Download presentation
Presentation is loading. Please wait.

1
Relapsed and Refractory Myeloma
Ruben Niesvizky Myeloma Center Myelomacenter.org

2
Multiple Myeloma: Natural History of Disease
Asymptomatic Symptomatic Relapsing Refractory M-Protein Level Remission duration decreases with each line of therapy Active Myeloma Relapse Remission MGUS or Indolent Myeloma // // Second- or Third-Line Therapy Frontline Therapy Durie B; International Myeloma Foundation. Concise review of the disease and treatment options: multiple myeloma. 2011/2012 edition; Kumar SK, et al. Mayo Clin Proc. 2004;79:

3
Outline Approach to the patient with RRMM: Proteasome inhibitors
Evidence based Factors to be considered in selecting therapy Proteasome inhibitors Inmunomodulatory Agents HDAC inhibitors Alkylating agents

4
Clinical Considerations for Relapsed/Refractory Disease
Disease characteristics/prior therapy Line of therapy Plateau phase=quiescent period Aggressiveness of relapse Relapsed or relapsed and refractory disease “High risk disease” Prior therapies (eg SCT, prior IMiD, bortezomib-based therapy)
")
5
Clinical Considerations for Relapsed/Refractory Disease
Disease characteristics/prior therapy Line of therapy Plateau phase=quiescent period Aggressiveness of relapse Relapsed or relapsed and refractory disease “High risk disease” Prior therapies (eg SCT, prior IMiD, bortezomib-based therapy)
")
6
Response Duration Decreases With Successive Therapies
578 patients; median age 65 years (follow up 55 months) Overall survival One year 72% Two years 55% Three years 22% 84% died within five years Kumar SK, et al. Mayo Clin Proc. 2004;79:
 Overall survival. One year 72% Two years 55% Three years 22% 84% died within five years. Kumar SK, et al. Mayo Clin Proc. 2004;79:")
7
APEX: Bortezomib Early or Late Relapse
1 prior therapy n = 132 > 1 prior therapy n = 200 Median TTP (months) 7.0 4.9 CR (%) 10%* 7%† CR + PR (%) 51%* 37%† Median Duration of Response (months) 8.1 7.8 1-year Survival 89% 73% * Evaluable patients, response to bortezomib after 1 prior therapy: n = 128 † Evaluable patients, response to bortezomib after >1 prior therapy: n = 187 Sonneveld P, et al. Haematologica. 2005;90: Abstract P ; Data on file; Millennium Pharmaceuticals, Inc.
 CR (%) 10%* 7%† CR + PR (%) 51%* 37%† Median Duration of Response (months) year Survival. 89% 73% * Evaluable patients, response to bortezomib after 1 prior therapy: n = 128. † Evaluable patients, response to bortezomib after >1 prior therapy: n = 187. Sonneveld P, et al. Haematologica. 2005;90: Abstract P ; Data on file; Millennium Pharmaceuticals, Inc.")
8
Improved Outcomes with the Early Use of LenDex : TTP and OS
Time to Progression Overall Survival 2nd Line (LenDex) Median 17.1 months ≥ 3th line(LenDex) Median 10.6 months 2nd Line (LenDex) Median 42 months ≥ 3th line(LenDex) Median 35.8 month Stadmauer EA et al. Eur J Haematol 2009; 82:426-32
 Median 17.1 months. ≥ 3th line(LenDex) Median 10.6 months. 2nd Line (LenDex) Median 42 months. ≥ 3th line(LenDex) Median 35.8 month. Stadmauer EA et al. Eur J Haematol 2009; 82:")
9
Clinical Considerations for Relapsed/Refractory Disease
Disease characteristics/prior therapy Line of therapy Plateau phase=quiescent period Aggressiveness of relapse Relapsed or relapsed and refractory disease “High risk disease” Prior therapies (eg SCT, prior IMiD, bortezomib-based therapy)
")
10
Time to Progression After SCT Correlates With OS After Initial Relapse
Kumar SK, et al. Bone Marrow Transplant. 2008;42:

11
Clinical Considerations for Relapsed/Refractory Disease
Disease characteristics/prior therapy Line of therapy Plateau phase=quiescent period Aggressiveness of relapse Relapsed or relapsed and refractory disease “High risk disease” Prior therapies (eg SCT, prior IMiD, bortezomib-based therapy)
")
12
Frontline vs Relapsed Refractory
Treatment Naive Response to Therapy Survival Outcomes High risk features Genomic instability Relapsed and Refractory Response to Therapy Survival Outcomes Toxicities and Co-morbidities Toxicities and Co-morbidities

13
Outcomes in Relapsed and Refractory Multiple Myeloma
Frontline Treatment Relapsed Relapsed /Refractory Expected survival (months) 20-50 Sensitivity to therapy Sensitive Treatment limitations/ comorbidities Peripheral neuropathy (~15% at diagnosis) 14-16 Less Sensitive/Resistant >80% incidence of peripheral neuropathy Compromised marrow reserve Cytopenia 6-10 Resistant Intolerant to or ineligible for available therapy Elderly population ( risk for heart, lung, renal, liver dysfunction, diabetes) Adapted from: Durie BGM. Multiple Myeloma. International Myeloma Foundation. 2011/2012 edition. Jagannath S. Clin Lymphoma Myeloma. 2008;8 Suppl 4:S149-S156. For Training and Educational Purposes Only. Not for Distribution.
 Sensitivity to. therapy. Sensitive. Treatment limitations/ comorbidities. Peripheral neuropathy (~15% at diagnosis) Less Sensitive/Resistant. >80% incidence of peripheral neuropathy Compromised marrow reserve. Cytopenia Resistant. Intolerant to or. ineligible for available therapy. Elderly population ( risk for heart, lung, renal, liver dysfunction, diabetes) Adapted from: Durie BGM. Multiple Myeloma. International Myeloma Foundation. 2011/2012 edition. Jagannath S. Clin Lymphoma Myeloma. 2008;8 Suppl 4:S149-S156. For Training and Educational Purposes Only. Not for Distribution.")
14
Nature of Relapse How did the patient present?
80% share clinical features with presentation Has been a shift on presentation? Intact immunoglobulin to light chain only Non-secretory relapse Extra medullar disease

