Download presentation
Presentation is loading. Please wait.

1
Western LDC 26 March 2013 Donncha O’Carolan Chief Dental Officer

2
Overview Presentation Background to DHSSPS local decontamination guidance & recent changes GDS budget – structure, allocation & trend Need for efficiencies &GDS savings proposals New Contract Q&A

3
Local Decontamination Guidance

4
A Protocol for the Local Decontamination of Surgical Instruments Issued July 2001, Health Estates DHSSPS Key areas All local decontamination outside of clinical setting where possible Recommends automated washing Downward displacement autoclaves- not suitable for processing wrapped instruments or hollow instruments Do not re-use single use instruments Described as short term strategy

5
BDA A12 Issued February 2003 Key points Where possible instruments to be decontaminated in a separate room Recommends washer disinfector over manual cleaning Wrapped instruments must be sterilised in a vacuum autoclave Single use instruments used wherever possible & discarded after use

6
Hine Review of Decontamination of Endoscopes May 2004 problem identified with decontamination of endoscopes/ risk of cross infection with blood bore viruses Review of effectiveness of arrangements for decontamination of endoscopes & lessons learnt Service wide review of decontamination of all re-usable medical devices

7
Audit of Dental Practices Letter from CDO issued all GDPs December 2004 Review current policies & procedures Complete audit Conform with recommendations in A12 Overall compliance 53% amber 47% green Priority areas: amalgam separators; chart recorders autoclaves; independent water supplies; LDU; WDs; disposable instruments

8
Audit of Dental Practices – follow up 2005/07 Series of training workshops across NI (Dr Wil Coulter & Dr Caroline Pankhurst) Cross Infection Control Manual /CD-ROM Action plan developed 2006/07 (published annual report 2007/08 ) Input DHSSPS, HSSB Dental Directors, Dr Wil Coulter, DPAs, ICNs, LDCs, RoI
 Cross Infection Control Manual /CD-ROM Action plan developed 2006/07 (published annual report 2007/08 ) Input DHSSPS, HSSB Dental Directors, Dr Wil Coulter, DPAs, ICNs, LDCs, RoI")
9
Policy Position Nov 2007 QIS letter; listed priority areas, priority funding, 3-5yr lead in time, advice & support HTM 01-05 (web) issued DH mid 2009 PEL(09) 02 issued18 June 2009 HTM 01-05 & audit tool (hard copy) issued DH Nov 2009 PEL(10)04 issued 19 Feb 2010
 issued DH mid 2009 PEL(09) 02 issued18 June 2009 HTM & audit tool (hard copy) issued DH Nov 2009 PEL(10)04 issued 19 Feb 2010")
10
Evidence Base Advisors HTM01-05; BDA, MHRA, HPA, Infection Protection Society, Healthcare Commission, Decontamination experts, GDPs, microbiologists, engineers Evidence base published: Acts & Regulations; Codes of Practice; British, European & International Stds, research papers, Official Publications

11
Funding QIS money 2005 - 2010 key priority decontamination (approx £1million recurrent) Addition QIS money 2007/2008 £3 million Practice allowance Additional £4million (↑ from 5% to 11%) September 2007. Currently £8.6million –‘increasing practice requirements in relation to the provision of high quality premises, health & safety, staffing support & information collection & provision

