Download presentation
Presentation is loading. Please wait.

1
Ron Hoffman, MD Thrombosis & Hemostasis Unit Rambam Medical Center
Bleeding Tendency Ron Hoffman, MD Thrombosis & Hemostasis Unit Rambam Medical Center 2

2
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

4
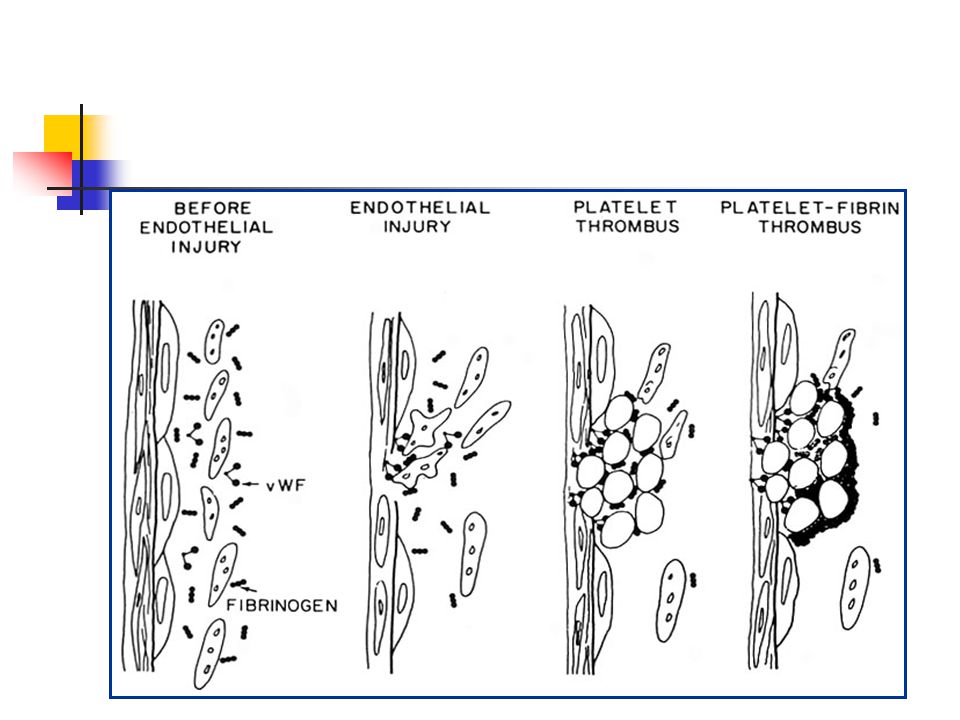
Primary Hemostasis

5
Coagulation cascade Intrinsic system (surface contact)
Extrinsic system (tissue damage) XII XIIa Tissue factor XI XIa IX IXa VIIa VII VIII VIIIa KEY POINT: The efficacy/safety ratio for currently available therapies is less than satisfactory due to their ill-defined, multitargeted activity. New antithrombotic strategies are needed that offer an improved efficacy/safety profile compared with existing antithrombotic agents.1,2 Currently available antithrombotic agents include the heparins (UFH and Enoxaparin), vitamin K antagonists (warfarin), and direct thrombin inhibitors (hirudins).3–6 The most widely used agents, heparins and vitamin K antagonists, have a range of actions on various components of the coagulation cascade. This contributes to the unpredictable clinical responses associated with these agents.3–5 Other limitations of currently available antithrombotics include3–7 High incidence of serious adverse effects, particularly bleeding complications Routine monitoring of coagulation markers may be needed and represents a substantial burden in terms of time and costs Narrow therapeutic margin Limited effectiveness in preventing VTE Factor Xa inhibitors are a novel class of antithrombotic agents designed to selectively target only 1 core step in the coagulation cascade, leading to potent and targeted effectiveness.8 Vitamin K dependant factors X Xa V Va II IIa IIa (Thrombin) Fibrinogen Fibrin For training purposes only—Not for distribution
 XII. XIIa. Tissue factor. XI. XIa. IX. IXa. VIIa. VII. VIII. VIIIa. KEY POINT: The efficacy/safety ratio for currently available therapies is less than satisfactory due to their ill-defined, multitargeted activity. New antithrombotic strategies are needed that offer an improved efficacy/safety profile compared with existing antithrombotic agents.1,2. Currently available antithrombotic agents include the heparins (UFH and Enoxaparin), vitamin K antagonists (warfarin), and direct thrombin inhibitors (hirudins).3–6. The most widely used agents, heparins and vitamin K antagonists, have a range of actions on various components of the coagulation cascade. This contributes to the unpredictable clinical responses associated with these agents.3–5. Other limitations of currently available antithrombotics include3–7. High incidence of serious adverse effects, particularly bleeding complications. Routine monitoring of coagulation markers may be needed and represents a substantial. burden in terms of time and costs. Narrow therapeutic margin. Limited effectiveness in preventing VTE. Factor Xa inhibitors are a novel class of antithrombotic agents designed to selectively target only 1 core step in the coagulation cascade, leading to potent and targeted effectiveness.8. Vitamin K dependant factors. X. Xa. V. Va. II. IIa. IIa. (Thrombin) Fibrinogen. Fibrin. For training purposes only—Not for distribution.")
6
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

