Download presentation
Presentation is loading. Please wait.

1
Seyed Mojtaba Aghili, M.D. Imam Khomeini General Hospital
Vertigo Seyed Mojtaba Aghili, M.D. Imam Khomeini General Hospital

3
Definition Dizziness may mean vertigo, syncope, presyncope, weakness, giddiness, anxiety, or a disturbance in mentation to various patients. Vertigo is the perception of movement (rotational or otherwise) where no movement exists
 where no movement exists.")
4
Definition Syncope is a transient loss of consciousness that is accompanied by loss of postural tone with spontaneous recovery. Near-syncope is light-headedness with concern for an impending loss of consciousness

5
Pathophysiology visual, vestibular, and proprioceptive systems
Vertigo arises from a mismatch of information from two or more of the involved senses

6
PH/E The most striking clinical sign associated with vertigo is nystagmus. Rhythmic movement of the eyes that has both a fast and a slow component, with direction named by its fast component.

7
The fast component of nystagmus is caused by the cortex
The nystagmus of vestibular injury or dysfunction is provoked when the affected side is in the dependent position, and the characteristic pattern is vertical and rotational or horizontal.

8
Vertical nystagmus by itself (and not associated with a rotational component) usually indicates a brainstem abnormality. an atypical pattern of nystagmus in the absence of other signs of CNS disease does not necessarily indicate central pathology

9
Clinical Features "peripheral" or "central"
Peripheral vertigo is caused by disorders affecting the vestibular apparatus and the eighth cranial nerve Central vertigo is caused by disorders affecting central structures, such as the brainstem and the cerebellum

10
severity and even accentuation with certain head positions, while suggestive, does not uniformly distinguish underlying pathology.

11
Etiologic Classification of Vertigo
Vestibular/otologic Benign paroxysmal positional vertigo Traumatic: following head injury Infection: labyrinthitis, vestibular neuronitis, Ramsay Hunt syndrome Syndrome Ménière syndrome Neoplastic Vascular Otosclerosis Paget disease Toxic or drug-induced: aminoglycosides

12
Neurologic Vertebrobasilar insufficiency Lateral Wallenberg syndrome
Anterior inferior cerebellar artery syndrome Neoplastic: cerebellopontine angle tumors Cerebellar disorders: hemorrhage, degeneration Basal ganglion diseases Multiple sclerosis Infections: neurosyphilis, tuberculosis Epilepsy Migraine headaches Cerebrovascular disease

13
General Hematologic: anemia, polycythemia, hyperviscosity syndrome
Toxic: alcohol Chronic renal failure Metabolic: thyroid disease, hypoglycemia

14
Peripheral vs Central Vertigo
Peripheral Central Onset Sudden Sudden or slow Severity of vertigo Intense spinning Ill defined, less intense Pattern Paroxysmal, intermittent Constant Aggravated by position/movement Yes Variable Associated nausea/diaphoresis Frequent Variable Nystagmus Rotatory-vertical, horizontal Vertical Fatigue of symptoms/signs Yes No Hearing loss/tinnitus May occur Does not occur Abnormal tympanic membrane May occur Does not occur Central nervous system symptoms/signs Absent Usually present

15
Peripheral vs Central Peripheral vertigo: distressing symptoms, seldom life-threatening. Central vertigo: less distressing symptoms, slower onset than those due to peripheral vertigo

16
Diagnosis The key: an unprompted description of the patient's "dizziness." Avoid leading questions because they may bias the patient's responses

18
Peripheral vs Central Peripheral vertigo: intense and associated with nausea, vomiting, diaphoresis, tinnitus, hearing loss, and photophobia

19
Peripheral vs Central Central vertigo: associated with neurologic symptoms and signs such as diplopia, dysarthria, and bilateral visual abnormalities. An associated headache or history of headache: migraine, stroke, transient ischemic attack (TIA), or a space-occupying lesion.
, or a space-occupying lesion.")
20
? Clinician should not be reassured that a central cause is not present when symptoms appear more consistent with benign peripheral etiology

21
Central Vertigo should be evaluated for central vertigo.
Older patients, those with hypertension or cardiovascular disease, those with other risk factors for stroke, or those taking warfarin should be evaluated for central vertigo.

