Download presentation
Presentation is loading. Please wait.

1
OB/GYN Emergencies July 2010 Emory Family Medicine

2
Topics Postpartum hemorrhage Shoulder dystocia
Third trimester bleeding Eclampsia Ectopic pregnancy Miscarriage PID Ovarian pathology

3
Learning Objectives

4
OB Emergencies Postpartum hemorrhage Shoulder dystocia
Third trimester bleeding Eclampsia

5
Postpartum Hemorrhage
Defined as >500 cc blood loss. Risk factors Overdistended uterus: polyhydramnios, twins pitocin stimulated labor general anesthesia amnionitis retained placental fragments

6
Postpartum Hemorrhage Treatment
Sweep uterus to remove retained parts. Massage uterus. Pitocin units in 1 liter, bolus. Methergine 0.2 mg IM, may repeat. Consider not using in pre-eclamptic. Hemabate (prost. F2alpha) 0.25 mg IM.
 0.25 mg IM.")
7
Postpartum Hemorrhage Treatment
Inspect for other causes of PPH - cervical/vaginal laceration, episiotomy. Consider pelvic hematoma - may not initially be visible. Treat blood loss like any other condition - fluids, blood products. Get help!!!

8
OB Emergencies Postpartum hemorrhage Shoulder dystocia
Third trimester bleeding Eclampsia

9
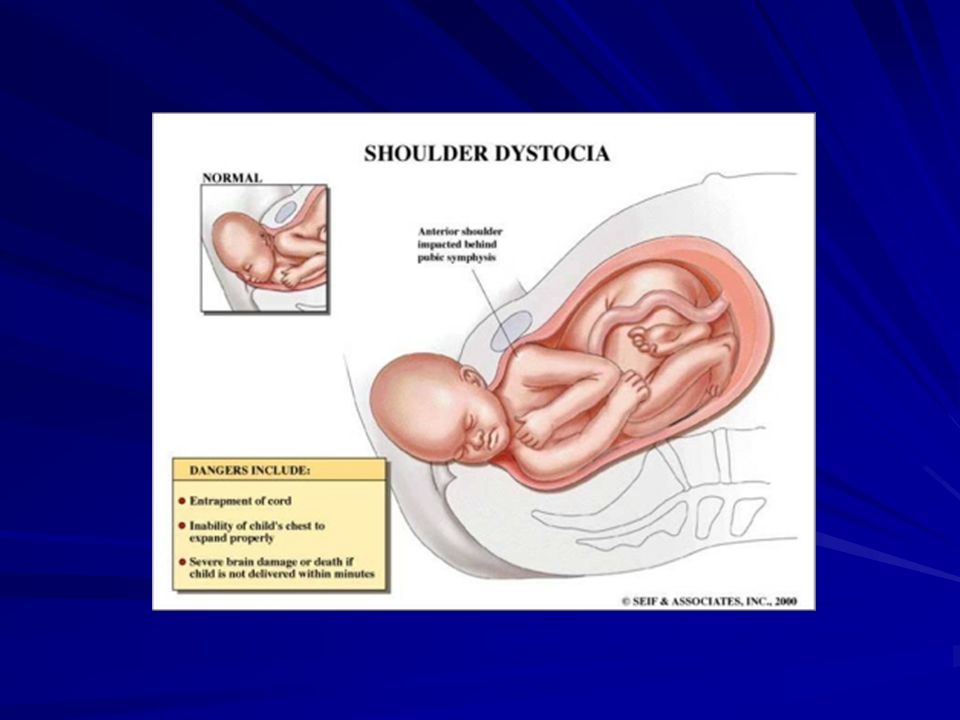
Shoulder Dystocia Defined as a vaginal delivery in which the anterior shoulder of the baby is not readily deliverable. % all deliveries - BE READY! Risk Factors - ???

10
Shoulder Dystocia Risk Factors Fetal macrosomia Maternal obesity
Previous infant > 4000gm Diabetes Prolonged gestation

13
Shoulder Dystocia Fetal macrosomia 50% infants < 4000gm.
Fetal wt > 4000gm ---> risk increased x11. Fetal wt > 4500gm ---> risk increased x22. EFW off by 3 lbs (!!!) in 6% patients in one study. Ultrasound error is easily +/- 10%.
 in 6% patients in one study. Ultrasound error is easily +/- 10%.")
14
Shoulder Dystocia Treatment
ALSO Course mnemonic - HELPERR Go get Dr. McRoberts !!! Get Help. Suprapubic pressure - NOT FUNDAL. Generous episiotomy. Rotate posterior shoulder - Wood’s screw maneuver. May then deliver posterior arm first.

