Download presentation
Presentation is loading. Please wait.

1
Comparative Pathology of TRUS Biopsy, Mapping Biopsy and Prostatectomy Specimens Francisco G. La Rosa, MD Francisco.LaRosa@ucdenver.edu Associate Professor, Department of Pathology University of Colorado Denver, Aurora, Colorado Targeted Focal Therapy Workshop August 16 – 17, 2012

5
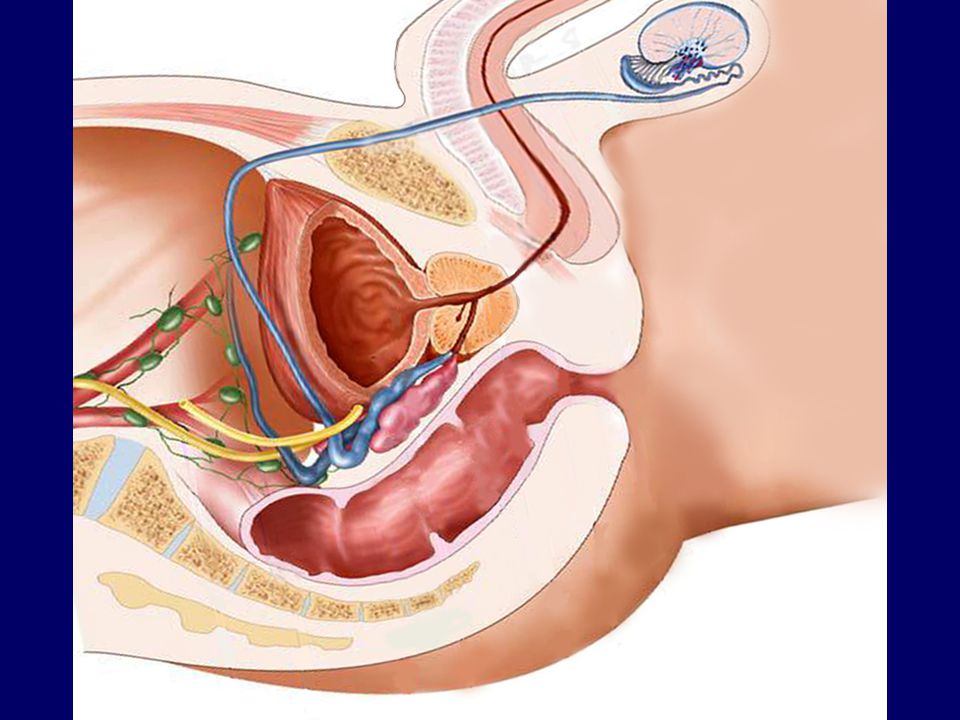
SAGITAL SECTION OF THE PROSTATE GLAND Seminal Vesicle Central Zone Bladder Peri-urethral zone Anterior Zone Fibro-muscular Peripheral Zone Transition Zone Urethra

6
CROSS SECTION OF THE PROSTATE FIBROMUSCULAR STROMA anterior PERI-URETHRAL STROMA EJACULATORY DUCTS

7
HISTORY OF PROSTATE BIOPSY - 1930, Ferguson: First described prostate biopsy. Obtained cancer cells by aspirating prostate tissue with an 18-gauge needle transperineally. - 1937, Astraldi: First transrectal biopsy - 1963, Takahashi & Ouchi: First TRUS biopsy - 1967, Watanabe: First clinical application of TRUS images - 1980’s Transperineal biopsies

8
The first sextant prostate needle biopsy scheme was developed by Hodge et al. in 1989 The sextant biopsy scheme consisted of biopsies of the prostate in the midline at the base, mid-gland, and apex. The midline sextant biopsies had a PCa detection rate of 20-30%. However, 25-50% of aggressive PCa remain undetected when using the midline sextant biopsies scheme. J Urol 1989; 142: 71-74 J Urol 2000; 163: 152-157 J Urol 2000; 163: 163-166 Urology 2003; 61: 1181-1186 J Urol 1998; 159: 1260-1264