16
Nature of Relapse How did the patient present?
80% share clinical features with presentation 35% relapse both light chain and intact Ig 49.6% intact Ig 10% free light chain only

17
Survival according to paraprotein and FLC secretion at first relapse.
Brioli A et al. Blood 2014;123: ©2014 by American Society of Hematology

18
Survival from relapse according to paraprotein and FLC secretion at relapse for patients with IgG and IgA paraproteins. Brioli A et al. Blood 2014;123: ©2014 by American Society of Hematology

19
Nature of Relapse How did the patient present?
80% share clinical features with presentation 35% relapse both light chain and intact Ig 49.6% intact Ig 10% free light chain only Has been a shift on presentation? Intact immunoglobulin to light chain only Non-secretory relapse Extra medullar disease

21
Progression-free survival according to the presence of extramedullary (EM) involvement at diagnosis.
Varettoni M et al. Ann Oncol 2009;21: © The Author Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please

22
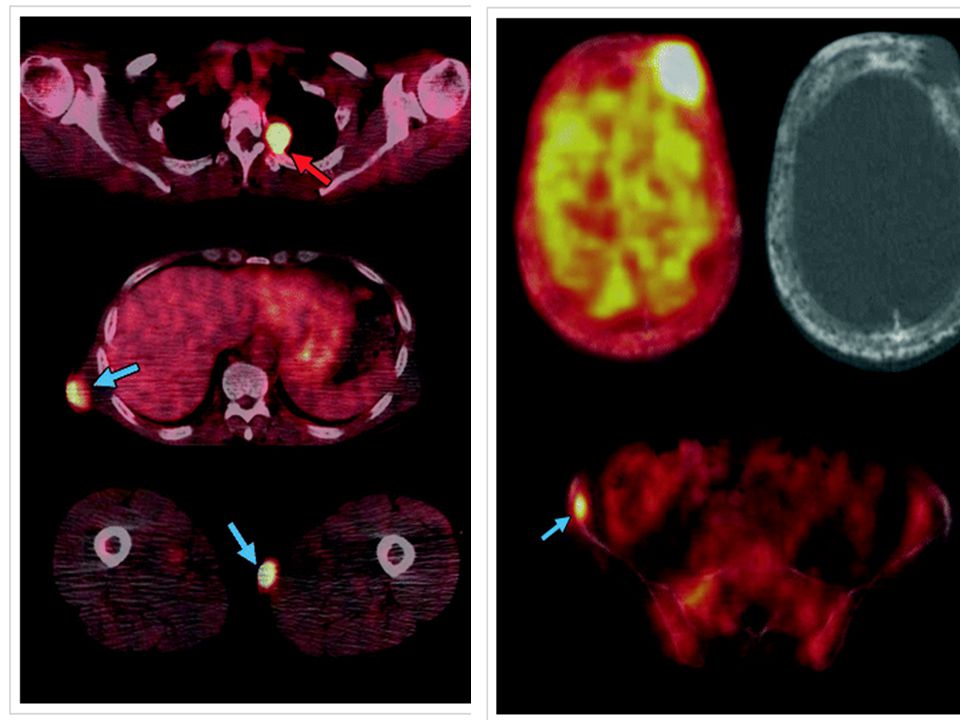
Outcome according to baseline PET/CT.
Zamagni E et al. Blood 2011;118: ©2011 by American Society of Hematology

23
Patient Heterogeneity

24
Clinical Considerations for Relapsed/Refractory Disease
Toxicity considerations Peripheral neuropathy Thrombotic risk Myelosuppression Impact of prior therapies (eg, SCT, other cumulative toxicity)
")
25
Overall survival in 6-year intervals from time of diagnosis
ANY PROGRESS? Overall survival in 6-year intervals from time of diagnosis Time (months) Proportion of patients 0.2 0.4 0.6 0.8 1.0 20 40 60 80 100 120 140 2001–2006 1995–2000 1989–1994 1983–1988 1977–1982 1971–1976 Kumar et al. Blood. 2008 Brenner et al. Blood. 2008 25 25
 Proportion of patients – – – – – –1976. Kumar et al. Blood Brenner et al. Blood")
27
< 65 años > 65 años Kumar et al: Leukemia Nov 2013

28
Proteosome Inhibitors
Bortezomib Carflizomib Ixazomib Oprozomib

29
Proteasome Inhibitors
Outcomes Correlate with Depth of Response

30
Quality of Response: Survival
Niesvizky et al., Br J Haematol Oct;143(1):46-53
:")
31
Proteasome Inhibitors
Benefits of Retreatment