22
Temporal Patterns Seen in Vertigo
Conditions Seconds Benign paroxysmal positional vertigo, postural hypotension Minutes Transient ischemic attacks Hours Ménière disease Days Viral labyrinthitis Constant Nonspecific dizziness

23
Physical Examination Ear, Neurologic, and Vestibular examinations
Insufflation of air by use of a pneumatic otoscope that precipitates a burst of vertigo with nystagmus is diagnostic of an inner ear fistula

24
Central vertigo Central vertigo:
check for an absent corneal reflex, facial paresis, difficulty swallowing, dysphonia, and depressed gag reflex. Limb and truncal ataxia, and test the vestibulospinal system and cerebellum through tandem gait and Romberg testing. Proprioception and vibration

25
BPPV: Dx aided by the Dix-Hallpike position test.
This test should not be performed on patients with carotid bruits, cerebrovascular disease, risk factors or concern for vertebrobasilar insufficiency (VBI), spinal injury, or cervical spondylosis
, spinal injury, or cervical spondylosis.")
26
Dix-Hallpike The patient should be cautioned that the test could provoke vertigo. Pretreatment with 50 milligrams dimenhydrinate IM or IV may make the test more tolerable but will not obliterate nystagmus

27
Dix-Hallpike A positive test is indicated by rotatory nystagmus following a latency of no more than 30 seconds; the nystagmus exhibits rapid eye torsions toward the affected ear and lasts for 10 to 40 seconds

28
Dix-Hallpike The side exhibiting the positive test is the side of the lesion. The test is about 50% to 80% sensitive for BPPV.

29
Benign paroxysmal positional vertigo is the most common cause of vertigo
visual, vestibular, and proprioceptive systems, any disease that interrupts the integration of these three systems

30
slow movement of the eyes toward the side of the stimulus, regardless of the direction of deviation of the eyes. The cerebral cortex then corrects for these eye movements and rapidly brings the eyes back to the midline

31
direction of nystagmus is denoted by the direction of the fast "cortical" component.
Nystagmus caused by vestibular disease: unidirectional and horizontorotary. If the nystagmus is vertical, a central lesion (either brainstem or cerebral)
")
32
Differential Considerations
Patients use the term dizzy to describe a variety of experiences,including sensations of morion, weakness, fainting, lightheadedness, unsteadiness, and depression.

33
differential diagnosis of dizzy
dysrhythmias, anemia, myocardial infarction, viral illness, depression sepsis, hypovolemia, drug side effects, and PTE,

34
cerebellar hemorrhage: immediate therapeutic intervention
Acute suppurative labyrinthitis is the only cause of peripheral vertigo that requires urgent intervention.

37
History Does true vertigo exist?
The labyrinth has no effect on the level of consciousness, patient should not have an associated change in mentation or syncope. A sensation of imbalance often accompanied vertigo, but true instabiliry, disequilibrium or ataxia makes a higher likelihood of a central process.

38
time of onset and the duration of vertigo?
Episodic vertigo that is severe, lasts several hours, and has symptom-free intervals between episodes suggests a peripheral labyrinth disorder auditory symptoms?

39
Are there association neurologic symptoms?
recent head or neck trauma? isolated vertigo can be the only initial symptom of cerebellar and other posterior circulation bleeds, transient ischemic attacks (TIAs), and infarction.
, and infarction.")
40
Imaging and admission Older age, male sex, hypertension,
coronary artery disease, diabetes mellitus, and atrial fibrillation, frequent episodes lasting only minutes or prolonged episodes of a day or more

41
Past Medical History aminoglycosides, anticonvulsants, alcohols, quinine, quinidine, and minocycline, caffeine and nicotine

42
Physical Examination Pulses and blood pressure in both arms.
R/o subclavian steal syndrome, which also can cause vertebrobasilar artery insufficiency

43
Physical Examination Carotid or vertebral artery bruits?
impacted cerumen or a foreign object in the ear canal? Examination of the eyes?