15
Shoulder Dystocia Treatment
Rotate anterior shoulder obliquely. Fracture clavicle. Symphysiotomy Dr. Patil has done this at least 3 times. Zavenelli maneuver I precepted this maneuver while watching ER.

16
Helperr H - Help E - Episiotomy L - Legs into McRoberts
P - Pressure, suprapubic E - Enter for rotational maneuvers R - Remove posterior arm R - Roll patient onto hands and knees

17
OB Emergencies Postpartum hemorrhage Shoulder dystocia
Third trimester bleeding Eclampsia

18
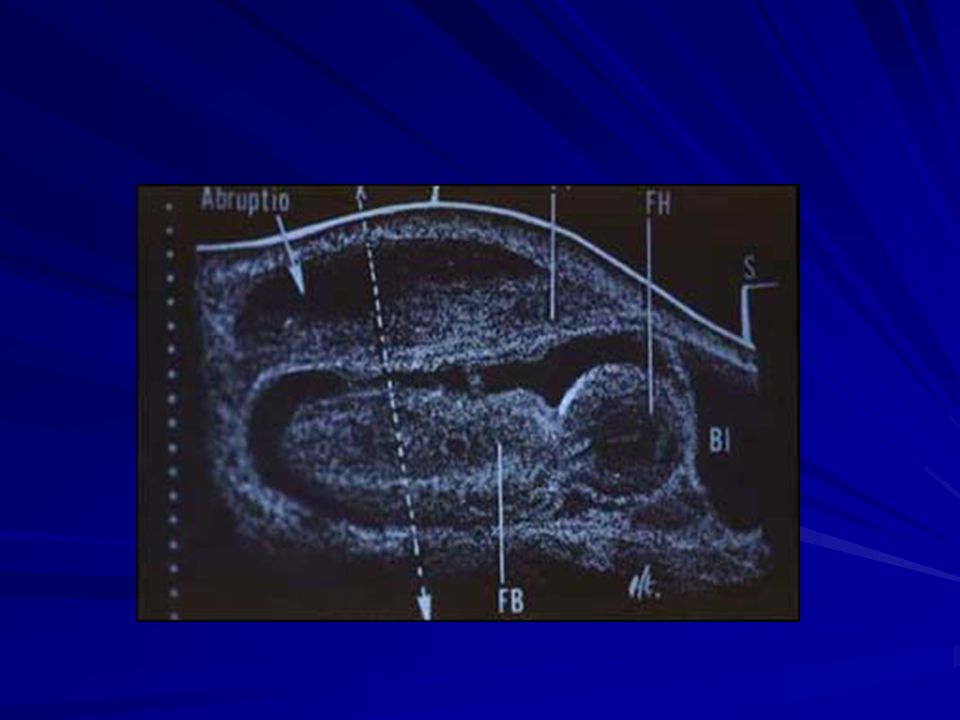
Placental Abruption Painful third trimester bleeding.
1:120 pregnancies, approx. 1%. Recurrence rate of 10%. Port wine stained amniotic fluid. Mark line at top of fundus at presentation and follow fundal height serially.

19
Placental Abruption

20
Placental Abruption

21
Placental Abruption

24
Placental Abruption Risk factors
Increased blood pressure Trauma Drug use - cocaine Smoking/poor nutrition Chorioamnionitis Twins/polyhydramnios

25
Placental Abruption Treatment
Trauma - 2 large bore IVs, labs, fluids, can take a red top tube for spontaneous clot - may check CBC/coags and fibrinogen serially. Consider ultrasound - must have cc blood to be visible. May be able to see a retroplacental lucency

26
Placental Abruption Treatment
If term, deliver. Consider controlled induction if patients are stable. If preterm, weigh risks of continued pregnancy against risks of complications from preterm delivery. Need NICU backup. Give steroids and vitamin K as usual.

27
Placental Abruption Treatment
Do not use beta mimetics to tocolyze. They may cause maternal hypotension - badness. They may also cause maternal tachycardia which may mask hypotension. Use magnesium to tocolyze. Get Help!!!