9
Stamey et al. in 1995 evaluated radical prostatectomy specimens and found that PCa had a higher likelihood of being found in the anterior horns of the peripheral zone and suggested that laterally directed biopsies may provide better detection. Urology 1995; 45: 2-12

10
Multiple studies have found that directing prostate needle biopsies more laterally increases the PCa detection rates. J Urol 2000; 163: 152-157 J Urol 2000; 163: 163-166 Urology 2003; 61: 1181-1186

11
The current recommendation is an extended-biopsy scheme with at least 8-12 cores including lateral biopsies. Transition zone biopsies are not recommended on initial evaluation. Curr Opin Urol 2004; 14: 157-162

12
It is important to perform both the lateral modified fan- shaped biopsy and the midline sextant biopsies to improve overall PCa detections rates. Thus, we recommend performing midline sextant biopsies, modified fan-shaped biopsy, and transition zone biopsies based on prostate volume, as follows: - 8 biopsies for ≤15 cc - 14 for those >15 cc but ≤50 cc - 14-20 for those >50 cc 1.Werahera PN, Sullivan K, La Rosa FG, Kim FJ, Lucia MS, O’Donnell C, Sidhu RS, Sullivan HT, Schulte B, Crawford ED. Optimization of Prostate Cancer Diagnosis by Increasing the Number of Core Biopsies Based on Gland Volume.. Int J Clin Exp Pathol (in press)
.")
13
TRUS Biopsies

