumonia Malignancy Pulmonary Embolism Transudate CHF Cirrhosis Nephrotic syndrome

19
Exudative Effusion Cell count - Neutrophil predom acute pleural process (pneumonia, PE) - Lyphocytic predom chronic process (Cancer, TB, CABG) Culture/stain- infected fluid Glucose- low level (<60mg/dl)(pneumonia, CA) Cytology- malignancy (non-dx- thoracoscopy) pH- parapneumonic <7.2 -must drain fluid malignant < 7.2 –poor prognosis
 Culture/stain- infected fluid. Glucose- low level (<60mg/dl)(pneumonia, CA) Cytology- malignancy (non-dx- thoracoscopy) pH- parapneumonic <7.2 -must drain fluid. malignant < 7.2 –poor prognosis.")
20
Malignant Effusions Clinical features suggestive of malignacy:
Symptoms> 1mo, absence of fever, blood-tinged fluid, chest CT suggesting malignancy Lung >breast > lymphoma/leukemia metastatic adenocarcinoma positive cytology 70% Lymphoma 25-50% Mesothelioma 10% Squamous Cell Carcinoma 20% Sarcoma within pleura 25% Pleural fluid: bloody, lymphocytic, decreased or normal glucose and pH, cytology

21
EXUDATIVE EFFUSIONS Lymphocytic (> 50%) Eosinophilic (> 10%)
CA (30-35%) TB (15-20%) Sarcoidosis PMNs Empyema Parapneumonic Rheumatoid Pulmonary infarction PMN or Lymphocytic PE Conn tissue disease Post-cardiac injury Eosinophilic (> 10%) Trauma PTX CA Asbestos, parasites Pneumonia RBC > 100,000/mm Pulmonary infarction
 TB (15-20%) Sarcoidosis. PMNs. Empyema. Parapneumonic. Rheumatoid. Pulmonary infarction. PMN or Lymphocytic. PE. Conn tissue disease. Post-cardiac injury. Eosinophilic (> 10%) Trauma. PTX. CA. Asbestos, parasites. Pneumonia. RBC > 100,000/mm. Pulmonary infarction.")
22
EXUDATIVE EFFUSIONS Other Tests
Suspected TB Adenosine deaminase (> 50 IU/L) B2 - microglobulin Lysozyme III (> 20mcg/mL) PCR (Sens 100%, Spec 95%) AFB (smear 10-20%; cx 25-50%) PPD Suspected Rheumatoid Pleural RF Low glucose Suspected SLE Serum Complement Pleural ANA LE cells prep? Suspected Pneumonia pH Suspected Pancreatitis Pleural Amylase
 B2 - microglobulin. Lysozyme III (> 20mcg/mL) PCR (Sens 100%, Spec 95%) AFB (smear 10-20%; cx 25-50%) PPD. Suspected Rheumatoid. Pleural RF. Low glucose. Suspected SLE. Serum Complement. Pleural ANA. LE cells prep Suspected Pneumonia. pH. Suspected Pancreatitis. Pleural Amylase.")
23
UNDIAGNOSED PLEURAL EFFUSIONS
15-20% of effusions Careful review of history, PE, meds, risk factors Consider occult abdominal process Consider PE

24
UNDIAGNOSED PLEURAL EFFUSIONS Cont’d
Risk factors for TB or malignant effusion Weight loss > 4.5 kg (10 pounds) Fever > 38 C Positive PPD Large effusion (> 1/2 hemithorax) < 95% lymphs in pleural fluid If ANY factor present, evaluate for TB, CA
 Fever > 38 C. Positive PPD. Large effusion (> 1/2 hemithorax) < 95% lymphs in pleural fluid. If ANY factor present, evaluate for TB, CA.")
25
UNDIAGNOSED PLEURAL EFFUSIONS Cont’d
PPD If (+) and lymphocytic effusion, initiate TB treatment If (-), repeat in 6-8 wks However, if effusion < 5% mesothelial cells, consider TB treatment If (-), not anergic, > 5% mesothelial cells, wait for repeat PPD in 6-8 wks If repeat PPD (-), not anergic and cultures negative, observe
 and lymphocytic effusion, initiate TB treatment. If (-), repeat in 6-8 wks. However, if effusion < 5% mesothelial cells, consider TB treatment. If (-), not anergic, > 5% mesothelial cells, wait for repeat PPD in 6-8 wks. If repeat PPD (-), not anergic and cultures negative, observe.")
27
BEYOND THORACENTESIS Pleural Biopsy Thoracoscopy
Most helpful in evaluating for TB Limited utility for CA (40-50% positive) Repeat cytology x 3 Sarcoid, fungal: might be helpful Thoracoscopy Most helpful in evaluating for malignancy
 Repeat cytology x 3. Sarcoid, fungal: might be helpful. Thoracoscopy. Most helpful in evaluating for malignancy.")
28
Approach to Pleural Effusion
PORCEL et al. AFP 2006; 73: 1212