12
PEL(10)04 – Northern Ireland Amendments [Feb 2010] IssueHTM 01-05 (DH Position)DHSSPS position N. Ireland Time scales Working at or above Essential requirements 1 yr from November 2009; Detailed plan to move to best practice QIS letter 13 November 2007 set the timescale for ‘Best Practice’ 3 years to start working towards. 5 years to achieve. Manual cleaning Every practice meeting essential requirements ‘validated decontamination cycle’ Best practice- Washer disinfector Manual cleaning is not a validated process Practices to use Washer-Disinfectors by November 2012. Packaging processed instruments Permits drying and packing of instruments processed in a type N steriliser (Non-vacuum) and storage for 21 days This is not a validated process No evidence base to support this Instruments processed in a type N steriliser should be stored in covered trays and used in same working day Room layout 3 exemplar room layouts are illustrated Figure 1 layout is not accepted as a washer- disinfector is absent
![PEL(10)04 – Northern Ireland Amendments [Feb 2010] IssueHTM (DH Position)DHSSPS position N.](http://images.slideplayer.com/13/3902552/slides/slide_12.jpg "Ireland Time scales Working at or above Essential requirements 1 yr from November 2009; Detailed plan to move to best practice QIS letter 13 November 2007 set the timescale for ‘Best Practice’ 3 years to start working towards. 5 years to achieve. Manual cleaning Every practice meeting essential requirements ‘validated decontamination cycle’ Best practice- Washer disinfector Manual cleaning is not a validated process Practices to use Washer-Disinfectors by November Packaging processed instruments Permits drying and packing of instruments processed in a type N steriliser (Non-vacuum) and storage for 21 days This is not a validated process No evidence base to support this Instruments processed in a type N steriliser should be stored in covered trays and used in same working day Room layout 3 exemplar room layouts are illustrated Figure 1 layout is not accepted as a washer- disinfector is absent.")
13
Review of PEL(10) 04 DHSSPS reviewed in summer 2011 –Meetings HSCB, RQIA & NIMDTA DHSSPS further reviewed in summer/autumn 2012 –Meetings BDA, HSCB, RQIA & NIMDTA Awaiting results of recontamination studies UCL Awaiting amendments to HTM 01-05
 04 DHSSPS reviewed in summer 2011 –Meetings HSCB, RQIA & NIMDTA DHSSPS further reviewed in summer/autumn 2012 –Meetings BDA, HSCB, RQIA & NIMDTA Awaiting results of recontamination studies UCL Awaiting amendments to HTM 01-05")
14
PEL(12)23 IssueHTM01-05 (DH Position)DHSSPS Position Timescales (Unchanged) Working at or above Essential requirements 1 yr from November 2009; Detailed plan to move to best practice All practices to have achieved best practice by November 2012 Manual cleaning (Unchanged/clarificati on) Every practice meeting essential requirements ‘validated decontamination cycle’ Best practice- Washer disinfector Manual cleaning not a validated process; Require Washer disinfector; (best practice) Manual cleaning; instruments where manufacturer specifies no WD or WD temporarily unavailable ( written protocol) LDU Room Layouts (Unchanged/clarificati on) 3 exemplar room layoutsFig 1 unacceptable no WD. Fig 2 & 3 acceptable. Need separate room Packaging Instruments processed type N (Changed/Amended) Permits drying & wrapping after processing type N & storage 21 days 21 days storage type N wrapped instruments 60 days storage type B wrapped instruments Non wrapped stored & used in working day Packaging & Storage of instruments ( New) 4.26 store with use-by date 4.29 If stored in clinical area for use on current patients, purpose designed cabinet Clearly dated ‘use by’ Stored in clinical area for use on patients within clinical session – dedicated storage cabinet
 Permits drying & wrapping after processing type N & storage 21 days 21 days storage type N wrapped instruments 60 days storage type B wrapped instruments Non wrapped stored & used in working day Packaging & Storage of instruments ( New) 4.26 store with use-by date 4.29 If stored in clinical area for use on current patients, purpose designed cabinet Clearly dated ‘use by’ Stored in clinical area for use on patients within clinical session – dedicated storage cabinet.")
15
PEL(12)23 Refer to full HTM 01-05 document DH reviewing storage times – DHSSPS will review guidance as appropriate Dental hand-pieces –advice from manufacturers as to which sterilisation cycle most suitable (4.5 HTM 01-05) Advice from Health Estates Investment Group – John Singh
23 Refer to full HTM document DH reviewing storage times – DHSSPS will review guidance as appropriate Dental hand-pieces –advice from manufacturers as to which sterilisation cycle most suitable (4.5 HTM 01-05) Advice from Health Estates Investment Group – John Singh")
16
Minimum Standards for Dental Care and Treatment RQIA will inspect against HSCB will commission against Std 13.4:’Prevention & Control of Infection’ ‘Your dental service meets current best practice on the decontamination of reusable dental & medical instruments’. RQIA will inspect 13.4 in 2013/14 DHSSPS/RQIA: Agreed inspection criteria

17
GDS Budget Structure/Trend/Savings Proposals

18
DHSSPS Structure CDO Minister Permanent Secretary & Deputy Secretaries HEIGSQS Primary Care Public Health HRD Local decontamination Capital planning Regulation of private dentistry Dental standards RQIA GDS contract CDS Oral health improvement Health protection Workforce Occupational health Dental school School of hygiene

