Download presentation
Presentation is loading. Please wait.

1
DIAGNOSIS & TREATMENT PLANNING DR MAYANK SINGH
DEPTT. OF PROSTHODONTICS

2
PATIENT INTERVIEW Establish rapport with the patient Gain insight into the psychological makeup of the patient Explore any physical condition that may effect the treatment Ascertain the patient expectations of treatment

3
STRUCTURE OF INTERVIEW
Dental history - In the dental history it is important to find out why teeth have been lost. If lost by caries If lost by periodontal disease Presence of removal partial Dentures will increase the possibility of further carious activity Every effort must be made to discover and eliminate its cause

4
DIET The patient diet should be evaluated If the patient have sugar containing diet a change must be effected. The problem caused by the sugar is compounded by the wear of removal partial dentures because the prosthesis shield the microorganism from the cleansing and buffering action of patient saliva.

5
HABITS Patient habit should be evaluated to determine whether the effect the prognosis of the treatment. Bruxism and clenching Tongue thrusting

6
EVALUATION OF ORAL HYGIENE
It is critical to the prognosis of the patient treatment Inadequate oral hygiene must be recognized early in the diagnostic procedure so that a preventive dentistry programme can be evaluated.

7
EVALUATION OF CARIES SUSCEPTIBILITY
The presence of large number of restored teeth Sign of recurrent caries Evidence of decalcification

8
ORAL PROPHYLAXIS Supragingival calculus should be removed and oral prophylaxis should be performed The diagnostic cast and definitive intraoral examination will be more accurate if teeth are cleaned

9
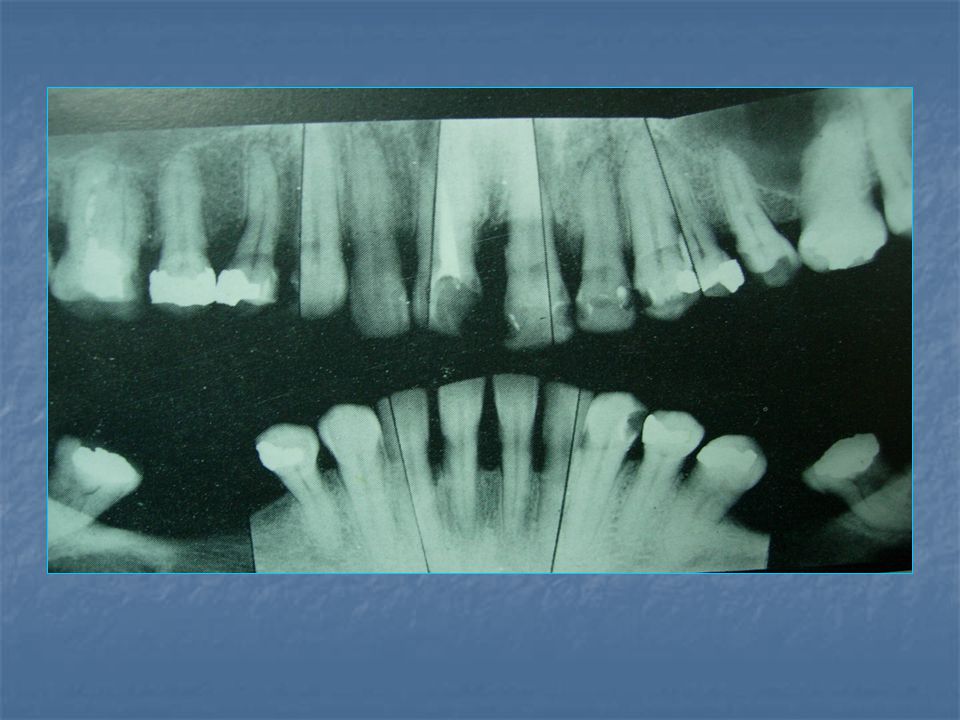
RADIOGRAPH Complete series of periapical and a full mouth radiograph is essential for definitive examination of partially edentulous patient Full mouth radiograph is ideal for screening for pathological condition

10
Periapical radiographs helps in determining
1. Crown root ratio of remaining teeth 2. Status of periodontal ligament space 3. Lamina dura of abutment teeth 4. Quantity of bone on the residual ridge in edentulous area

11
DIAGNOSTIC IMPRESSION AND CAST
A diagnostic procedure for a partially edentulous patient must be considered incomplete unless it includes the evaluation of accurate diagnostic cast.