28
OB Emergencies Postpartum hemorrhage Shoulder dystocia
Third trimester bleeding Eclampsia

29
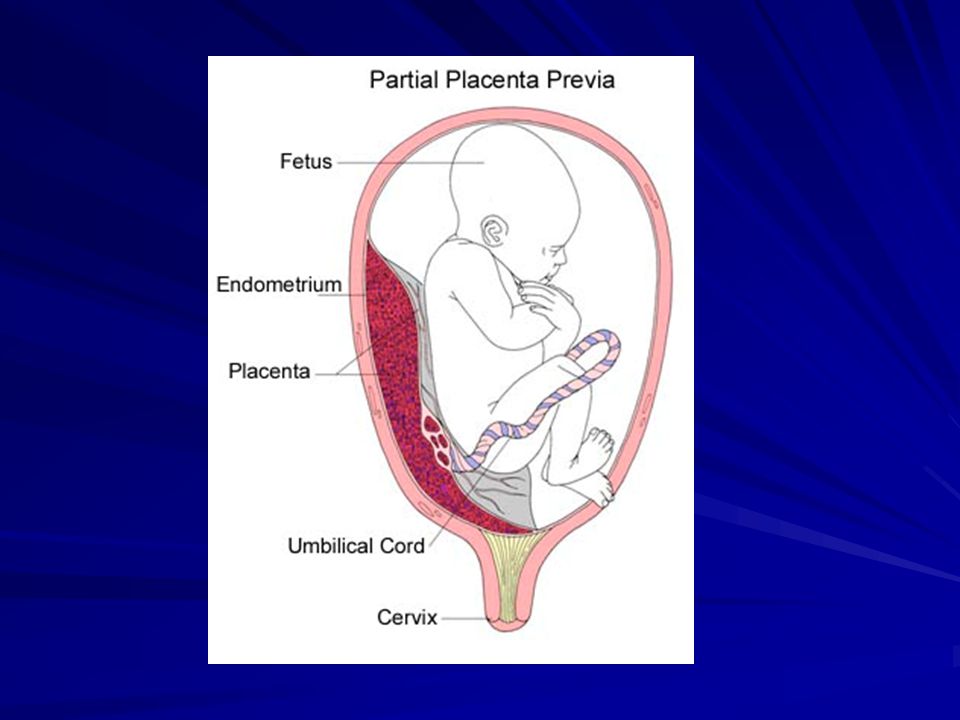
Placenta Previa Painless third trimester vaginal bleeding
1: :250 pregnancies average 1:50 grand multiparas,1:1500 nulliparas Undiagnosed third trimester bleeding, consider a double set-up in the OR. Biggest risk factor is prior C-section, which confers a 1% risk.

30
Placenta previa Types Total - needs operative delivery.
Partial and Marginal - may consider a vaginal delivery as the baby’s head may tamponade the placenta during descent Consider fetal hemorrhage in addition to maternal hemorrhage.

34
Special Labs KB or Kleihauer-Betke test. Checks for amount of fetal cells in maternal circulation. Apt test. Determines if blood is fetal or maternal. Rh status. Mom needs rhogam if she is Rh negative. 1 amp = 300 micrograms which covers 30cc fetal hemorrhage.

35
Placenta Previa Treatment
If baby mature by amniocentesis (L/S ratio, PG - phosphotidylglycerol/ amniostat) or >36 wk EGA, then deliver. If baby immature and maternal condition stable, give steroids/vitamin K. May tocolyze prn until mature or condition unstable. Get help!!!
 or >36 wk EGA, then deliver. If baby immature and maternal condition stable, give steroids/vitamin K. May tocolyze prn until mature or condition unstable. Get help!!!")
36
Placental abnormalities
Placenta accreta Firm attachment to myometrium. 4% of previas have this. Placenta increta Invasion of myometrium. Placenta percreta Invades through myometrium. Placenta concreta - placenta hard as rock and well set.

37
Placenta accreta

38
Placenta Accreta

39
Vascular Abnormalities
Vasa Previa - fetal vessel running in front of internal os. These may rupture causing painless third trimester vaginal bleeding. 1:3000 deliveries. The Apt test may be used to differentiate fetal from maternal bleeding in this case.

40
Vasa Previa

41
Vasa Previa

42
OB Emergencies Postpartum hemorrhage Shoulder dystocia
Third trimester bleeding Eclampsia

43
Eclampsia Seizure in pregnancy at or near term usually associated with preeclampsia or hypertension. May occur up to 48 hours after delivery. 70% at delivery, 30% postpartum. Risk factors - primigravida, non-white, age>35. 1: :3500 (it happens, we’re not sure when).
.")
44
Eclampsia Common symptoms
Headache - 82% Visual changes - 44% Epigastric/RUQ pain - 19%

45
Eclampsia Treatment Deliver - get help, not HELLP.
Bite stick, left lateral decubitus, prevent falls, suction PRN, O2. Magnesium 4-6 gm over minutes. May bolus an additional 2gm prn a second seizure. Run at 2gm/hr, check levels.

46
Eclampsia Treatment Diazepam - may cause apnea at high enough doses, may lead to fetal compromise. Dilantin??? Hydralazine to control hypertension. Consider labs to assess HELLP, DIC.

47
Healthy babies do exist!!!

48
GYN Emergencies Ectopic pregnancy Miscarriage PID Ovarian pathology

49
Ectopic Pregnancy 1:100 pregnancies on average. 25% recurrence rate.
Future fertility rate = 50%. Remember Rh status. Risk factors ???

