Download presentation
Presentation is loading. Please wait.

1
Ischemic Heart Disease William J Hunter MD

2
Types of Heart Disease Acquired Heart Disease Acquired Heart Disease Congenital Heart Disease Congenital Heart Disease

3
Acquired Heart Disease Ischemic Heart Disease Ischemic Heart Disease Hypertensive Heart Disease Hypertensive Heart Disease Valvular Heart Disease Valvular Heart Disease Myocardial Heart Disease Myocardial Heart Disease

4
Ischemic Heart Disease Supply of oxygen in the coronary arterial blood is inadequate to provide for the oxygen demands of the heart. Supply of oxygen in the coronary arterial blood is inadequate to provide for the oxygen demands of the heart.

5
Epidemiology of ischemic heart disease 500,000 die 500,000 die Overall rate has fallen since 1980 Overall rate has fallen since 1980 Prevention - working on risk factors: smoking, hypertension, cholesterol, better diabetic control, aspirin prophylaxis Prevention - working on risk factors: smoking, hypertension, cholesterol, better diabetic control, aspirin prophylaxis Therapeutic advances- new medications, coronary care units, thrombolysis, angioplasty, stents and coronary bypass surgery Therapeutic advances- new medications, coronary care units, thrombolysis, angioplasty, stents and coronary bypass surgery

6
Results of Ischemic HD Angina Pectoris - ASVD Angina Pectoris - ASVD Stable angina Stable angina Prinzmetal’s angina - spasm Prinzmetal’s angina - spasm Preinfarction (unstable) angina - MI Preinfarction (unstable) angina - MI Myocardial Infarct- myocardial necrosis Myocardial Infarct- myocardial necrosis Sudden cardiac death Sudden cardiac death Chronic ischemic HD with heart failure- ‘focal fibrosis’ or presbycardia Chronic ischemic HD with heart failure- ‘focal fibrosis’ or presbycardia
 angina - MI Preinfarction (unstable) angina - MI Myocardial Infarct- myocardial necrosis Myocardial Infarct- myocardial necrosis Sudden cardiac death Sudden cardiac death Chronic ischemic HD with heart failure- ‘focal fibrosis’ or presbycardia Chronic ischemic HD with heart failure- ‘focal fibrosis’ or presbycardia")
7
Acute Coronary Syndromes The new ‘in’ word- TV ads The new ‘in’ word- TV ads A spectrum -from unstable angina to acute myocardial infarct A spectrum -from unstable angina to acute myocardial infarct Atherosclerotic plaque disruption and associated platelet-fibrin thrombus formation Atherosclerotic plaque disruption and associated platelet-fibrin thrombus formation Sudden death Sudden death

8
Acute coronary Syndrome

9
Etiology of Ischemic HD 95-98% Atherosclerotic Narrowing with plaques 95-98% Atherosclerotic Narrowing with plaques Coronary embolism (rare) Coronary embolism (rare) Dissecting aneurysm (rare) Dissecting aneurysm (rare) Arteritis (polyarteritis, rheumatoid, Kawasaki Disease) (rare) Arteritis (polyarteritis, rheumatoid, Kawasaki Disease) (rare) Syphilis (rare) Syphilis (rare) Cocaine abuse Cocaine abuse
 Coronary embolism (rare) Dissecting aneurysm (rare) Dissecting aneurysm (rare) Arteritis (polyarteritis, rheumatoid, Kawasaki Disease) (rare) Arteritis (polyarteritis, rheumatoid, Kawasaki Disease) (rare) Syphilis (rare) Syphilis (rare) Cocaine abuse Cocaine abuse")
10
Coronary Atherosclerosis 90% have at least one 75% occlusion- the key is acute change of the plaque 90% have at least one 75% occlusion- the key is acute change of the plaque Hemorrhage into the atheroma Hemorrhage into the atheroma Rupture of the plaque with thrombosis Rupture of the plaque with thrombosis Erosion or ulceration of the plaque with thrombosis Erosion or ulceration of the plaque with thrombosis Most have two arteries involved Most have two arteries involved Most blocks are in the epicardial arteries Most blocks are in the epicardial arteries