29
Approach to Pleural Effusion
PORCEL et al. AFP 2006; 73: 1212

30
Approach to Pleural Effusion
PORCEL et al. AFP 2006; 73: 1212

31
Treatment Thoracentesis – then treat underlying disease
Uncomplicated pneumonia – antibiotics Hemithorax involved/empyema – tube thoracostomy +/- VATS Malignant effusion- chest tube +/- pleurodesis (sclerosants) VATS
 VATS.")
32
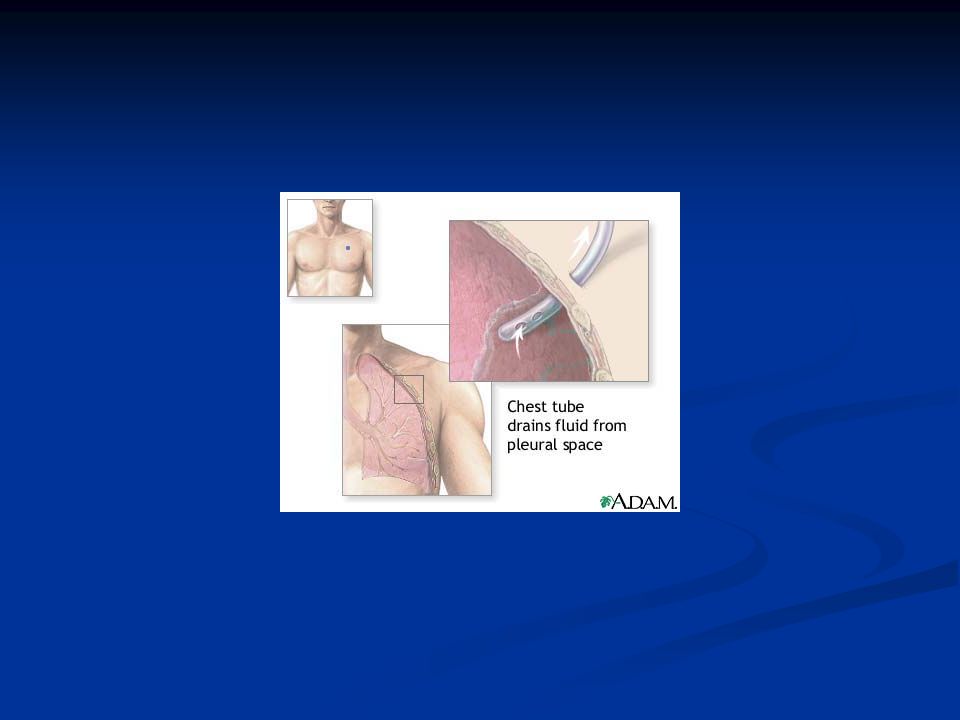
Indications for Chest Tube
Empyema Complicated parapneumonic effusion Hemothorax Malignant effusion- chest tube +/- pleurodesis (sclerosants)
")
44
Pleural Biopsy Most helpful in evaluating for TB
Limited utility for CA (40-50% positive) Repeat cytology x 3 Sarcoid, fungal: might be helpful
 Repeat cytology x 3. Sarcoid, fungal: might be helpful.")
45
Thoracoscopy

46
You may find this lecture and notes at this site:
faculty.ksu.edu.sa/ahmedbahammam

Similar presentations


















. -Cytological tests (>")


 The fluid is a plasma filtrate.>")