7
Clinical Features of Bleeding Disorders
Platelet Coagulation disorders factor disorders Site of bleeding Skin Deep in soft tissues Mucous membranes (joints, muscles) (epistaxis, gum, vaginal, GI tract) Petechiae Yes No Ecchymoses (“bruises”) Small, superficial Large, deep Hemarthrosis / muscle bleeding Extremely rare Common Bleeding after cuts & scratches Yes No Bleeding after surgery or trauma Immediate, Delayed (1-2 days), usually mild often severe
 (epistaxis, gum, vaginal, GI tract) Petechiae Yes No. Ecchymoses ( bruises ) Small, superficial Large, deep. Hemarthrosis / muscle bleeding Extremely rare Common. Bleeding after cuts & scratches Yes No. Bleeding after surgery or trauma Immediate, Delayed (1-2 days), usually mild often severe.")
8
(typical of platelet disorders)
Petechiae (typical of platelet disorders) Do not blanch with pressure (cf. angiomas) Not palpable (cf. vasculitis)
 Do not blanch with pressure (cf. angiomas) Not palpable (cf. vasculitis)")
9
(typical of coagulation factor disorders)
Ecchymoses (typical of coagulation factor disorders)
")
10
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

11
Systemic screening Epistaxis – age, frequency, spontaneous, how long, way of bleeding arrest, blood products. Oral cavity : tooth, gums, tonsils + adenoids . Skin Trauma: minor , major GI & urinary tract. Brain Gynecological: menses, pregnancy and deliveries abortions. Hemarthroses, muscular. Circumcision , umbilical

12
Important aspects Differentiation between hemostatic bleeding and surgical. Immediate vs. late bleeding (primary vs secondary hemostatic problem). Abnormal blood vessel Normal coagulation factors may be present in pregnancy!

13
Medications – most common
COX & ADP inhibitors : Aspirin, Clopidogrel, NSAID Background disease Acute leukemia (APL) MPD Uremia Cirrhosis
 MPD. Uremia. Cirrhosis.")
14
Family history prolonged PT and/or PTT Sex-linked recessive
Factors VIII and IX deficiencies cause bleeding Prolonged PTT; PT normal Autosomal recessive (rare) Factors II, V, VII, X, XI, fibrinogen deficiencies cause bleeding - prolonged PT and/or PTT Factor XIII deficiency is associated with bleeding and impaired wound healing PT/ PTT normal; clot solubility abnormal Factor XII, prekallikrein, HMWK deficiencies do not cause bleeding
 Factors II, V, VII, X, XI, fibrinogen deficiencies cause bleeding - prolonged PT and/or PTT. Factor XIII deficiency is associated with bleeding and. impaired wound healing. PT/ PTT normal; clot solubility abnormal. Factor XII, prekallikrein, HMWK deficiencies. do not cause bleeding.")
15
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

16
Clinical bleeding Senile purpura, purpura simplex
Signs of systemic disease : ED, Cushing, Amyloidosis, Cirrhosis, MPD

17
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

18
CBC and blood smear (thrombocytopenia, thrombocytopathia).
Basic coagulation tests: PT, aPTT, Fibrinogen. Advanced coagulation tests: TT, Mixing assays, Factor levels , PFA, Fibrinolysis assays.

19
Laboratory Evaluation of the Coagulation Pathways
Partial thromboplastin time (PTT) Prothrombin time (PT) Surface activating agent (Ellagic acid, kaolin) Phospholipid Calcium Thromboplastin Tissue factor Phospholipid Calcium Intrinsic pathway Extrinsic pathway Thrombin time Common pathway Thrombin Fibrin clot
 Prothrombin time. (PT) Surface activating agent. (Ellagic acid, kaolin) Phospholipid. Calcium. Thromboplastin. Tissue factor. Phospholipid. Calcium. Intrinsic pathway. Extrinsic pathway. Thrombin time. Common pathway. Thrombin. Fibrin clot.")
20
Pre-analytic errors Biological effects Problems with blue-top tube
Hct ≥55 or ≤15 Lipemia, hyperbilirubinemia, hemolysis Laboratory errors Delay in testing Prolonged incubation at 37°C Freeze/thaw deterioration Problems with blue-top tube Partial fill tubes Vacuum leak and citrate evaporation Problems with phlebotomy Heparin contamination Wrong label Slow fill Underfill Vigorous shaking