50
Ectopic Pregnancy Risk Factors
Prior ectopic. Prior abdominal surgery, especially BTL. This confers a 50% ectopic rate. Endometriosis PID - 50% ectopics have this hx. Relative risk (RR) increased x 7. IUD (?), DES, prior abortion. First Ab increases RR x 1.3, 2nd x 2.6.
 increased x 7. IUD ( ), DES, prior abortion. First Ab increases RR x 1.3, 2nd x 2.6.")
51
Ectopic Pregnancy Diagnosis
(+) hCG, unilateral abdominal/pelvic pain, vaginal bleeding. Pain - 94% Missed LMP - 89% Vaginal bleeding - 80% Palpable mass in only 50% - don’t squeeze too hard!!!
 hCG, unilateral abdominal/pelvic pain, vaginal bleeding. Pain - 94% Missed LMP - 89% Vaginal bleeding - 80% Palpable mass in only 50% - don’t squeeze too hard!!!")
52
Ectopic Pregnancy Most present after rupture (by 10 weeks EGA)
Unruptured ectopics - 65% have a (+) culdocentesis Ruptured ectopics - 85% have a (+) culdocentesis
 culdocentesis. Ruptured ectopics - 85% have a (+) culdocentesis.")
53
Discriminatory Zone This is the value of the hCG above which an intrauterine sac should be seen. Transabdominal U/S hCG Transvaginal (TV) U/S (or less) 50% of IUPs visible at an hCG of 1500 By TV U/S, fetal cardiac activity at weeks EGA.
 U/S (or less) 50% of IUPs visible at an hCG of By TV U/S, fetal cardiac activity at weeks EGA.")
54
Ectopic Pregnancy Treatment
Get help!!! Trauma - 2 large bore IV, fluids, CBC/ coags, ABO/Rh, type and screen/cross. With “Chronic Ectopic” - consider methotrexate If not sure in equivocal patient and U/S not helpful, observe and check “doubling” of hCG.

55
Heterotopic pregnancy
Defined ??? Classically 1:30000 Now with advent of ovulation induction (clomid, pergonal, etc...) this risk is much higher, 1:900 is the lowest number I’ve seen, up to 1:7000.
 this risk is much higher, 1:900 is the lowest number I’ve seen, up to 1:7000.")
56
Spontaneous Abortion Threatened Ab - uterine cramps with vaginal bleeding w/o cervical dilation. Historically, 50% abort, 50% don’t. Can’t predict who will abort, therefore, strict bedrest not necessary. Demonstration of fetal cardiac activity decreases risk of SAb to 5% or less

57
Spontaneous Abortion Inevitable Ab - cramps, vaginal bleeding, cervical dilation (not just parous cervix). May note tissue in the os. May be accompanied by a gush of fluid. Rare case reports of salvaged pregnancies.

58
Spontaneous Abortion Incomplete Ab - Vaginal bleeding, cramps, os dilated with tissue present. Tissue may have already partially passed in patient with continued bleeding. May remove tissue with ring forceps. Suction curettage in unstable patient after demonstrating no fetal cardiac activity or Mom’s life in danger.

59
Spontaneous Abortion Missed Ab - Dead fetus for several weeks without passage of tissue. I see this most commonly in women without doptones at weeks. Ultrasound then shows lack of fetal cardiac activity. Most pass spontaneously. May need suction curettage.

60
Pelvic Inflammatory Disease
Clinically defined Cervical motion tenderness, abdominal pain, adnexal pain (possibly mass - TOA). Fever Fullness in the posterior fornix - pus on culdocentesis, fluid in pouch of Douglas. Elevated WBC, elevated ESR. Positive gram stain/culture
. Fever. Fullness in the posterior fornix - pus on culdocentesis, fluid in pouch of Douglas. Elevated WBC, elevated ESR. Positive gram stain/culture.")
61
Pelvic Inflammatory Disease DDx
Acute appendicitis, especially ruptured. Diverticulitis, especially abscess. Septic abortion Adnexal torsion Others (Crohn’s exacerbation with fistula formation.)
")
62
Pelvic Inflammatory Disease Treatment
Tubo-ovarian abscess - consult GYN, take to surgery and drain. May consider IV antibiotics in small abscess with stable patient. Treat aggressively as this can predispose to future ectopics and infertility. I was taught to hospitalize in first episode.

63
Ovarian Pathology Painful cyst, especially hemorrhagic or ruptured.
Torsion. Recent case of torsed dermoid cyst requiring surgery in a pregnant woman. Endometrioma - torsed or ruptured. Adhesions.

Similar presentations























>")