14
TRANS RECTAL ULTRASOUND (TRUS) GUIDED BIOPSY PROCEDURE
 GUIDED BIOPSY PROCEDURE")
16
Bad Histology

17
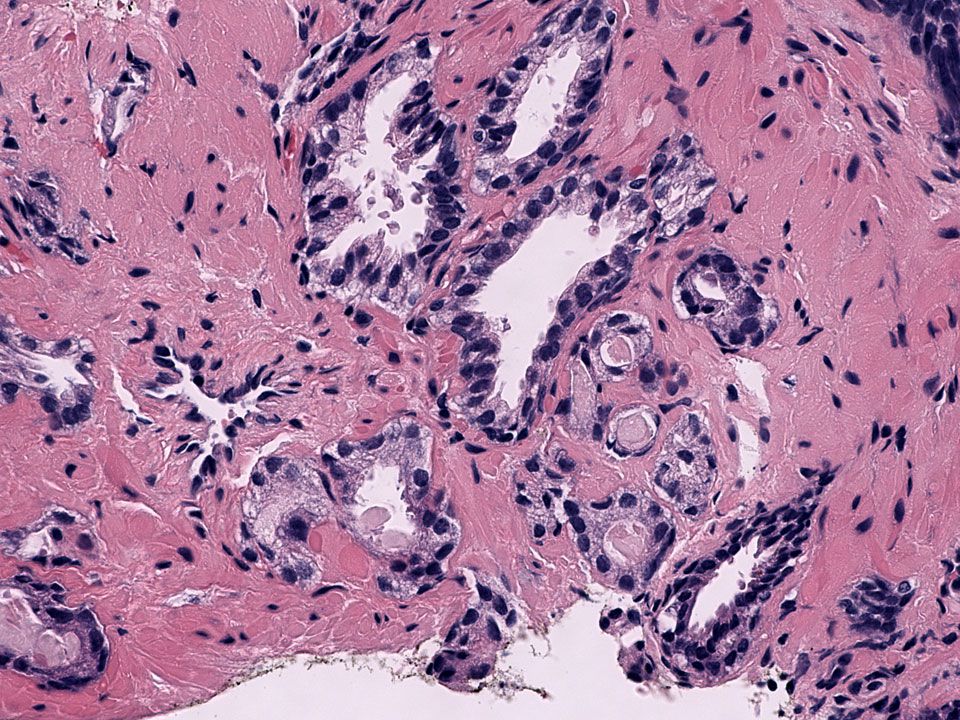
Good Histology

18
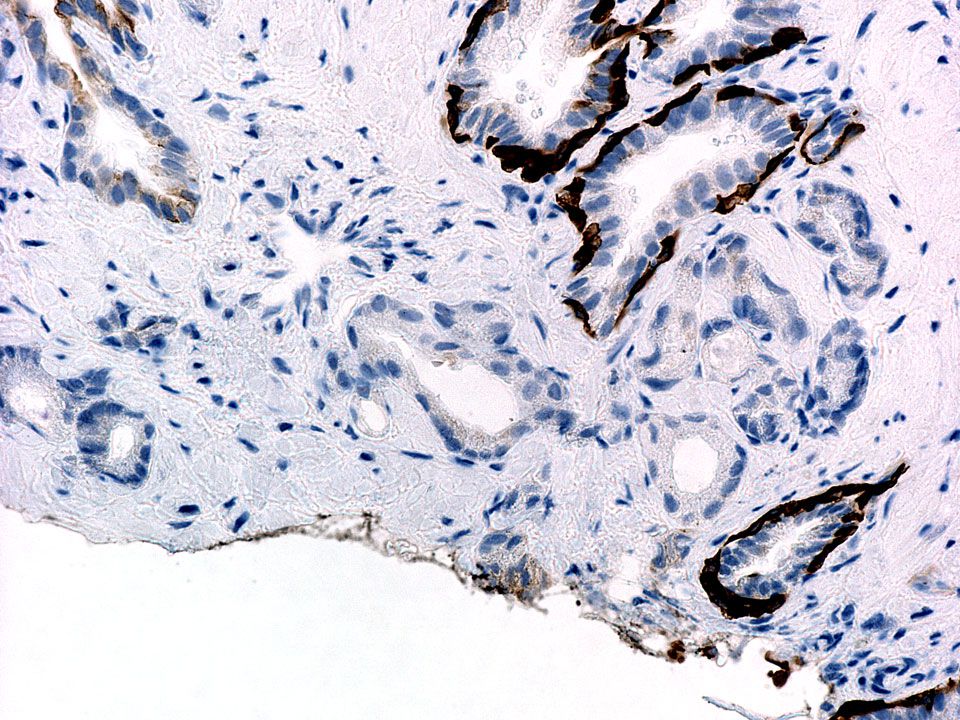
Peripheral Zone

19
Central Zone

21
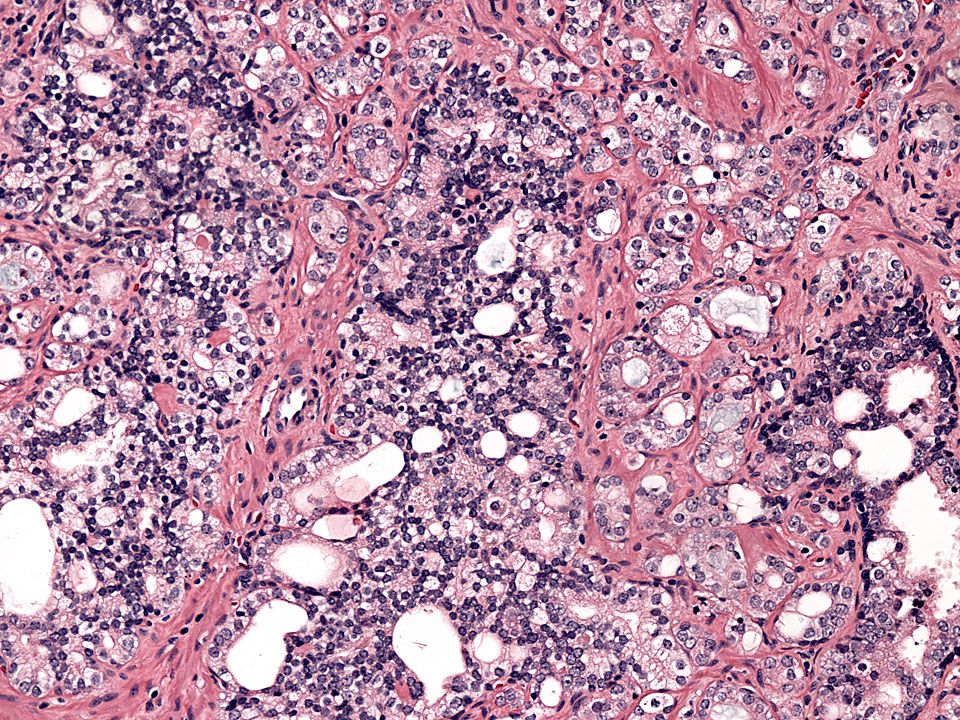
40X Seminal Vesicles

22
Mapping Biopsies

24
Mapping Grid and its relationship with the Prostate

27