12
MOUNTED DIAGNOSTIC CAST
Uses includes the following : Extruded teeth, low hanging tuberosities, lack of inter arch space, malposed teeth and defective restoration are readily apparent. They provide a detail analysis of patient occlusion Aid in the education of the patient and in presentation of the treatment planning. They provide a permanent dental record of the patient condition before treatment.

13
Centric jaw relation record
Bone to bone relation Recorded repeatedly and verified Best reference point

14
Methods of determining centric jaw relation
Conventional method Bilateral manipulation of the mandible Alteration of protrusion and retrusion

16
Media for recording centric jaw relation
Wax Impression pastes Plaster of paris Dental stone Acrylic resin Modeling plastic waxes Soft wax Hard wax

19
Definitive oral examination
Evaluation of caries and existing restoration

20
Evaluation of sensitivity to percussion
Tooth movement caused by-prosthesis or occlusion Traumatic occlusion Periapical or pulpal abscesses Acute pulpitis Gingivitis or periodontitis Cracked tooth syndrome

21
Evaluation of mobile teeth
Traumatic occlusion Inflammatory changes in periodontal ligament Loss of alveolar bone support

22
Splinting of abutment teeth
Indications Remaining teeth have reduced support-periodontal disease Teeth with short ,tapered roots Presence of two or three widely spaced retainable teeth

23
Evaluation of periodontium
Pocket depth in excess of 3mm Furcation involvement Deviation from normal color and contour of gingiva Marginal exudate Abutment teeth have less than 2mm of attached gingiva Treatment Root scaling and planning Gingivectomy Periodontal flap procedures Free gingival grafts

24
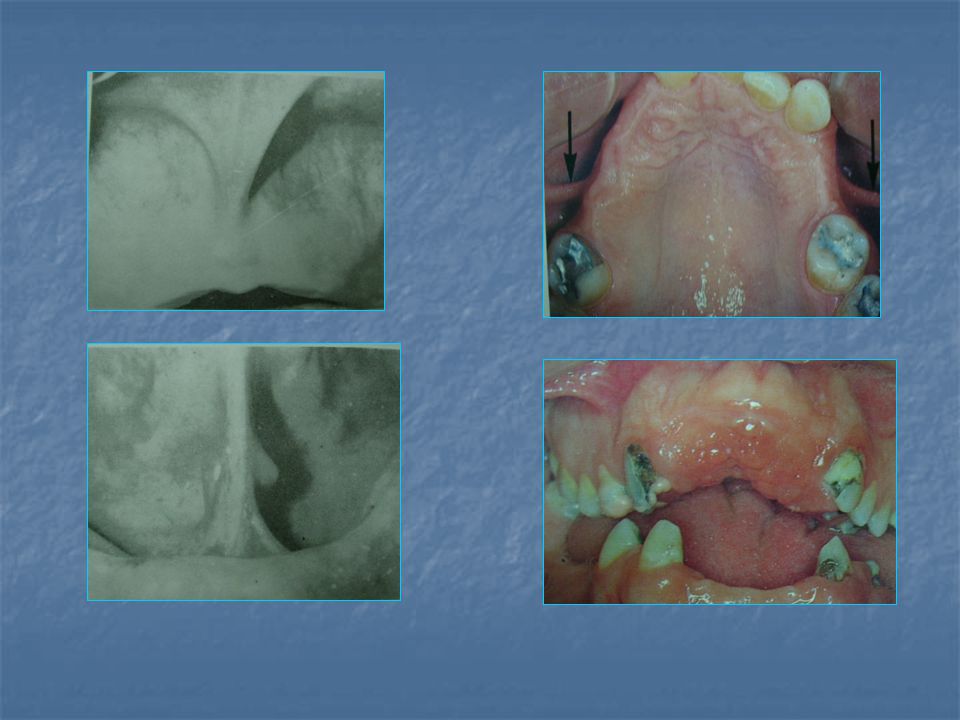
Evaluation of hard tissue abnormalities
Torus palatinus Torus mandibularis Exostosis and undercuts Mandibular tuberosity

