Download presentation
Presentation is loading. Please wait.

1
Onchematologic emergencies
Dr. Demeter Judit Semmelweis Egyetem ÁOK., I.sz. Belgyógyászati Klinika

2
Onkohematologic emergencies
Hemodynamic - vena cava superior syndrom NHL - pericardial tamponade lymphomas - hyperviscosity syndrome MM, Wald. - thrombosis myeloprolif. Hematologic - bleeding qualitative-quantitive pathologies of platelets ITP lack of coagulation factors DIC (M3) Nervous system - spinal cord compression NHL, MM immediate MR! - koponyaűri nyomásfokozódás NHL Metabolic - tumorlysis syndrome hyperuricaemia, hyperkalaemia - hypercalcaemia MM, NHL - hypokalaemia AML - hypoglykaemia insulinoma Other - TTP/HUS
 Nervous system - spinal cord compression NHL, MM immediate MR! - koponyaűri nyomásfokozódás NHL. Metabolic - tumorlysis syndrome hyperuricaemia, hyperkalaemia - hypercalcaemia MM, NHL - hypokalaemia AML - hypoglykaemia insulinoma. Other - TTP/HUS.")
3
Incidence: number of patients with hematologic and oncologic malignancies is increasing The number of patients presenting with hemato-oncologic emergencies is expected to be increasing

4
Prospects: patients cancer no longer should be looked upon as incurable and terminal even not even in the emergency departments Patients are to some degree amenable to therapy or intervention Following the succcesful treatment of an emergency condition, these patients may lead relatively normal lives.

5
mechanical emergencies
1.neutropenic fever. the most common ! mechanical emergencies airway obstruction, superior vena cava syndrome cardiac tamponade spinal cord compression. metabolic emergencies. hyperviscosity syndrome hypercalcemia syndrome of inappropriate antidiuretic hormone secretion (SIADH) acute tumor lysis syndrome. Often missed! superior sulcus lung tumor (Pancoast syndrome).
 acute tumor lysis syndrome. Often missed! superior sulcus lung tumor (Pancoast syndrome).")
6
Infectious Emergencies Neutropenic Fever
appropriate recognition and management may significantly lessen morbidity and mortality! Neutropenia absolute granulocyte count is < 500 cells/µL or < 1000 cells/µL with an anticipated decrease to < 500 cells/µL. nadir mostly between 2-4 weeks after chemotherapy Fever if if temperature exceeds >38.3° (101° F) or if the temperature = 38.0° C (100.4° F) for > 1 hour.
 or. if the temperature = 38.0° C (100.4° F) for > 1 hour.")
7
lack of circulating white blood cells.
few of the classic signs and symptoms of bacterial infections e.g. significant pneumonia without cough or infiltrates on plain film. urinary tract infection without WBC deposition in the urinary tract , lack of dysuria and frequency. meningitis may present without clinical evidence of meningismus or cerebral spinal fluid pleocytosis. Febrile neutropenia: cultures of blood and urine chest x-ray performed (chest CT even better!) if indwelling central line : at least one set of blood culture through it!
 if indwelling central line : at least one set of blood culture through it!")
8
Immediate empiric antibiotic therapy!
( because progression of infection in neutropenic patients may be very rapid) Initial antibiotic therapy should be tailored to the suspected offending pathogens. In the not too distant past, neutropenic patients were covered with two antibiotics, typically a third-generation cephalosporin in combination with an aminoglycoside. Traditionally, G-negative bacilli ( Pseudomonas, E coli, and Klebsiella): most common offending pathogens. Nowadays: increase in the rate of infections caused by gram-positive bacteria, (some of them methicillin-resistant) . Staphylococcus aureus coagulase-negative staphylococci most common causes, particularly in patients with an indwelling catheter Recommended: single agent antimicrobial therapy (monotherapy). third or fourth-generation cephalosporin (ceftazidime or cefipime) or a carbapenem (imipenem-cilastatin or meropenem)
 Initial antibiotic therapy should be tailored to the suspected offending pathogens. In the not too distant past, neutropenic patients were covered with two antibiotics, typically a third-generation cephalosporin in combination with an aminoglycoside. Traditionally, G-negative bacilli ( Pseudomonas, E coli, and Klebsiella): most common offending pathogens. Nowadays: increase in the rate of infections caused by gram-positive bacteria, (some of them methicillin-resistant) . Staphylococcus aureus. coagulase-negative staphylococci most common causes, particularly in patients with an indwelling catheter. Recommended: single agent antimicrobial therapy (monotherapy). third or fourth-generation cephalosporin (ceftazidime or cefipime) or a carbapenem (imipenem-cilastatin or meropenem)")
9
clinically-suspected serious catheter-related infections
. Include vancomycin in the treatment if: clinically-suspected serious catheter-related infections known colonization with methicillin-resistant Staphylococcus aureus positive results of blood culture for gram-positive bacteria before final identification and susceptibility are known hypotension or other clinical evidence of cardiovascular impairment Growth factor treatment: filgrastim (Neupogen). stimulates WBC production reduces the duration of neutropenia and fever, reduces the requirement of parenteral antibiotics reduces the duration of hospitalization. safe even in acute leukemia Granulocyte transfusion not recommended!
. stimulates WBC production. reduces the duration of neutropenia and fever, reduces the requirement of parenteral antibiotics. reduces the duration of hospitalization. safe even in acute leukemia. Granulocyte transfusion not recommended!")
10
Management of neutropenic fever
1. initial antibiotic of choice: third or fourth generation cephalosporin or a carbapenem. (single agent therapy) 2. Cultures of blood and urine ! 3. Consider chest CT if pulmonary symptoms present (active pulmonary infections may be present despite normal chest x-rays) 4. Vancomycin if indwelling intravenous catheter infection suspected (in addition to gram-negative coverage). 5. rapid institution of empiric antibiotic therapy reduces morbidity and mortality. 6. reverse isolation room.
 2. Cultures of blood and urine ! 3. Consider chest CT if pulmonary symptoms present (active pulmonary infections may be present despite normal chest x-rays) 4. Vancomycin if indwelling intravenous catheter infection suspected. (in addition to gram-negative coverage). 5. rapid institution of empiric antibiotic therapy reduces morbidity and mortality. 6. reverse isolation room.")
11
Mechanical Emergencies:
Spinal Cord Compression any patient who presents with back pain may have spinal cord compression due to malignancy!