32
Bortezomib Retreatment – A Retrospective Multicenter Survey
Retrospectively collected data- multicenter non-interventional survey of pts who received bortezomib for a second time (retreatment) Patients: 65 pts,19 centers; median age 65 yrs Treatment received Median 4 prior therapies Retreatment Initial bortezomib Diagnosis 52 mos Mean of 5 cycles Mean of 4 cycles 6 pts received additional therapy Median Bortezomib mg/m2 Initial Re-treatment 1.3 94% 86% 1.0 2% 12% other 8% 4% + Dex 39% 61% Results: 49 evaluable (modified ITT) Retreatment Best Response Treatment Outcomes Safety: AE occurring in > 2 patients % Patients months Patients (n) Hrusovsky I, et al. ASH 2007, abstract #2720
 Patients: 65 pts,19 centers; median age 65 yrs. Treatment received. Median 4 prior therapies. Retreatment. Initial. bortezomib. Diagnosis. 52 mos. Mean of 5 cycles. Mean of 4 cycles. 6 pts received additional therapy. Median. Bortezomib mg/m2. Initial. Re-treatment % 86% % 12% other. 8% 4% + Dex. 39% 61% Results: 49 evaluable (modified ITT) Retreatment. Best Response. Treatment Outcomes. Safety: AE occurring in > 2 patients. % Patients. months. Patients (n) Hrusovsky I, et al. ASH 2007, abstract #2720.")
33
Petrucci et al, Br J Haem 2013,160,649-659