Grid Alignment in perineal area and Rectal Location of Ultrasound Probe

28
Pathology Report of Mapping Biopsies

30
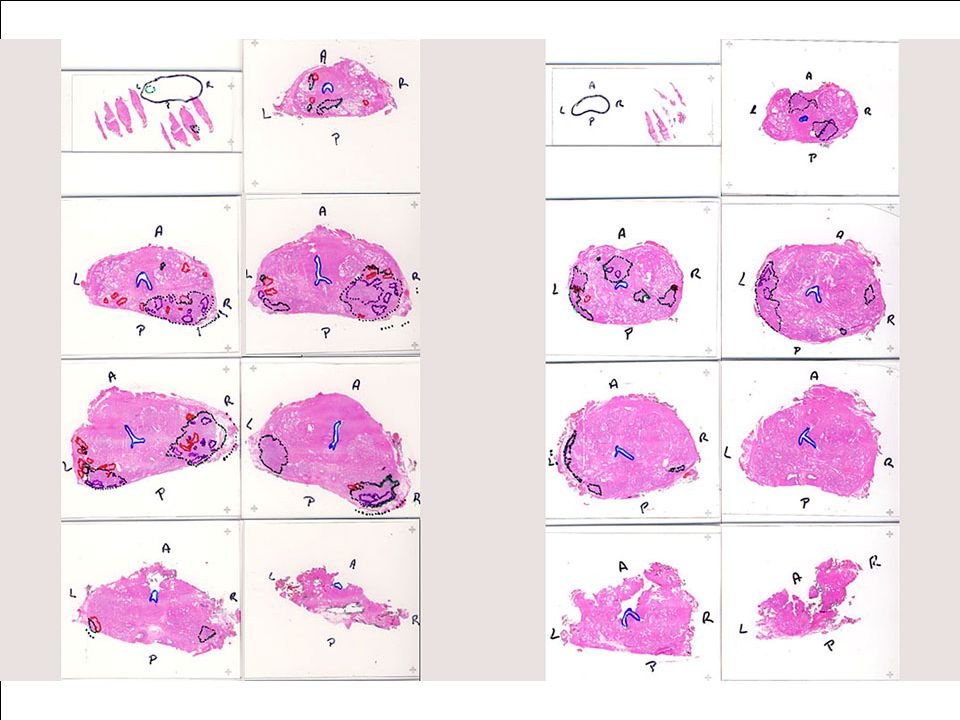
3D Reconstruction of Prostate With Location of Cancer Lesions

31
Watch Video “Mapping Biopsy procedure” http://3dprostate.com/videos/mapping-biopsy.html

32
Whole Mount Prostatectomy Specimens http://3dprostate.com/videos/gross-prostate.html http://3dprostate.com/videos/gross-prostate.html