11
Atherosclerotic plaque

12
Hemorrhage into plaque compromises lumen

14
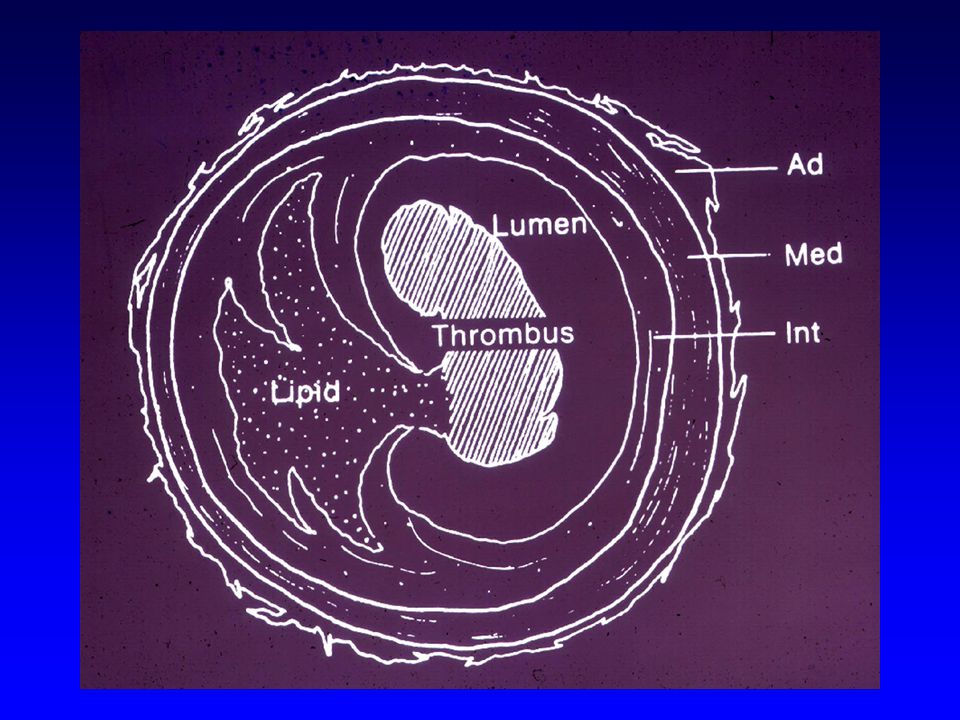
Cut section of a coronary artery with complete occlusion

15
Histologic section with recent thrombosis

16
Rupture of Plaque

17
Progression of Myocardial necrosis after occlusion

18
Myocardial Infarct Most have Most have >75% occlusion of coronary by plaque >75% occlusion of coronary by plaque multi-vessel disease multi-vessel disease 80% have recent thrombus 80% have recent thrombus LAD most commonly involved LAD most commonly involved

19
Typical MI Most have multivessel disease Most have multivessel disease Ulcerative stenotic plaque or hemorrhage into the plaque Ulcerative stenotic plaque or hemorrhage into the plaque Platelets aggregate Platelets aggregate Tissue thromboplastin released Tissue thromboplastin released Vasoactive amines released Vasoactive amines released Thrombosis and spasm occur Thrombosis and spasm occur Ischemic necrosis Ischemic necrosis

20
Arteries involved LAD (40 - 50%) Anterior wall, apex, Anterior 2/3 septum LAD (40 - 50%) Anterior wall, apex, Anterior 2/3 septum RCA (30- 40%) Post wall, post 1/3 septum RCA (30- 40%) Post wall, post 1/3 septum LCA (15- 20%) Lateral wall LCA (15- 20%) Lateral wall
 Anterior wall, apex, Anterior 2/3 septum LAD ( %) Anterior wall, apex, Anterior 2/3 septum RCA (30- 40%) Post wall, post 1/3 septum RCA (30- 40%) Post wall, post 1/3 septum LCA (15- 20%) Lateral wall LCA (15- 20%) Lateral wall")
22
Role of Hemodynamic Changes Sudden drop in BP Sudden drop in BP Must be difference in pressure between coronary ostia and coronary sinus Must be difference in pressure between coronary ostia and coronary sinus

23
Role of Vasospasm Vasospasm documented in angina Vasospasm documented in angina Spasm can cause rupture of plaques Spasm can cause rupture of plaques Rare cases of MI after spasm Rare cases of MI after spasm

24
Role of Platelet Rupture of Plaques > adherence Rupture of Plaques > adherence The aggregation contributes to blockage The aggregation contributes to blockage Thromboxane, histamine, serotonin => vasospasm Thromboxane, histamine, serotonin => vasospasm ASA helps ASA helps

25
Supply of O2 in the Blood Anemia Anemia CO and cyanide CO and cyanide O2 demand O2 demand Hypertension Hypertension Valvular disease Valvular disease Hyperthyroidism Hyperthyroidism Fever Fever Catecholamines Catecholamines (? personality types) (? personality types)
 (. personality types).")
26
Role of acute Plaque Change in MI Hemorrhage into the atheroma - expanding its volume Hemorrhage into the atheroma - expanding its volume Rupture or fissuring, exposing the highly thrombogenic plaque constituent Rupture or fissuring, exposing the highly thrombogenic plaque constituent Erosion or ulceration Erosion or ulceration Note that the original plaque may not have been a significant lesion (no critical stenosis Note that the original plaque may not have been a significant lesion (no critical stenosis

27
Time of Day Peak incidence of MI: 6am to noon Peak incidence of MI: 6am to noon Adrenergic stimulation of awakening can put more stress on the plaque Adrenergic stimulation of awakening can put more stress on the plaque Surge of blood pressure at same time frame Surge of blood pressure at same time frame

28
Key Events in Ischemic Damage FeatureTime Onset of ATP depletion seconds Loss of contractility < 2 min ATP reduced to 50% to 50% 10 min to 10% to 10% 40 min Irreversible cell injury 20 -40 min Microvascular injury > 1 hr