44
Internuclear ophthalmoplegia
eyes are in a normal position on straight-ahead gaze, but on eye movement the adducting eye (cranial nerve III) is weak or shows no movement while the abducting eye (cranial nerve VI) moves normally, although ofren displaying a coarse nystagmus.
 is weak or shows no movement while the abducting eye (cranial nerve VI) moves normally, although ofren displaying a coarse nystagmus.")
45
Internuclear ophthalmoplegia
interruption of the medial longitudinal fasciculus on the side of the third cranial nerve weakness: brainstem pathology and virtually pathognomonic of multiple sclerosis.

46
Positional testing Hallpike maneuver, the patient is moved quickly from an upright seated position to a supine position, and the head is turned to one side and extended (to a headdown posture) approximately 30' from the horizontal plane off the end of the stretcher. repeated with the head turned to the other side, indicates vestibular pathology on that same side.
 approximately 30 from the horizontal plane off the end of the stretcher. repeated with the head turned to the other side, indicates vestibular pathology on that same side.")
47
Positional testing

48
Nystagmus?

49
Neurologic examination
cranial nerve deficits suggests a space-occupying lesion in the brainstem or cerebellopontine angle corneal reflex, hearing loss, evidence of cerebellar dysfunction? In supranuclear facial paralysis, the forehead is spared because these muscles receive bilateral cortical innervation.

50
Neurologic examination
Dysmetria is the inability ro arrest a muscular movement at the desired point. Dysmetria should be assessed using finger-to-finger/finger-to-nose pointing dysdiadochokinesia(an inability to perform coordinated muscular movement smoothly) is assessed with rapid alternating movements.
 is assessed with rapid alternating movements.")
51
Neurologic examination
Any marked abnormality (e.g., consistent falling or a grossly abnormal gait) should suggest a central lesion, especially in a patient whose vertiginous symptoms have subsided.
 should suggest a central lesion, especially in a patient whose vertiginous symptoms have subsided.")
52
Ancillary testing A finger-stick blood glucose
Blood counts and blood chemistries An electrocardiogram

53
Radiologic imaging cerebellar hemorrhage, cerebellar infarction, or other central lesions: emergent computed tomography (CT) or magnetic resonance imaging (MRI) of the brain MRI, has become the diagnostic modality of choice when cerebellar processes other than acute hemorrhage
 or magnetic resonance imaging (MRI) of the brain. MRI, has become the diagnostic modality of choice when cerebellar processes other than acute hemorrhage.")
54
Radiologic imaging many studies strongly support the use of imaging in patients of advanced age or at risk for cerebrovascular disease.