19
New HSC structures Independent Assurance Performance Management Department HSCB (Including LCGs) Trusts PHA BSO RQIAPCC Agencies NDPBs Key Stakeholders GDS
 Trusts PHA BSO RQIAPCC Agencies NDPBs Key Stakeholders GDS")
20
GDS Budget – Structure

21
GDS Budget – Allocation Mechanism

22
GDS Budget – Structure Net Patient Pressure

23
GDS Budget – Investments £4 million (recurrent) into practice allowance ( total approx £8.6 million) £3 million (non-recurrent) into QIS £500k (recurrent) into VT grants £2.33m (recurrent) into extending registration period £400k (recurrent) salaried dental services £5.7 million Improve access via dental tender £1.1 (recurrent) into commitment payments
 into practice allowance ( total approx £8.6 million) £3 million (non-recurrent) into QIS £500k (recurrent) into VT grants £2.33m (recurrent) into extending registration period £400k (recurrent) salaried dental services £5.7 million Improve access via dental tender £1.1 (recurrent) into commitment payments")
24
Dentistry: other investments Capitation fees (deprived) ↑ 100% 0-5 yo;↑ 50% 6- 17yo Continuing Care (all) ↑ 15% & ↑ 50% (deprived) £120k CPD for DCPs £300k for 5 additional dental students £3 million re-equip school of dentistry £100k additional registrar posts Occupational health services for the whole dental team
 ↑ 100% 0-5 yo;↑ 50% 6- 17yo Continuing Care (all) ↑ 15% & ↑ 50% (deprived) £120k CPD for DCPs £300k for 5 additional dental students £3 million re-equip school of dentistry £100k additional registrar posts Occupational health services for the whole dental team")
25
GDS Budget: Proportion of Earnings 2006/072007/082008/092009/102010/112011/12 Items of Service 65.6%62.3%58.3%59.5%59.3%58.4% Capitation & Continuing Care 21.6%21.0%21.9%23.2%22.6%23.4% Block Payments (allowances) 12.7%16.8%19.8%17.3%18.1%18.2%
 12.7%16.8%19.8%17.3%18.1%18.2%")
26
GDP – Taxable Income net income* 2007/082008/092009/102010/11 Principal £121,200£129,600£122,900£114,200 Associate £66,100£66,700£62,700£59,400 *Estimates of taxable income are not affected by flows of money between principals and associates

27
GDS Budget – increased provision

28
GDS Budget

29
GDS Budget: Market Changes

31
GDS Budget: Proposals for Savings- Principles Must have potential to realise savings for GDS budget Can be implemented within existing GDS contract or with minor regulatory change Can be implemented within coming financial year Must be consistent with direction of new GDS contract Comply with equality legislation & other regulatory requirements.

32
GDS Budget – Proposals for Savings QIS- £1.16m transfer to GDS budget (done) Core service ( consistent with PDCS) Molar endo – prior approval Co/Cr – prior approval Bridgework – posterior/large; prior approval Veneers -all prior approval Alter time bar on S&P (evidence base absent)
 Core service ( consistent with PDCS) Molar endo – prior approval Co/Cr – prior approval Bridgework – posterior/large; prior approval Veneers -all prior approval Alter time bar on S&P (evidence base absent)")
33
GDS Budget – Proposals for Savings Orthodontic treatment – IOTN 3.6, all other ortho prior approval (consistent with PDCS & rest UK) Practice allowance –new criteria Average of 750 patients/DS, with average 200 fee paying Removal of commitment payments
 Practice allowance –new criteria Average of 750 patients/DS, with average 200 fee paying Removal of commitment payments")
34
Scale & Polish No evidence to support the clinical effectiveness of single S&P, nor frequency of provision –Cochrane Collaboration (Beirne, Worthington & Clarkson, 2008) –Clinical Outcomes of Single-Visit Oral Prophylaxis (Jones; Milsolm et al 2011) Item 10c number claims = 813 Item 10a number claims = 602,743 Item 10b number claims = 47,760 Perio SOD number contacts = 4,800
 –Clinical Outcomes of Single-Visit Oral Prophylaxis (Jones; Milsolm et al 2011) Item 10c number claims = 813 Item 10a number claims = 602,743 Item 10b number claims = 47,760 Perio SOD number contacts = 4,800")
35
ADHS (2009) 15% periodontally healthy (no bleeding or calculus/LOA <4mm) 41% periodontally healthy( LOA <4mm) but had calculus bleeding 44% LOA>4mm would require 10c or perio department SOD Adult registration 55% = 645,480 patients Approx 284,000 patients need item 10c?
 15% periodontally healthy (no bleeding or calculus/LOA <4mm) 41% periodontally healthy( LOA <4mm) but had calculus bleeding 44% LOA>4mm would require 10c or perio department SOD Adult registration 55% = 645,480 patients Approx 284,000 patients need item 10c")
36
GDS Budget: Potential Savings Move to a core service under the SDR: ~ £840k Altering claims conditions on S&P: ~ £744.5k Changes to the practice allowance: ~£500k Ceasing commitment payment: ~ £3.1m Restricting orthodontic treatment to IOTN 3.6: ~£1.7m ( realised over a 24 month period) Total = £6.8million (approx)
 Total = £6.8million (approx)")
37
Process & Timelines Consultation closes 3 April 2013 Consideration stage Minister signs off IOTN & commitment payment –regulatory change – Health committee Core service, S&P, practice allowance – SDR changes;