33
Prostate Cancer: Gross

38
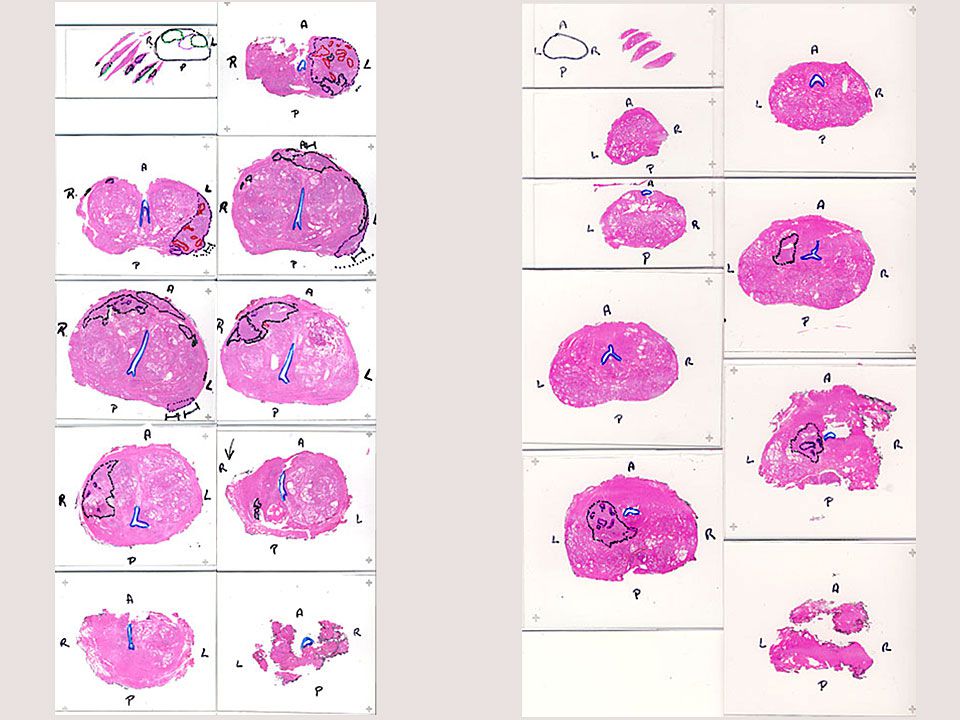
3-Dimensional Reconstruction of whole- mounted prostatectomy specimens

41
Venn-diagram representation of activity of patients between positive results from transperineal mapping biopsies (TPMB) and three-dimensional whole-mounted radical prostatectomies (3D-WMRP). (+) indicates presence of prostatic cancer (-) indicates no cancer
 indicates presence of prostatic cancer (-) indicates no cancer.")
42
- TPMB with a 5-mm grid is an important staging tool that more closely reflects true PCa disease state as found at RP as 10-12-core TRUSB and other more limited protocols. - TPMB can detect or rule out more aggressive disease, identifying with more accuracy the size and GS of PCa lesions, ensuring that patients are not mistakenly under-treated or unnecessarily over- treated, minimizing treatment-related morbidity.