21
Initial Evaluation of a Bleeding Patient - 1
Normal PT Normal PTT Abnormal Urea solubility Factor XIII deficiency Normal Consider evaluating for: Mild factor deficiency Monoclonal gammopathy Abnormal fibrinolysis Platelet disorder (a2 anti-plasmin def) Vascular disorder Elevated FDPs
 Vascular disorder. Elevated FDPs.")
22
Initial Evaluation of a Bleeding Patient - 2
Normal PT Abnormal PTT 50:50 mix is abnormal Repeat with 50:50 mix Test for inhibitor activity: Specific factors: VIII,IX, XI Non-specific (anti-phospholipid Ab) 50:50 mix is normal Test for factor deficiency: Isolated deficiency in intrinsic pathway (factors VIII, IX, XI) Multiple factor deficiencies (rare)
 50:50 mix is normal. Test for factor deficiency: Isolated deficiency in intrinsic pathway (factors VIII, IX, XI) Multiple factor deficiencies (rare)")
23
Initial Evaluation of a Bleeding Patient - 3
Abnormal PT Normal PTT 50:50 mix is abnormal Repeat with 50:50 mix Test for inhibitor activity: Specific: Factor VII (rare) Non-specific: Anti-phospholipid (rare) 50:50 mix is normal Test for factor deficiency: Isolated deficiency of factor VII (rare) Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)
 Non-specific: Anti-phospholipid (rare) 50:50 mix is normal. Test for factor deficiency: Isolated deficiency of factor VII (rare) Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)")
24
Initial Evaluation of a Bleeding Patient - 4
Abnormal PT Abnormal PTT 50:50 mix is abnormal Repeat with 50:50 mix Test for inhibitor activity: Specific : Factors V, X, Prothrombin, Fibrinogen (rare) Non-specific: anti-phospholipid (common) 50:50 mix is normal Test for factor deficiency: Isolated deficiency in common pathway: Factors V, X, Prothrombin, Fibrinogen Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)
 Non-specific: anti-phospholipid (common) 50:50 mix is normal. Test for factor deficiency: Isolated deficiency in common pathway: Factors V, X, Prothrombin, Fibrinogen. Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)")
25
Thrombin Time Bypasses factors II-XII
Measures rate of fibrinogen conversion to fibrin Procedure: Add thrombin with patient plasma Measure time to clot Variables: Source and quantity of thrombin

26
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

27
Thrombocytpenia and thrombocytopathia,
Hemophilia A,B, Acquired VWD Acquired coagulations factors deficiency: Cirrosis

28
Classification of platelet disorders
Quantitative disorders Abnormal distribution Dilution effect Decreased production Increased destruction Qualitative disorders Inherited disorders (rare) Acquired disorders Medications Chronic renal failure Cardiopulmonary bypass MPD
 Acquired disorders. Medications. Chronic renal failure. Cardiopulmonary bypass. MPD.")
29
Inherited platelet disorders

30
Thrombocytopenia Immune-mediated Idioapthic (ITP) Drug-induced
Collagen vascular disease Lymphoproliferative disease Viral (HIV) Non-immune mediated DIC Microangiopathic hemolytic anemia Drugs
 Non-immune mediated. DIC. Microangiopathic hemolytic anemia. Drugs.")
31
Features of Acute and Chronic ITP
Features Acute ITP Chronic ITP Peak age Children (2-6 yrs) Adults (20-40 yrs) Female:male 1:1 3:1 Antecedent infection Common Rare Onset of symptoms Abrupt Abrupt-indolent Platelet count at presentation <20,000 <50,000 Duration weeks Long-term Spontaneous remission Common Uncommon
 Adults (20-40 yrs) Female:male 1:1 3:1. Antecedent infection Common Rare. Onset of symptoms Abrupt Abrupt-indolent. Platelet count at presentation <20,000 <50,000. Duration 2-6 weeks Long-term. Spontaneous remission Common Uncommon.")
32
Initial treatment of ITP
Platelet count Symptoms Treatment (per µl) >50,000 None 20-50,000 Not bleeding None Bleeding Glucocorticoids IVIG <20,000 Not bleeding Glucocorticoids
 >50,000 None ,000 Not bleeding None. Bleeding Glucocorticoids. IVIG. <20,000 Not bleeding Glucocorticoids.")
33
Coagulation factor disorders
Inherited bleeding disorders Hemophilia A and B vonWillebrands disease Other factor deficiencies Acquired bleeding Disorders Liver disease Vitamin K deficiency/warfarin overdose DIC