38
The Health Service - 65 Years old “We shall never have all we need. Expectations will always exceed capacity. The service must always be changing, growing and improving – it must always appear inadequate.” Aneurin Bevan - 1948

39
New Dental Contract

40
Primary Dental Care Strategy 2006 Local commissioning of services; Access to appropriate dental care for everyone who needs it; A clear definition of treatments available under the health service; A greater emphasis on disease prevention; Guaranteed out-of-hours services; A revised remuneration system, which rewards dentists fairly for operating the new arrangements.

41
Problems with existing system Quantity not quality is rewarded; Treatment rather than prevention is rewarded; Demand led rather than needs led; SDR > 400 items is administratively complex; Patient charges are difficult for the public to understand

42
Problems with existing system Dentists incomes directly related to the volume of treatment provided causes remuneration treadmill; HSCB lacks control over targeting services at areas and patients with greatest need. 50 year old system no longer meets the needs of patients, oral health care professionals or society at large.

44
Care Payments Quality care payments (QCPs) Practice environment indicators Practice inspection Recognised charter-mark Practitioner indicators Peer review / clinical audit Higher qualification
 Practice environment indicators Practice inspection Recognised charter-mark Practitioner indicators Peer review / clinical audit Higher qualification")
46
Patient Care Payment Weighted Capitation formula Adjusted for Age Adjusted gender Adjusted for additional needs Adjusted for ‘new patients’ Adjusted for list turnover