43
Case 1 58-year-old man, PSA 4.2 ng/mL,

48
TRUS guided biopsies Prostate, right: - Prostatic adenocarcinoma, Gleason grade 3 + 3 (score = 6) involving <5% of 1 of 12 biopsy core fragments -No evidence of perineural or extra-capsular invasion Prostate, left, fine needle core biopsies (B): - Prostatic adenocarcinoma, Gleason grade 3 + 3 (score = 6) involving <5% of 2 of 10 biopsy core fragments - No evidence of perineural or extra-capsular invasion
 involving <5% of 1 of 12 biopsy core fragments -No evidence of perineural or extra-capsular invasion Prostate, left, fine needle core biopsies (B): - Prostatic adenocarcinoma, Gleason grade (score = 6) involving <5% of 2 of 10 biopsy core fragments - No evidence of perineural or extra-capsular invasion")
49
Radical prostatectomy (after fixation) Length (apex to base) : 3.8 cm Length (apex to base) : 3.8 cm Width (left to right) : 5.2 cm Width (left to right) : 5.2 cm Height (anterior to posterior) : 4.0 cm Height (anterior to posterior) : 4.0 cm Volume: 50.0 mL Volume: 50.0 mL Weight: 50.5 g Weight: 50.5 g Serial whole-mount sections from apex to base of entire prostate and seminal vesicles submitted in (A1-A9), seminal vesicle complex in A10, A11, right seminal vesicle in A12, A13, left seminal vesicle in A14, A15.
 Length (apex to base) : 3.8 cm Length (apex to base) : 3.8 cm Width (left to right) : 5.2 cm Width (left to right) : 5.2 cm Height (anterior to posterior) : 4.0 cm Height (anterior to posterior) : 4.0 cm Volume: 50.0 mL Volume: 50.0 mL Weight: 50.5 g Weight: 50.5 g Serial whole-mount sections from apex to base of entire prostate and seminal vesicles submitted in (A1-A9), seminal vesicle complex in A10, A11, right seminal vesicle in A12, A13, left seminal vesicle in A14, A15.")
52
Prostate and seminal vesicles, radical prostatectomy: - Prostatic adenocarcinoma, overall Gleason Grade 4 + 5 (score = 9) with secondary foci of Gleason grade 3 + 3 (score = 6), multifocal and bilateral, involving <5% of prostate (see comments) - Suspicious but not definitive for lymphovascular invasion - Perineural invasion, multifocal - No evidence of extracapsular extension - Seminal vesicles with no evidence of malignancy
 with secondary foci of Gleason grade (score = 6), multifocal and bilateral, involving <5% of prostate (see comments) - Suspicious but not definitive for lymphovascular invasion - Perineural invasion, multifocal - No evidence of extracapsular extension - Seminal vesicles with no evidence of malignancy")
54
Second Opinion Process Urology Clinic Patient (outside diagnostic material) Uropathology (2 nd opinion) Clinical Decision for Therapy Radiology (second opinion) UROLOGIC CANCER SECOND OPINION CONFERENCE Pathology slides returned
 Uropathology (2 nd opinion) Clinical Decision for Therapy Radiology (second opinion) UROLOGIC CANCER SECOND OPINION CONFERENCE Pathology slides returned")
55
UROLOGIC CANCER SECOND OPINION CONFERENCE

56
The Value of 2 nd Opinion Pathology Diagnosis of Prostate Biopsies Outside pathology report versus 2 nd Opinion in-house versus Whole-Mount Radical Prostatectomy