34
Petrucci et al, Br J Haem 2013,160,649-659

35
Proteasome Inhibitors
Carflilzomib

36
Study 003-A1: Open-Label Phase 2b Study of Single-Agent Carfilzomib in Relapsed and Refractory Multiple Myeloma (R/R MM) Study Population (N=266) Relapsed from ≥2 prior lines of therapy Must include bortezomib Must include thalidomide or lenalidomide Refractory to last regimen Carfilzomib IV on days 1, 2, 8, 9, 15 and 16 every 28 days 20 mg/m2 in Cycle 1 and 27 mg/m2 from Cycle 2 and beyond (maximum 12 cycles) Primary endpoint: ORR IMWG response criteria (IRC assessed) Secondary endpoints CBR (ORR+ MR), DOR, OS, PFS, TTP, safety CBR = clinical benefit rate; DOR = duration of response; IMWG = International Myeloma Working Group; IRC = Independent Review Committee; MR = minimal response; ORR = overall response rate; OS = overall survival; PFS = progression-free survival Siegel D, et al. Blood. 2012;120:
 Relapsed from ≥2 prior lines of therapy. Must include bortezomib. Must include thalidomide or lenalidomide. Refractory to last regimen. Carfilzomib IV on days 1, 2, 8, 9, 15 and 16 every 28 days. 20 mg/m2 in Cycle 1. and 27 mg/m2 from Cycle 2 and beyond. (maximum 12 cycles) Primary endpoint: ORR. IMWG response criteria (IRC assessed) Secondary endpoints. CBR (ORR+ MR), DOR, OS, PFS, TTP, safety. CBR = clinical benefit rate; DOR = duration of response; IMWG = International Myeloma Working Group; IRC = Independent Review Committee; MR = minimal response; ORR = overall response rate; OS = overall survival; PFS = progression-free survival. Siegel D, et al. Blood. 2012;120:")
37
Single-Agent Carfilzomib: Response Rates
TTR: 1.9 mo (≥PR) and 1.0 mo (≥MR) DOR: 7.8 mo (≥PR) and 8.3 mo (≥MR) N = 257 response-evaluable population DCR = 69% Percentage of Patients CBR = 37% ORR = 24% Subset analyses of higher risk populations showed similar response rates (e.g., unfavorable cytogenetics, baseline peripheral neuropathy) CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease; TTR = time to response; VGPR = very good partial response Siegel D, et al. Blood. 2012;120: *IRC-determined; 11 patients had unconfirmed response
 and 1.0 mo (≥MR) DOR: 7.8 mo (≥PR) and 8.3 mo (≥MR) N = 257 response-evaluable population. DCR = 69% Percentage of Patients. CBR = 37% ORR = 24% Subset analyses of higher risk populations showed similar response rates (e.g., unfavorable cytogenetics, baseline peripheral neuropathy) CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease; TTR = time to response; VGPR = very good partial response. Siegel D, et al. Blood. 2012;120: *IRC-determined; 11 patients had unconfirmed response.")
38
Single-Agent Carfilzomib: PFS, OS
1.0 0.8 0.6 0.4 0.2 0.0 3 9 12 18 6 15 3 12 21 27 1.0 0.8 0.6 0.4 0.2 0.0 15 6 9 18 24 Median OS = 15.6 mo (95% CI 13.0–19.2) Median PFS = 3.7 mo (95% CI 2.8–4.6) Proportion alive and without progression Proportion surviving Months N = 257 response-evaluable population Months Siegel D, et al. Blood. 2012;120: 38
 Median PFS = 3.7 mo (95% CI 2.8–4.6) Proportion alive and without progression. Proportion surviving. Months. N = 257 response-evaluable population. Months. Siegel D, et al. Blood. 2012;120:")
40
Phase II Trial of Carfilzomib Plus Len/Dex in R/R MM (1-3 prior lines of therapy)
Carfilzomib 20/27 mg/m2 IV* *20 mg/m2 cycle 1 days 1 and 2 only, 27 mg/m2 thereafter D1/D2 D8/D9 D15/D16 Week 1 Week 2 Week 3 Week 4: rest Lenalidomide d1-d21 25 mg/d PO D1 D8 D15 D22 Dexamethasone 40 mg/d PO Response (N = 52 pts receiving maximal planned dose) n (%) ORR Stringent CR CR VGPR PR SD 40 (77) 2 (4) 1 (2) 19 (37) 18 (35) 3 (6) Median duration of response, mos (range) 22.1 ( ) Wang M, et al. Blood. 2013;122: 40 40
 n (%) ORR. Stringent CR. CR. VGPR. PR. SD. 40 (77) 2 (4) 1 (2) 19 (37) 18 (35) 3 (6) Median duration of response, mos (range) 22.1 ( ) Wang M, et al. Blood. 2013;122:")
41