25
Evaluation of soft tissue abnormalities
Labial frenum Hypertrophic lingual frenum Unsupported and hypermobile gingiva

27
Evaluation of radiographic survey
Caries Existing restorations Root fragments and other foreign bodies Unerupted third molars Abutment teeth Root length,size ,form Crown/root ratio Lamina dura Periodontal ligament space Bone index areas

29
Evaluation of mounted diagnostic casts
Interarch distance Occlusal plane

30
Occlusal plane Enameloplasty Extracoronal cast metallic restorations
Irregular occlusal plane Enameloplasty Extracoronal cast metallic restorations Extraction

31
Occlusal interferences
Bruxism Excessive wear of teeth Chipping or fracture Increased mobility Tooth migration Injury to TMJ-muscle spasm,pain and joint symptoms

32
Occlusal equilibration
Selective grinding or coronal reshaping of tooth with the intent of equalizing occlusal stress

33
Treat at centric relation or centric occlusion?
Coincidence of centric relation or centric occlusion Absence of posterior tooth contacts Situation in which all posterior tooth contacts are to be restored with cast restorations Only a few posterior contacts Clinical symptoms of occlusal trauma

34
Diagnostic wax-up Provide a guide for tooth preparation
Indicate problems that may be encountered during treatment

35
Development of treatment plan
Phase1 Collection and evaluation of diagnostic data Immediate treatment to control pain and infection Biopsy or referral of patient Development of treatment plan Education and motivation of patient

36
Phase 2 Removal of deep caries followed by temporary restoration
Extripation of inflamed pulp Removal of nonretainable teeth Periodontal treatment Occlusal equilibration

37
Phase 3 Preprosthetic surgical procedures
Definitive endodontic procedures Fixed partial denture construction

38
Phase 4 Removal partial denture
Reinforcement of education and motivation

39
Phase 5 Postinsertion care Periodic recall

40
Q1. The first step in the diagnostic mounting procedure is the mounting of the maxillary cast on a
Fully adjustable articulator Semi-adjustable articulator Denar articulator d)Free plane articulator
Free plane articulator.")
41
Q2. Face bow which requires styli to be placed on selected points on the face is
Whip mix Hanau spring bow Hanau SM d)Hanau H2
Hanau H2.")
42
Q3. Beyron’s point is located _ mm anterior to the posterior margin of the tragus of the ear on a line to the outer canthus of the eye 11 12 13 d)14
14.")
43
Q4. While adjusting the articulator, the following setting are followed for condylar guidance, Bennett guide and incisal table respectively 30, 15, 0 0, 30, 15 15, 30, 0 30, 0, 15

44
Q5. Ramfjord and Ash (1971) have stated that three factors must be controlled in order to succeed in determining centric jaw relation. Which one is not among them? Psychologic stress Pain in temporomandibular joints Muscle memory Systemic illness

45
Q6. In which method of recording jaw relation does the operator place all four fingers of his hand on the lower border of the mandible and thumbs over the symphysis? Bilateral manipulation of the mandible Alternate protrusion and retrusion Both a and b Use of an occlusal splint

46
Q7. Which of the following is not used to record centric jaw relation
Acrylic resin ZoE paste Dental stone All of the above are used

47
Q8. While using metal impregnated wax, water bath temperature kept is
40°C 43°C 45°C 37°C

48
Thank you

49
ANSWERS 1. B 2. D 3. C 4. A 5. D 6. B 7. A 8. B

Similar presentations






>")






>")

. All rights reserved. Removable Prosthodontics Chapter 52 Copyright 2003, Elsevier Science (USA). All rights reserved.>")