57
Second opinion of prostate biopsies Most critical histopathological features: - Gleason Score - Gleason Score (sum of primary plus secondary grades) - Extracapsular extension - Perineural invasion (multifocal) - Identification of HG PIN, ASAP, acute inflammation
 - Extracapsular extension - Perineural invasion (multifocal) - Identification of HG PIN, ASAP, acute inflammation")
63
# of CasesDiscrepancies 820156 (19 %) DIAGNOSIS DISCREPANCIES WITH OUTSIDE CASES 2008 – 2010 (Source: Quality Improvement database, Department of Pathology, UCD)
 DIAGNOSIS DISCREPANCIES WITH OUTSIDE CASES 2008 – 2010 (Source: Quality Improvement database, Department of Pathology, UCD)")
64
We found a significant disagreement between outside and in-house primary and secondary Gleason grades (McNemar statistic 6.250, p=0.012) Barqawi AB, Turcanu R, Gamito EJ, Lucia SM, O'Donnell CI, Crawford ED, La Rosa DD, La Rosa FG. The value of second-opinion pathology diagnoses on prostate biopsies from patients referred for management of prostate cancer. Int J Clin Exp Pathol. 2011 Jun 20;4(5):468-75.
:")
65
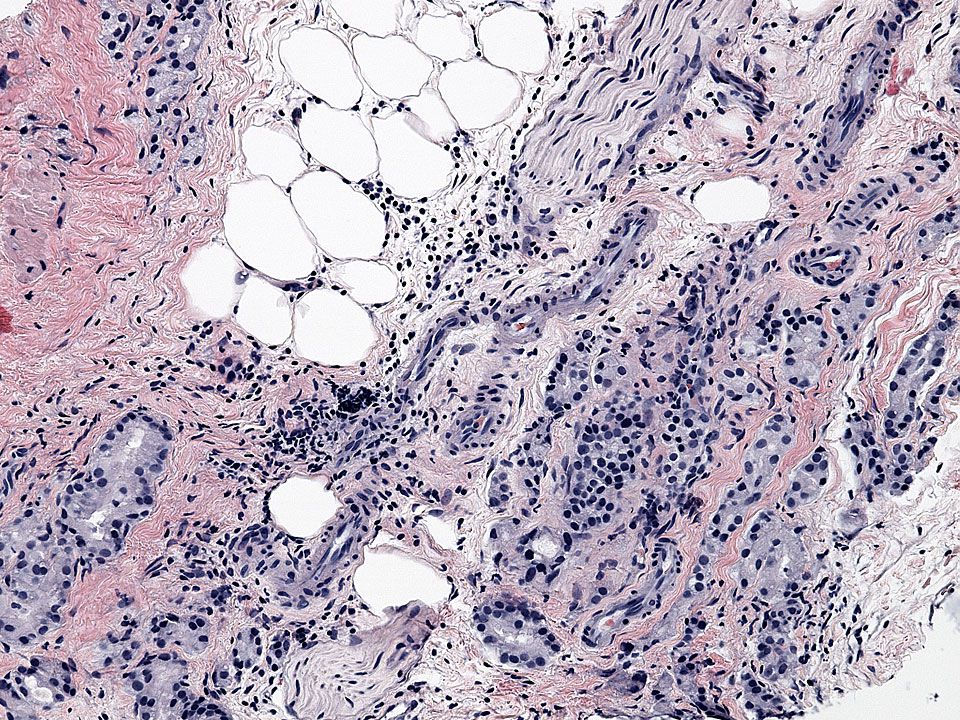
In-house pathologists detected significant features not reported by outside pathologists: i.e. the presence of adipose tissue invasion which is highly suspicious for extraprostatic extension by tumor Barqawi AB, Turcanu R, Gamito EJ, Lucia SM, O'Donnell CI, Crawford ED, La Rosa DD, La Rosa FG. The value of second-opinion pathology diagnoses on prostate biopsies from patients referred for management of prostate cancer. Int J Clin Exp Pathol. 2011 Jun 20;4(5):468-75.
:")
66
REPORTING ACUTE INFLAMMATION and BPH RELEVANCE: - Explains increased PSA values in patients negative for PCa - It can help in determining the need for quick repeat biopsies Schatteman PHF, Hoekx L, Wyndaele JJ, Jeuris W, van Marck E. Inflammation in Prostate Biopsies of Men without Prostatic Malignancy or Clinical Prostatitis. Eur Urol 2000;37:404-412

69
We strongly recommend that a re-evaluation by in-house urologic pathologists should be performed on all outside specimens before patients are admitted for treatment in any institution. Barqawi AB, Turcanu R, Gamito EJ, Lucia SM, O'Donnell CI, Crawford ED, La Rosa DD, La Rosa FG. The value of second-opinion pathology diagnoses on prostate biopsies from patients referred for management of prostate cancer. Int J Clin Exp Pathol. 2011 Jun 20;4(5):468-75.
:")
70
Paul Arangua Al Barqawi, MD E. David Crawford, MD Thomas Flaig, MD Eduard Gamito (+) Mark Gallen Michael Glode Kenneth Iczkowski, MD Clifford Jones, DD Francisco G. La Rosa, MD M. Scott Lucia, MD Colin I. O’Donnell Nayana Patel,, MD Susan Sullivan Kathleen Torkko Ruslan Turcanu, MD Departments of Pathology, Surgery, Radiology & Division of Medical Oncology University of Colorado Denver Anschutz Medical Campus School of Medicine Aurora, CO 80045 Urology Team
 Mark Gallen Michael Glode Kenneth Iczkowski, MD Clifford Jones, DD Francisco G. La Rosa, MD M. Scott Lucia, MD Colin I. O’Donnell Nayana Patel,, MD Susan Sullivan Kathleen Torkko Ruslan Turcanu, MD Departments of Pathology, Surgery, Radiology & Division of Medical Oncology University of Colorado Denver Anschutz Medical Campus School of Medicine Aurora, CO Urology Team.")
Similar presentations




























 never assigned Grade 2 rarely assigned on TURP and RP (exceptionally rare on biopsy)>")