For ASH Dec 09 Phase III ASPIRE Trial: Carfilzomib + Len/Dex vs Len/Dex in R/R MM (ongoing) Press release- PFS 26.3 vs 17.6 HR 0.69: CRd Carfilzomib 27 mg/m2 IV day 1, 2, 8, 9, 15, and 16 (20 mg/m2 on days 1, 2 of cycle 1 only) Lenalidomide 25 mg Days 1-21 Dexamethasone 40 mg once weekly Study Population (N=780) Measurable disease 1-3 prior regimens Relapse or PD Response to ≥1 prior regimen Exclusion factors: Bortezomib-refractory Len/dex-refractory Prior carfilzomib Rd Lenalidomide 25 mg Days 1-21 Dexamethasone 40 mg once weekly Stratify: Prior bortezomib, prior lenalidomide, β2 microglobulin level Primary endpoint: PFS 28-day cycles Available at: Accessed April 29, 2014. DRAFT 41
 Lenalidomide. 25 mg Days Dexamethasone. 40 mg once weekly. Study Population (N=780) Measurable disease. 1-3 prior regimens. Relapse or PD. Response to ≥1 prior regimen. Exclusion factors: Bortezomib-refractory. Len/dex-refractory. Prior carfilzomib. Rd. Lenalidomide. 25 mg Days Dexamethasone. 40 mg once weekly. Stratify: Prior bortezomib, prior lenalidomide, β2 microglobulin level. Primary endpoint: PFS. 28-day cycles. Available at: Accessed April 29, DRAFT. 41.")
42
Phase 1b Study of High-Dose Carfilzomib + Dexamethasone in R/R MM
Endpoint CFZ 20/45 20/56 Total ORR, % 57 50 55 CR, % VGPR, % 14 25 PR, % 43 30 DOR NR PFS, months 5.4 6.0 Study population: N=22 (expanded 007 cohort) Median prior regimens: 4 Regimen: (28-day cycles) Carfilzomib 20/45 or 20/56 mg/m2 30-min IV D1,2,8,9,15,16 Dexamethasone 20 mg D1,2,8,9,15,16 then 40 mg D22 Efficacy Treatment-emergent Grade ≥3 AE, % CFZ 20/45 20/56 Total Hematologic Thrombocytopenia Anemia Lymphopenia 29 14 50 25 36 27 18 Nonhematologic Hypertension Hypophosphatemia Pneumonia 7 13 9 Safety CFZ = carfilzomib Badros A, et al. ASH Abstract 4036.
 Median prior regimens: 4. Regimen: (28-day cycles) Carfilzomib 20/45 or 20/56 mg/m2 30-min IV D1,2,8,9,15,16. Dexamethasone 20 mg. D1,2,8,9,15,16 then 40 mg D22. Efficacy. Treatment-emergent Grade ≥3 AE, % CFZ. 20/45. 20/56. Total. Hematologic. Thrombocytopenia. Anemia. Lymphopenia Nonhematologic. Hypertension. Hypophosphatemia. Pneumonia Safety. CFZ = carfilzomib. Badros A, et al. ASH Abstract")
43
Phase III ENDEAVOR: Carfilzomib + Dex vs Bortezomib/Dex in R/R MM1
Note use of higher carfilzomib dose—based on results from 004 trial, which suggested dose-response relationship of carfilzomib2 Cd Carfilzomib 20/56 mg/m2 IV D1,2, 8, 9, 15, 16 Dexamethasone 20 mg PO or IV D1, 2, 8, 9, 15, 16, 22, 23 28-day cycle Study Population (N=888) Measurable disease Responsive to at least 1 prior therapy Relapsed following 1-3 prior treatment regimens ECOG PS 0-2 Vd Bortezomib 1.3 mg/m2 IV or SC D1, 4, 8, & 11 Dexamethasone 20 mg PO or IV D1, 2, 4, 5, 8, 9, 11, 12 21-day cycle Stratify: Prior PI, prior lines of therapy, ISS, bortezomib IV vs. SC Primary endpoint: PFS Treat until PD or unacceptable toxicity ClinicalTrials.gov. Available at: Accessed March 26, 2014. Vij R, et al. Blood. 2012;119:
 Measurable disease. Responsive to at least 1 prior therapy. Relapsed following 1-3 prior treatment regimens. ECOG PS 0-2. Vd. Bortezomib. 1.3 mg/m2 IV or SC D1, 4, 8, & 11. Dexamethasone. 20 mg PO or IV D1, 2, 4, 5, 8, 9, 11, day cycle. Stratify: Prior PI, prior lines of therapy, ISS, bortezomib IV vs. SC. Primary endpoint: PFS. Treat until PD or unacceptable toxicity. ClinicalTrials.gov. Available at: Accessed March 26, Vij R, et al. Blood. 2012;119:")
44
Novel PIs Under Investigation in R/R MM
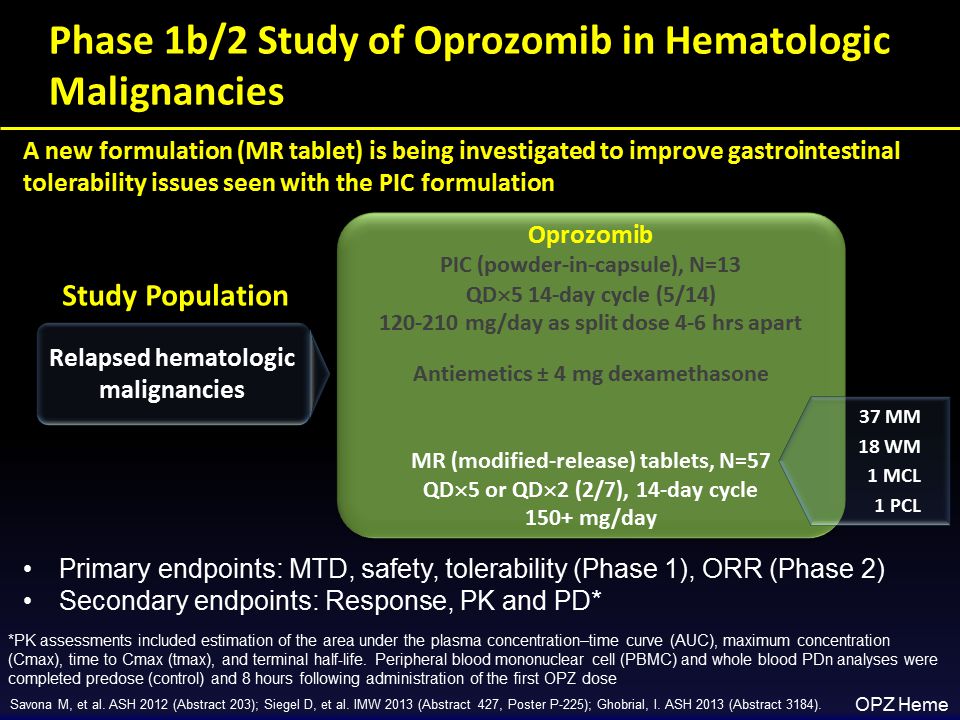
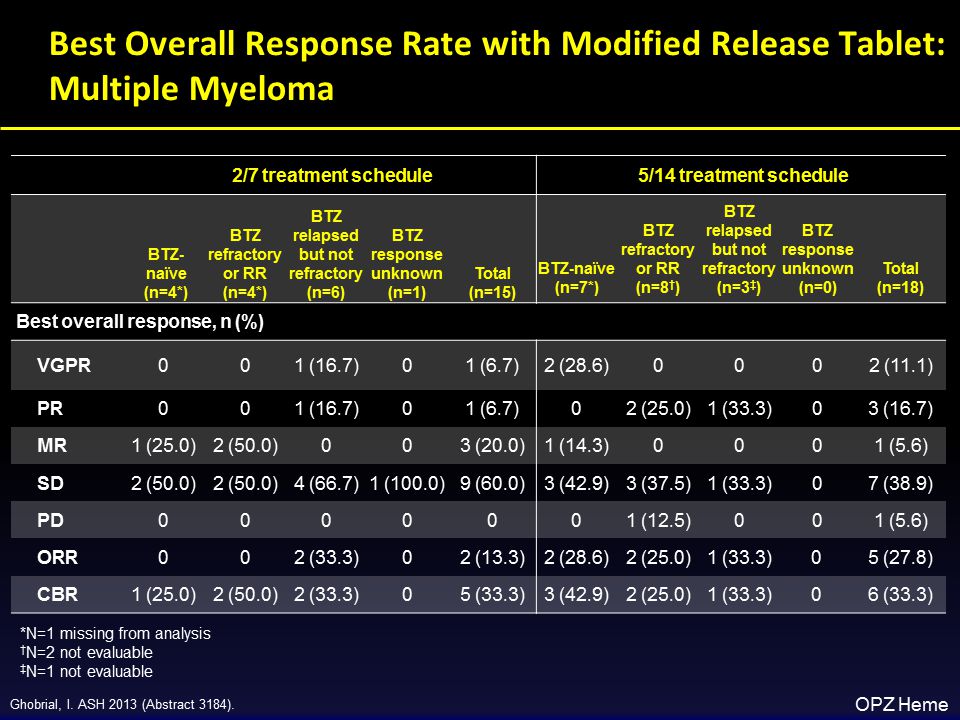
Agent Status Ixazomib Two phase I studies showed activity of single-agent ixazomib[2,3] Oprozomib Phase 1 dose-escalation study showed some activity in patients with heavily pretreated hematologic malignancies, including MM[4] Richardson PG, et al. ASH Abstract 302. Lonial S, et al. ASCO Abstract 8017. Kumar S, et al. ASCO Abstract 8514. Savona MR, et al. ASH Abstract 203.