29
Gross Changes of MI Up to 5 hours- no changes Up to 5 hours- no changes 6-24 hour- pallor 6-24 hour- pallor 24-48 hours- central pallor - hyperemia at margins 24-48 hours- central pallor - hyperemia at margins 2-5 days - hyperemic border, yellow band, soft dull center 2-5 days - hyperemic border, yellow band, soft dull center 5-10 days- broader yellow border and thin new pink border 5-10 days- broader yellow border and thin new pink border 10 days-3 wks - islands of red brown tissue surrounded by red-purple granulation tissue 10 days-3 wks - islands of red brown tissue surrounded by red-purple granulation tissue 3-6 weeks - fibrosis 3-6 weeks - fibrosis

30
Acute myocardial infarct

32
Acute MI - 4 days

33
Acute MI

34
Myocardial changes

35
Histology of MI 0-6 hours - none (? waviness) 0-6 hours - none (? waviness) 6-24 hours- eosinophilia, loss of cross striation 6-24 hours- eosinophilia, loss of cross striation 24-48 hours- coagulative necrosis, PMN 24-48 hours- coagulative necrosis, PMN 2-5 days- phagocytosis, granulation tissue 2-5 days- phagocytosis, granulation tissue 10 days - 3weeks increasing fibrosis, PMN’s disappear 10 days - 3weeks increasing fibrosis, PMN’s disappear 3-6 weeks - maturing fibrosis 3-6 weeks - maturing fibrosis
 6-24 hours- eosinophilia, loss of cross striation 6-24 hours- eosinophilia, loss of cross striation hours- coagulative necrosis, PMN hours- coagulative necrosis, PMN 2-5 days- phagocytosis, granulation tissue 2-5 days- phagocytosis, granulation tissue 10 days - 3weeks increasing fibrosis, PMN’s disappear 10 days - 3weeks increasing fibrosis, PMN’s disappear 3-6 weeks - maturing fibrosis 3-6 weeks - maturing fibrosis.")
36
Normal myocardium – note central nuclei and intercalated disks

37
Early ischemia- contraction bands

38
Early MI – coagulation necrosis. Pyknosis and karyolysis of nuclei

39
Early coagulation necrosis- loss of myocyte nuclei

40
MI 4days

41
Later coagulation necrosis – infiltration of neutrophils

42
Remote infarct – fibrous scar

43
Complications of MI Arrhythmias (90%) Arrhythmias (90%) CHF 60% CHF 60% Cardiogenic shock 10% Cardiogenic shock 10% Rupture (wall, septum, PAP M.) 5-10% Rupture (wall, septum, PAP M.) 5-10% Mural thrombus and embolism Mural thrombus and embolism Pericarditis Pericarditis Ventricular Aneurysms Ventricular Aneurysms Papillary muscle dysfunction Papillary muscle dysfunction
 Arrhythmias (90%) CHF 60% CHF 60% Cardiogenic shock 10% Cardiogenic shock 10% Rupture (wall, septum, PAP M.) 5-10% Rupture (wall, septum, PAP M.) 5-10% Mural thrombus and embolism Mural thrombus and embolism Pericarditis Pericarditis Ventricular Aneurysms Ventricular Aneurysms Papillary muscle dysfunction Papillary muscle dysfunction")
44
Complications of MI – Hemopericardium due to rupture

45
Rupture of myocardial infarct hemopericardium Area of infarct

46
MI with rupture

47
Rupture of myocardial infarct

48
Rupture of ventricular septum– giving rise to Acute right heart failure

49
Rupture of papillary muscle

50
Infarct of papillary muscle – leading to mitral valve dysfunction

51
Mural thrombus

52
Ventricular aneurysm due to MI - with mural thrombus thrombus

53
Diagnosis of MI Symptoms and signs Symptoms and signs 1/2 may be silent 1/2 may be silent EKG- New Q-wave, S-T segment and T-wave changes EKG- New Q-wave, S-T segment and T-wave changes Enzymes, CK, (CKMB), Troponins Enzymes, CK, (CKMB), Troponins Drs. Lynch & Baltaro will talk more about this Drs. Lynch & Baltaro will talk more about this

54
Subendocardial Infarct- non Q wave infarct severe ASCD severe ASCD no critical stenosis no critical stenosis Multifocal or bridges arterial zones Multifocal or bridges arterial zones diabetes diabetes Dangerous Dangerous

55
Infarct Modification After Reperfusion Reperfusion early- may prevent most necrosis Reperfusion early- may prevent most necrosis Hemorrhage - leaky damaged vessels Hemorrhage - leaky damaged vessels Necrosis with contraction bands Necrosis with contraction bands Increased oxygen free radicals Increased oxygen free radicals

56
Effects of reperfusion

Similar presentations



 less deleterious than ischemia Also called coronary.>")















 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")

 Includes Stable angina Acute coronary syndromes Sudden cardiac death due to.>")