55
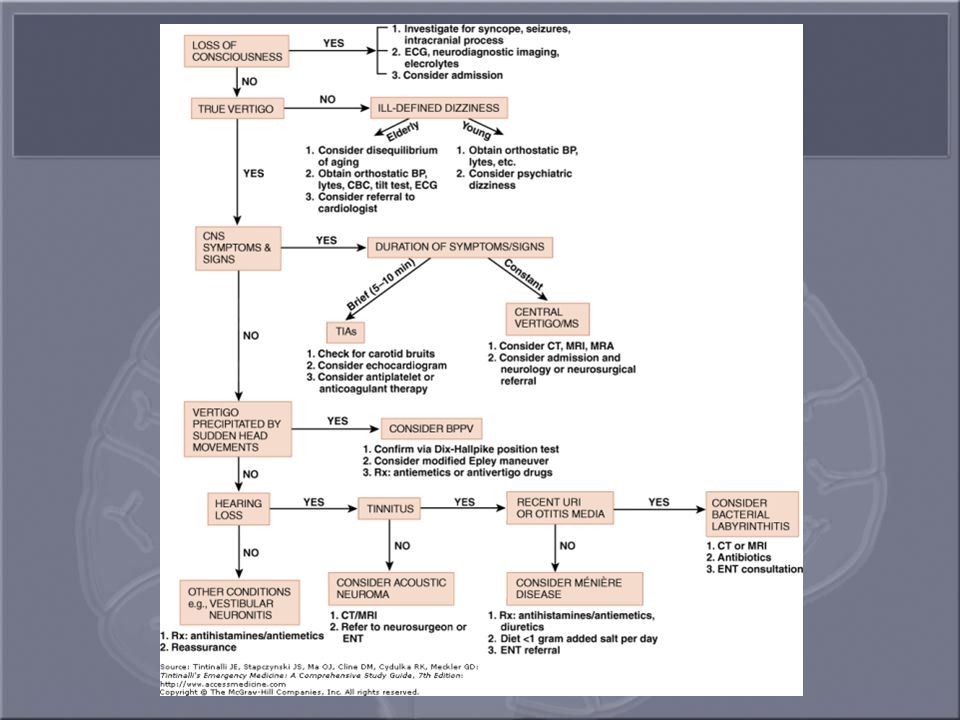
Diagnostic Algorithm

56
MANAGEMENT Any suggestion of cerebellar hemorrhage should warrant immediate imaging with CT or MRI and neurosurgery consultations. VBI should be considered in any patient of advanced age or at high risk of cerebrovascular disease with isolated, new-onset vertigo without an obvious cause.

57
Because of the possibility of progression of new-onset VBI in the first 24 to 72 hours, hospital or observation unit admission and considering early magnetic resonance angiography.

58
Changing or rapidly progressive symptoms should raise awareness of impending posterior circulation occlusion. If CT or MRI excludes hemorrhage as the source of the patient's symptoms, an immediate neurologic consultation, emergency angiography, and possibly anticoagulation are indicated.

59
Acute bacterial labyrinthitis requires admission, intravenous antibiotics, and occasionally surgical drainage and debridement.

60
Meniere's disease have been treated successfully by vasodilation and diuretic therapy, diets low in sodium and caffeine and cessation of smoking Chemical ablation of vestibular function with gentamicin and streptomycin is an option in severe Meniere's disease

61
The treatment of acute attacks of vertigo caused by peripheral disorders is symptomatic.
Intravenous diazepam in 2- to 5-mg doses is extremely effective in stopping vertigo. Outpatient treatment with diazepam can be continued at doses of 5 to 10 mg three times daily.

62
Anticholinergic drugs or antihistamines with anticholinergic activity are extremely useful in treating vertigo. Meclizine hydrochloride (Antivert) is usually prescribed as 25 mg every 8 hours Diphenhydramine hydrochloride (Benadryl), 25 to 50 mg every 6 to 8 hours, and dimenhydrinate.
 is usually prescribed as 25 mg every 8 hours. Diphenhydramine hydrochloride (Benadryl), 25 to 50 mg every 6 to 8 hours, and dimenhydrinate.")
63
Promethazine hydrochloride (Phenergan), 25 mg orally or rectally every 6 to 8 hours, is effective because of its strong antiemetic and mild anticholinergic properties; it also can be used intravenously in doses of 12.5 to 25 mg
, 25 mg orally or rectally every 6 to 8 hours, is effective because of its strong antiemetic and mild anticholinergic properties; it also can be used intravenously in doses of 12.5 to 25 mg")
64
Avoidance of stimulants (e.g., caffeine, pseudoephedrine, Nicotine)
canalith repositioning procedures, such as the Epley and Semont maneuvers in BPPV.

65
The Epley maneuver involves sequential movement of the head into four positions, staying in each position for approximately 30 seconds. One of the most useful tools the physician has is patient reassurance.

69
Management algorithm for vertigo

70
Epley

71
DISPOSITION Documented or suggested cerebellar hemorrhage or infarction, VBI, and acute bacterial labyrinthitis require workup and hospitalization. In patients older than age 55 years, particularly patients with vascular disease, admission for observation and imaging of cerebral vasculature is often warranted

72
Some patients may have such severe symptoms (e. g
Some patients may have such severe symptoms (e.g., vomiting, inability to walk) despite a trial of medication that they require admission for intravenous hydration and observation. All discharged patients should receive primary care; neurology; or a follow-up consult with an ear, nose, and throat specialist.
 despite a trial of medication that they require admission for intravenous hydration and observation. All discharged patients should receive primary care; neurology; or a follow-up consult with an ear, nose, and throat specialist.")
Similar presentations














 Is it a stroke? (2) What part of the brain is affected? (3) What caused this stroke? Is it a haemorrhage or an infarct? Can.>")