45
Ixazomib: Oral Proteasome Inhibitor

46
Ixazomib treatment duration and response.
Kumar S K et al. Blood 2014;124: ©2014 by American Society of Hematology

47
Proteasome Inhibitors
Oprozomib

52
OPomDex Study Design (Phase 1b)
")
53
Proteosome Inhibitors
Bortezomib Carflizomib Ixazomib Oprozomib Immunomodulating Agents Ub Substrates + Thalidomide Lenalidomide Pomalidomide

54
Immunomodulating Agents

55
Pomalidomide in Relapsed/Refractory Multiple Myeloma
POM + LoDEX achieved responses in pts with prior LEN and/or BORT treatment, including those who are refractory1-4 Study Phase N Treatment Population Median Prior Tx (Range) ≥ PR Lacy4 2 60 POM: 2 mg (28/28-day cycle) Dex: 40 mg/week 1-3 prior Tx, relapsed/refractory 2 (1-3) 65% 34 LEN-refractory 4 (1-14) 32% 35 DEX: 40 mg/week LEN- and BORT- refractory 6 (3-9) 26% POM: 4 mg 1-3 prior Tx, LEN-refractory 37% 6 (2-11) 29% 1. Lacy MQ et al. J Clin Oncol. 2009;27: Lacy MQ et al. Leukemia. 2010;24:1934. 3. Lacy MQ et al. Blood. 2011;118: Lacy MQ et al. Blood. 2011;118: Abstract 3963. 55
 ≥ PR. Lacy POM: 2 mg. (28/28-day cycle) Dex: 40 mg/week. 1-3 prior Tx, relapsed/refractory. 2 (1-3) 65% 34. LEN-refractory. 4 (1-14) 32% 35. DEX: 40 mg/week. LEN- and BORT- refractory. 6 (3-9) 26% POM: 4 mg. 1-3 prior Tx, LEN-refractory. 37% 6 (2-11) 29% 1. Lacy MQ et al. J Clin Oncol. 2009;27: Lacy MQ et al. Leukemia. 2010;24: Lacy MQ et al. Blood. 2011;118: Lacy MQ et al. Blood. 2011;118: Abstract")
56
Median No. Prior Regimens Refractory to Recent Therapy (%)
Pomalidomide Pts, n Median No. Prior Regimens Refractory to Recent Therapy (%) ORR (%) Pomalidomide ± dex1 191 5 100 2534 Pomalidomide, dex2 70 6 NR 2629 Pomalidomide, dex3 84 85 3435 Pomalidomide, cyclophosphamide, prednisone4 32 (1 to 3) 44* 59 Pomalidomide, dex, clarithromycin5 46 NR (at least 3) 60 *Len specifically 1. Vij R et al. J Clin Oncol. 2012;30. Abstract 8016. 2. Lacy MQ et al. Blood. 2011;118: Leleu X et al. Blood. 2011;118. Abstract 812. 4. Palumbo A et al. Blood. 2011;118. Abstract 632. Mark TM et al. Blood. 2011;118. Abstract 635.
 ORR (%) Pomalidomide ± dex 34. Pomalidomide, dex NR. 2629. Pomalidomide, dex 35. Pomalidomide, cyclophosphamide, prednisone (1 to 3) 44* 59. Pomalidomide, dex, clarithromycin NR (at least 3) 60. *Len specifically. 1. Vij R et al. J Clin Oncol. 2012;30. Abstract Lacy MQ et al. Blood. 2011;118: Leleu X et al. Blood. 2011;118. Abstract Palumbo A et al. Blood. 2011;118. Abstract 632. Mark TM et al. Blood. 2011;118. Abstract 635.")
57
ClaPd: Study Design Day
A single-center, phase 2 study of Clarithromycin combined with Pomalidomide + Low Dose Dexamethasone in RRMM Day Dex 40mg PO Pomalidomide 4 mg PO Clarithromycin 500mg PO BID p.o., orally; b.i.d., twice a day; RRMM, relapsed, refractory MM.