34
Hemophilia A and B Hemophilia A Hemophilia B
Coagulation factor deficiency Factor VIII Factor IX Inheritance X-linked X-linked recessive recessive Incidence 1/10,000 males 1/50,000 males Severity Related to factor level <1% - Severe - spontaneous bleeding 1-5% - Moderate - bleeding with mild injury 5-25% - Mild - bleeding with surgery or trauma Complications Soft tissue bleeding

35
Hemarthrosis (acute)
")
36
Treatment of Hemophilia A
Intermediate purity plasma products Virucidally treated May contain von Willebrand factor High purity (monoclonal) plasma products No functional von Willebrand factor Recombinant factor VIII Virus free/No apparent risk
 plasma products. No functional von Willebrand factor. Recombinant factor VIII. Virus free/No apparent risk.")
37
Acquired hemophilia Associated with: auto immunity, post partum, cancer and drugs Bleeding manifestations : muscular, internal, usually not hemarthroses Diagnosis : prolonged aPTT, mixing FVIII levels, r/o LAC Responding to immuno suppressive (IVIG) Control of bleeding by: high dose FVIII, Porcine FVIII, APCC, rFVIIa
 Control of bleeding by: high dose FVIII, Porcine FVIII, APCC, rFVIIa.")
38
Congenital Coagulopathies
FXII deficiency FXI deficiency Hemophilia A + B Afibrinogenemia FV + FVIII deficiency FVII deficiency FXIII deficiency Type 3 VWD

39
VWD Clinical Features von Willebrand factor
Synthesis in endothelium and megakaryocytes Forms large multimer Carrier of factor VIII Anchors platelets to subendothelium Bridge between platelets Inheritance - autosomal dominant Incidence - 1/10,000 Clinical features - mucocutaneous bleeding

40
Laboratory evaluation of VWD
Classification Type 1 Most common Partial quantitative deficiency Type 2 Qualitative deficiency Type 3 Total quantitative deficiency Diagnostic tests: Assay VWD type vWF antigen low normal very low vWF activity low low very low FVIII low normal absent Multimer analysis normal abnormal normal

41
Treatment of VWD Cryoprecipitate
Source of fibrinogen, factor VIII and VWF Only plasma fraction that consistently contains VWF multimers DDAVP (deamino-8-arginine vasopressin) plasma VWF levels by stimulating secretion from endothelium Duration of response is variable Not generally used in type 2 disease Dosage 0.3 µg/kg q 12 hr IV Factor VIII concentrate (Intermediate purity) Virally inactivated product
 plasma VWF levels by stimulating secretion from endothelium. Duration of response is variable. Not generally used in type 2 disease. Dosage 0.3 µg/kg q 12 hr IV. Factor VIII concentrate (Intermediate purity) Virally inactivated product.")
42
Vitamin K deficiency Source of vitamin K Green vegetables Synthesized by intestinal flora Required for synthesis Factors II, VII, IX ,X Protein C and S Causes of deficiency Malnutrition Biliary obstruction Malabsorption Antibiotic therapy (coumadin) Treatment Vitamin K Fresh frozen plasma
 Treatment Vitamin K Fresh frozen plasma.")
43
Liver Disease and Hemostasis
Decreased synthesis of II, VII, IX, X, XI, and fibrinogen Dietary Vitamin K deficiency (Inadequate intake or malabsortion) Dysfibrinogenemia Enhanced fibrinolysis (Decreased alpha-2-antiplasmin) DIC Thrombocytoepnia due to hypersplenism
 Dysfibrinogenemia. Enhanced fibrinolysis (Decreased alpha-2-antiplasmin) DIC. Thrombocytoepnia due to hypersplenism.")
44
Objectives Clinical aspects of bleeding Medical history Personal
Family Physical exam Approach to laboratory abnormalities Bleeding disorders Therapy 2

45
Treatment Approaches to the Bleeding Patient
Red blood cells Platelet transfusions Fresh frozen plasma Cryoprecipitate Amicar DDAVP Recombinant Human factor VIIa

46
Approach to bleeding disorders
Medical history – the most important diagnostic “test” Identify and correct any specific defect of hemostasis Laboratory testing is almost always needed to establish the cause of bleeding Screening tests (PT,PTT, platelet count) will often allow placement into one of the broad categories Specialized testing is usually necessary to establish a specific diagnosis.
 will often allow placement into one of the broad categories. Specialized testing is usually necessary to establish a specific diagnosis.")
Similar presentations