47
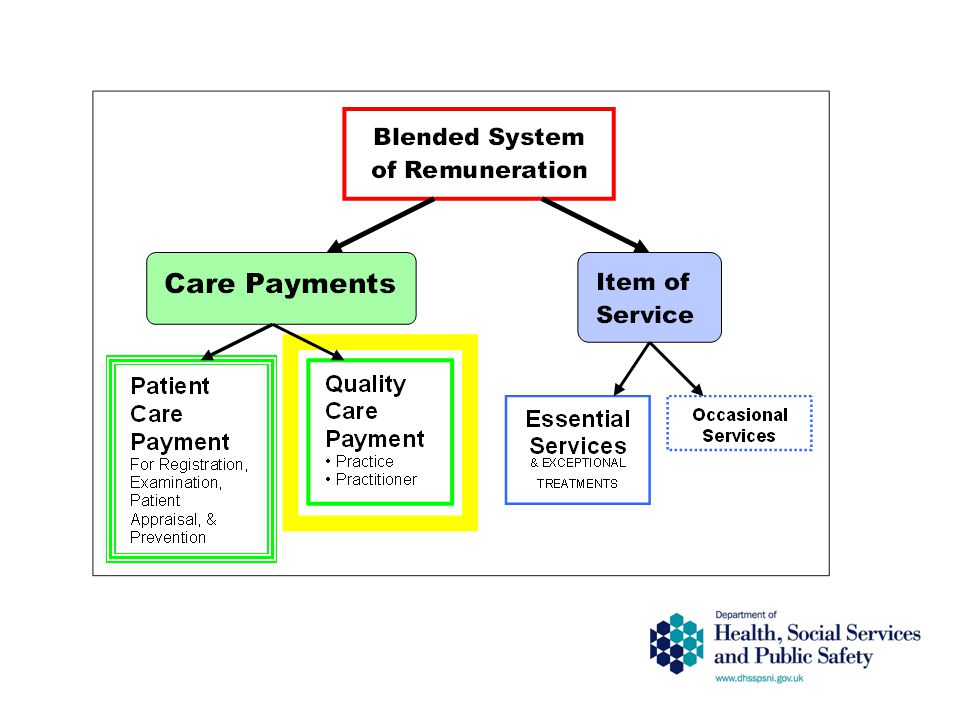
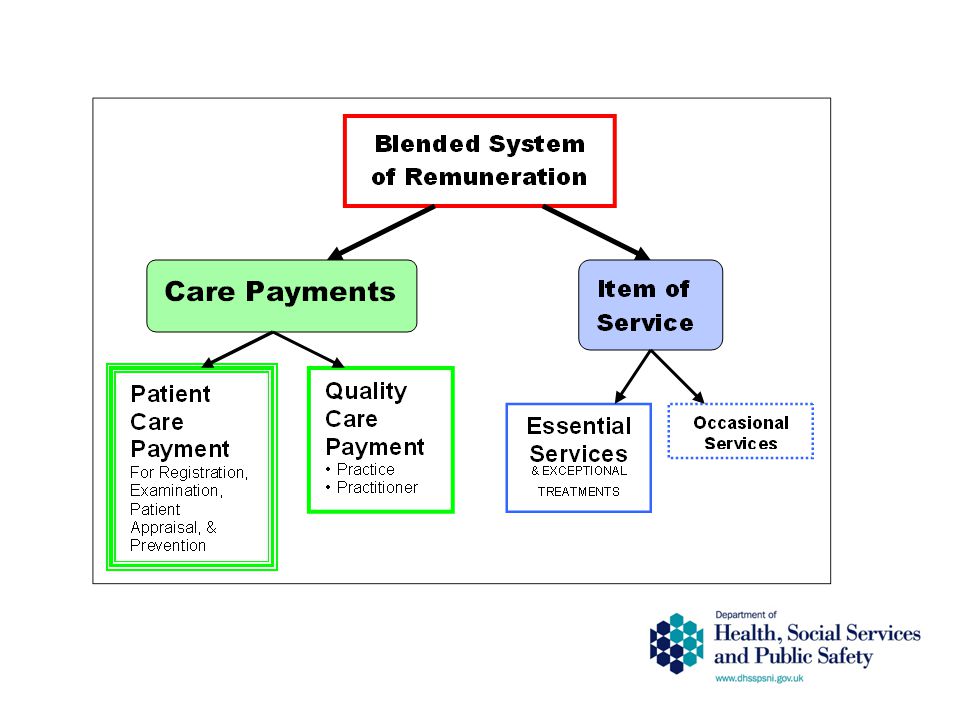
Care Payments Patient Care Payment For Registration, Examination, Patient Appraisal, Prevention & Necessary Treatment Patient Care Payment For Registration, Examination, Patient Appraisal, Prevention & Necessary Treatment Quality Care Payment Practice Practitioner Quality Care Payment Practice Practitioner Capitation and Quality Payment Model Care Payments Patient Care Payment For Registration, Examination, Patient Appraisal, Prevention & Necessary Treatment Patient Care Payment For Registration, Examination, Patient Appraisal, Prevention & Necessary Treatment Quality Care Payment Practice Practitioner Quality Care Payment Practice Practitioner

48
Why has it taken so long? Resources Addressing access issue IT system at BSO GDS budget – controlling pressures Legislative problems – e.g. pensions, performers lists Proposals from BDA?

49
How will new contract impact on profession? Local commissioning – HSCB will target resource at need. Control of entry – commissioning /performers lists Fixed GDS budget and global sum formula Focus on prevention Out of hours responsibility of HSCB

50
What’s in for Profession? Limits number of dental practices Increase value of practices? Can opt out of Out of Hours –Work-life balance? Performer/provider contracts Career structure? Capitation payments Improved cash flow Global sum More stable budgetary position ?

51
More information Visit www.dhsspsni.gov.uk/pgroups/dental/dental.asp CDO... News Updates from the Chief Dental Officer What's New Dental related information on events, news and publications other than those directly from Dental Branch Publications Material published by Dental Branch, or to which Dental Branch has made a substantive contribution

52
Thank You

Similar presentations



















 4 October 2012.>")
. Overview Provide an overview of the formula headlines Final schools funding formula 2015/16 Base Formula.>")