58
Clarithromycin???

59
Results Best Response (IMWG Criteria) n (%) Overall (N = 98)
ORR (≥ PR) 56 (57) CBR (≥ MR) 65 (66) sCR 6 (6) VGPR 17 (17) PR 33 (34) MR 9 (9) SD 23 (23) PD 10 (10) 98 patients completed at least 1 cycle of ClaPD. median number of cycles received was 6 (range 1–25) median study follow-up was months (range 1.0–25.6) In responding patients, median time to PR was 1 cycle (range 1–7). Median time to best response was 2 cycles (range 1-14). IMWG, International Myeloma Working Group; CBR, clinical benefit rate; MR, minimal response; PD, progressive disease; sCR, stringent complete response; SD, stable disease.
 56 (57) CBR (≥ MR) 65 (66) sCR. 6 (6) VGPR. 17 (17) PR. 33 (34) MR. 9 (9) SD. 23 (23) PD. 10 (10) 98 patients completed at least 1 cycle of ClaPD. median number of cycles received was 6 (range 1–25) median study follow-up was 9.6 months (range 1.0–25.6) In responding patients, median time to PR was 1 cycle (range 1–7). Median time to best response was 2 cycles (range 1-14). IMWG, International Myeloma Working Group; CBR, clinical benefit rate; MR, minimal response; PD, progressive disease; sCR, stringent complete response; SD, stable disease.")
60
Treatment History With Len/Bort Did Not Influence Response to ClaPD
Best Response (IMWG Criteria) n (%) Overall (N = 98) Lenalidomide refractory (N = 83) Bortezomib Refractory (N = 82) Lenalidomide and bortezomib refractory (N = 72) ORR (≥ PR) 56 (57) 47 (63) 46 (56) 39 (54) CBR (≥ MR) 65 (66) 56 (67) 54 (65) (65) sCR 6 (6) 6 (7) 5 (6) 5 (7) VGPR 17 (17) 13 (16) 9 (13) PR 33 (34) 28 (34) 25 (35) MR 9 (9) 8 (10) 8 (11) SD 23 (23) 18 (22) 19 (23) 16 (22) PD 10 (10) 8 (12) 9 (11) IMWG, International Myeloma Working Group; MR, minimal response; PD, progressive disease; sCR, stringent complete response; SD, stable disease.
 n (%) Overall. (N = 98) Lenalidomide. refractory. (N = 83) Bortezomib. Refractory. (N = 82) Lenalidomide and. bortezomib refractory. (N = 72) ORR (≥ PR) 56 (57) 47 (63) 46 (56) 39 (54) CBR (≥ MR) 65 (66) 56 (67) 54 (65) (65) sCR. 6 (6) 6 (7) 5 (6) 5 (7) VGPR. 17 (17) 13 (16) 9 (13) PR. 33 (34) 28 (34) 25 (35) MR. 9 (9) 8 (10) 8 (11) SD. 23 (23) 18 (22) 19 (23) 16 (22) PD. 10 (10) 8 (12) 9 (11) IMWG, International Myeloma Working Group; MR, minimal response; PD, progressive disease; sCR, stringent complete response; SD, stable disease.")
61
OS by double-refractory state
Results OS by cytogenetic risk OS by double-refractory state 1.00 1.00 0.75 0.75 Survival (%) 0.50 Survival (%) 0.50 Standard risk High risk Not double-refractory Double-refractory 0.25 0.25 Time (days) Time (days) Number of patients at risk Relapsed Refractory Number of patients at risk Relapsed Refractory Adverse cytogenetics did not appear to influence risk of death as of last study follow-up. HR 1.05, 95%CI (0.49,2.26), P = 0.888 A history of being double-refractory, however, approached a significant effect on survival time. HR 2.67, 95%CI (0.93,7.69), P = 0.068
 Survival (%) Standard risk. High risk. Not double-refractory. Double-refractory Time (days) Time (days) Number of patients at risk Relapsed Refractory Number of patients at risk Relapsed Refractory Adverse cytogenetics did not appear to influence risk of death as of last study follow-up. HR 1.05, 95%CI (0.49,2.26), P = A history of being double-refractory, however, approached a significant effect on survival time. HR 2.67, 95%CI (0.93,7.69), P =")
62
IFM 2010-02: Study design End-points Primary: TTP
RRMM Exposed to Len del 17p and/or t(4;14) Measurable disease ECOG 0–2 PNn > 1 x109/L Plat ≥ 75 x109/L Hb ≥ 8 g/dL CrCl ≥30 mL/min Pomalidomide 4 mg/day, po, days 1–21 (of 28 d cycle) Dexamethasone 40 mg, po, days 1, 8, 15, 22 Aspirin/LMWH once daily, continuously Until progression Safety analysis by DMC after 15 patients recruited End-points Primary: TTP Secondary: Safety, Response rate (CBR), DoR, OS, PFS, EFS, cytogenetic groups Median follow-up: 8.2 months At data cut-off, 36 patients (72%) had discontinued trial n (%) Progression 25 (69) Death other cause 1 (3) Toxicity 9 (25) Sponsor decision
 Measurable disease. ECOG 0–2. PNn > 1 x109/L. Plat ≥ 75 x109/L. Hb ≥ 8 g/dL. CrCl ≥30 mL/min. Pomalidomide 4 mg/day, po, days 1–21 (of 28 d cycle) Dexamethasone 40 mg, po, days 1, 8, 15, 22. Aspirin/LMWH once daily, continuously. Until progression. Safety analysis by DMC after 15 patients recruited. End-points. Primary: TTP. Secondary: Safety, Response rate (CBR), DoR, OS, PFS, EFS, cytogenetic groups. Median follow-up: 8.2 months. At data cut-off, 36 patients (72%) had discontinued trial. n (%) Progression. 25 (69) Death other cause. 1 (3) Toxicity. 9 (25) Sponsor decision.")
63
IFM 2010-02: Time To Progression (ITT)
del17p t(4;14) ITT O/N Median 95% CI ITT population 33 / 50 2.9 [2.7;5.0] 8-month TTP, % 22 del17p 12 / 22* 7.3 [2.7;14.7] 41 t(4;14) 24 / 32* 2.8 [1.9;4.0] 12.4
 ITT. O/N. Median. 95% CI. ITT population. 33 / [2.7;5.0] 8-month TTP, % 22. del17p. 12 / 22* 7.3. [2.7;14.7] 41. t(4;14) 24 / 32* 2.8. [1.9;4.0]")
64
IFM 2010-02: Overall Survival
O/N Median 95% CI ITT population 26 / 50 12 [4.9;15.5] 8-month OS, % 55 del17p 12 / 22* [2.4;-] 58 t(4;14) 16 / 32* 9.2 [4.6;-] 50
 16 / 32* 9.2. [4.6;-] 50.")
65
40 mg weekly (20 mg after cycle 4)
Phase I/II: Carfilzomib/Pomalidomide/LoDEX (Car-Pom-d) in R/R MM 28-day cycles (cycles 1-6) Maintenance (cycles 7+) Study Population (N=79) Relapsed and/or refractory measurable MM Lenalidomide-refractory Carfilzomib* 20/27 mg/m2 (D1-2, 8-9, 15-16) Pomalidomide* 4 mg (D1-21) Dexamethasone* 40 mg weekly (20 mg after cycle 4) Carfilzomib D1-2, 15-16 Pomalidomide unchanged Dexamethasone Treatment continued until PD or unacceptable toxicity All patients received antiviral treatment and aspirin 81 mg or low molecular weight heparin *Dosing based on MTD established in phase 1 Primary endpoint: ORR Secondary endpoints: DOR, TTP, PFS, time to next therapy, OS Shah JJ, et al. Blood. 2013;122:690.
 in R/R MM. 28-day cycles. (cycles 1-6) Maintenance. (cycles 7+) Study Population (N=79) Relapsed and/or refractory measurable MM. Lenalidomide-refractory. Carfilzomib* 20/27 mg/m2 (D1-2, 8-9, 15-16) Pomalidomide* 4 mg (D1-21) Dexamethasone* 40 mg weekly (20 mg after cycle 4) Carfilzomib. D1-2, Pomalidomide. unchanged. Dexamethasone. Treatment continued until PD or unacceptable toxicity. All patients received antiviral treatment and aspirin 81 mg or low molecular weight heparin. *Dosing based on MTD established in phase 1. Primary endpoint: ORR. Secondary endpoints: DOR, TTP, PFS, time to next therapy, OS. Shah JJ, et al. Blood. 2013;122:690.")
66
Car-POM-d in R/R MM: Efficacy
Cytogenetic Risk (by mSMART) Response, % High (n = 18) Intermediate (n = 19) Standard (n = 38) All Pts (N = 79) ORR 78 53 74 70 VGPR 22 26 32 27 PR 56 42 43 Median PFS: 9.7 mos; median DOR: 17.7 months; median OS not reached No significant difference in PFS or OS based on cytogenetics 80% of pts with del(17p) were alive at 12 mos; 58% were progression-free Shah JJ, et al. Blood. 2013;122:690.
 Response, % High (n = 18) Intermediate (n = 19) Standard (n = 38) All Pts (N = 79) ORR VGPR PR Median PFS: 9.7 mos; median DOR: 17.7 months; median OS not reached. No significant difference in PFS or OS based on cytogenetics. 80% of pts with del(17p) were alive at 12 mos; 58% were progression-free. Shah JJ, et al. Blood. 2013;122:690.")
67
Proteosome Inhibitors
Bortezomib Carflizomib Ixazomib Oprozomib Immunomodulating Agents Ub Substrates + Thalidomide Lenalidomide Pomalidomide HDAC inhibitors Romidepsin Vorinostat Panobinostat

69
Phase 2 trial of the histone deacetylase inhibitor romidepsin for the treatment of refractory multiple myeloma Niesvizky et al, Cancer Volume 117, Issue 2, pages , 22 SEP 2010

70
HDAC Inhibitors in RRMM
Description Regimen N ORR (> PR), % HDAC Inhibitors Romidepsin + bortezomib + dex[4] 25 60 Vorinostat + bortezomib[5] 143 17 Bortezomib + panobinostat + dex[6] 55 34.5
, % HDAC Inhibitors. Romidepsin + bortezomib + dex[4] Vorinostat + bortezomib[5] Bortezomib + panobinostat + dex[6]")
71
Vorinostat Bortezomib vs Placebo Bortezomib
Vorinostat: Median PFS: 7·63 months (95% CI 6·87-8·40) Placebo: Median 6·83 months (5·67-7·73) (hazard ratio [HR] 0·77, 95% CI 0·64-0·94;p=0·0100). Dimopoulos et al, Lancet Oncol Oct;14(11):
 Placebo: Median 6·83 months (5·67-7·73) (hazard ratio [HR] 0·77, 95% CI 0·64-0·94;p=0·0100). Dimopoulos et al, Lancet Oncol Oct;14(11):")
72
PANORAMA 1: Phase III Trial of Panobinostat + Bortezomib + Dex
Dexamethasone Study Population (N=768) Relapse or relapsed/refractory MM Bortezomib-refractory excluded 1-3 prior lines of therapy Stratification based on prior lines of therapy, prior bortezomib Placebo Bortezomib Dexamethasone Primary endpoint: PFS Richardson PG, et al. ASCO Abstract 8510.
 Relapse or relapsed/refractory MM. Bortezomib-refractory excluded. 1-3 prior lines of therapy. Stratification based on prior lines of therapy, prior bortezomib. Placebo. Bortezomib. Dexamethasone. Primary endpoint: PFS. Richardson PG, et al. ASCO Abstract")
73
PANORAMA 1: Primary Endpoint Met (PFS)
")
74
Bortezomib Carflizomib Ixazomib Oprozomib Thalidomide Lenalidomide
Melphalan Cyclophosphamide Bendamustin Ub Substrates + Thalidomide Lenalidomide Pomalidomide Romidepsin Vorinostat Panobinostat

75
Autotransplant for Refractory MM
SWOG Trial 8993 PFS OS N = 66 Median = 11 mo N = 66 Median = 19 mo Vesole DH, et al. J Clin Oncol. 1999;17:

76
PBSCT in Relapsed MM TTP median HD Mel 19 months [95% CI 16—25]
PAD Weekly CTX 400 mg/m2 x 21 HD Mel Induction Consolidation TTP median HD Mel 19 months [95% CI 16—25] Cyclophosphamide 11 months [9—12]; hazard ratio 0·36 [95% CI 0·25—0·53]; p<0·0001). Cook G et al,The Lancet Oncology, Volume 15, Issue 8, Pages , July 2014
![PBSCT in Relapsed MM TTP median HD Mel 19 months [95% CI 16—25]](http://slideplayer.com/slide/3900510/13/images/76/PBSCT+in+Relapsed+MM+TTP+median+HD+Mel+19+months+%5B95%25+CI+16%E2%80%9425%5D.jpg "PAD. Weekly CTX 400 mg/m2 x 21. HD Mel. Induction. Consolidation. TTP median. HD Mel 19 months [95% CI 16—25] Cyclophosphamide 11 months [9—12]; hazard ratio 0·36 [95% CI 0·25—0·53]; p<0·0001). Cook G et al,The Lancet Oncology, Volume 15, Issue 8, Pages , July")
77
A Phase 1 Study of Bendamustine and Melphalan Conditioning for Autologous Stem Cell Transplant with Multiple Myeloma.

78
Dose Levels for Bendamustine
On Day 1 Melphalan (100mg/m2) On Day 2 Melphalan (100mg/m2) 1 30 mg/m2 2 60 mg/m2 3 90 mg/m2 4 5 6 125 mg/m2 100 mg/m2
 On Day 2 Melphalan (100mg/m2) mg/m mg/m mg/m mg/m mg/m2.")
79
Elotuzumab Daratumumab SAR650984 Bortezomib Carflizomib Ixazomib
Oprozomib Melphalan Cyclophosphamide Bendamustine Ub Substrates + Filanesib Palbociclib Thalidomide Lenalidomide Pomalidomide Romidepsin Vorinostat Panobinostat

81
The Team and Collaborators
Myelomacenter.org Tomer Mark MD Morton Coleman, MD Roger Pearse, MD Adriana Rossi, MD David Jayabalan Karen Pekle RNP Arthur Perry PA Susan Matthew, PhD Scott Ely, MD/MPH Selina Chen-Kiang, PhD Monica Guzman, PhD Giorgio Inghirami, MD Linda Tegnestam RN Kathleen Pogonowski RN Stanley Goldsmith MD Maureen Lane PhD Paul Christos

Similar presentations



















 Induces High Rates.>")

: Results from the Expansion.>")
 for Newly Diagnosed Multiple Myeloma (MM) Patients: Initial Results of a Multicenter, Open Label.>")


 in Combination with Lenalidomide and Dexamethasone in Relapsed/Refractory Multiple Myeloma.>")