12
She developed paralysis and incapacitating pain.
disseminated metastatic breast cancer to bone (after both chemotherapy and radiation therapy). She developed paralysis and incapacitating pain. MRI image: extensive bone tumor with collapse of the T10 and T11 vertebrae resulting in spinal cord compression.
. She developed paralysis and incapacitating pain. MRI image: extensive bone tumor with collapse of the T10 and T11 vertebrae resulting in spinal cord compression.")
13
Epidural spinal cord compression
devastating complication of many malignancies breast lung prostate cancer AML (chloroma) muItiple myeloma Frequency ca. 5% Importance of early detection in remaining ambulatory!
 muItiple myeloma. Frequency ca. 5% Importance of early detection in remaining ambulatory!")
14
Epidural spinal cord compression
Might be the first clinical manifestation of malignancy. Pts with known diagnosis of cancer (breast, lung, prostate, renal) + back pain potentially lethal back pain entities cancer cauda equina syndrome abdominal aortic aneurysm, back pain and a history of malignancy should be assumed to be metastasis to the spine or epidural spinal cord compression until proven otherwise
 + back pain. potentially lethal back pain entities. cancer. cauda equina syndrome. abdominal aortic aneurysm, back pain and a history of malignancy should be assumed to be metastasis to the spine or epidural spinal cord compression until proven otherwise.")
15
Epidural spinal cord compression
Presenting symptoms numbness tingling sensory loss bowel or bladder incontinence abnormalities of proprioception e.g.loss of vibratory sense back pain worsened by particular maneuvers, such as (coughing or lying in a supine position pain that is worse at night. New-onset radiculopathy from compression of a spinal root may also be the first manifestation of tumor (DDG: A herniated disc)
")
16
Epidural spinal cord compression
The physical examination may show evidence of spinal cord compression with paralysis or may be completely normal and unrevealing. A detailed motor, sensory, and deep tendon reflex examination should be performed in all patients with suspected spinal cord compression, as well as observation of gait and evaluation of sphincter tone

17
Epidural spinal cord compression
think about the diagnosis in patients with back pain! Dg-ic workup: Magnetic resonance imaging epidural spinal cord compression can be subtle, and detection requires a high index of suspicion! Treatment: high dose corticosteroids - decompressive laminectomy - radiation

18
Epidural spinal cord metastasis and/or compression.
Pain may be the only finding ! Suspicious: Pain worsened by cough or the supine position 2. Physical examination: midline bony tenderness (often absent), ataxic gait weakness autonomic dysfunction (bowel or bladder incontinence). 3. Corticosteroids –iv. immediately! 4. Think about the diagnosis!
, ataxic gait. weakness. autonomic dysfunction (bowel or bladder incontinence). 3. Corticosteroids –iv. immediately! 4. Think about the diagnosis!")
19
Superior Vena Cava Syndrome
becomes an emergency with the development of cerebral edema (life-threatening cerebral herniation) or laryngeal edema (leading to airway compromise) Causes: ( tuberculosis, aortic aneurysm, and fibrosing mediastinitis) Nowadays: lung carcinoma lymphoma catheter-related superior vena cava thrombosis.
 or. laryngeal edema (leading to airway compromise) Causes: ( tuberculosis, aortic aneurysm, and fibrosing mediastinitis) Nowadays: lung carcinoma. lymphoma. catheter-related superior vena cava thrombosis.")
20
Thickening of the prevertebral soft tissue shadow indicates laryngeal edema

21
Superior Vena Cava Syndrome
Clinical manifestations: protean depend on the degree of vena cava obstruction. Fom relatively asymptomatic with only mild facial fullness when bending forward or may have florid symptoms of facial swelling, headache, and airway compromise.

22
A clue to the diagnosis is the presence of asymmetric neck, chest, or upper arm venous distension.
One diagnostic tool that has been employed by some is to compare the patient’s appearance to that of a picture of the patient, often a driver’s license Subtle and sometimes marked changes in the physical appearance of the patient’s face can be identified.

23
The key to understanding the variability of the clinical presentation is the anatomy of the azygous vein. The azygous vein is a large vessel that enters the proximal superior vena cava and drains blood from the thorax. Obstruction above the level of the azygous entry point may lead to relatively few symptoms due to the ability of the azygous to decompress the upper extremities, head, and neck. If a compressive lesion or thrombus obstructs the SVC below the entry point there is no mechanism for upper torso, head, and neck decompression, and patients may present with marked venous collateral formation and facial swelling on examination .

24
dezsine

25
Patient’s driver’s license before cancer diagnosis-
Picture 1 year later

28
Superior vena cava syndrome
Traditional teaching : most patients present with a sensation of facial fullness, facial swelling, cough, variable arm swelling, and dilated neck and upper chest wall veins, with these it would not be a difficult diagnosis to make. However, this oncologic entity may present with few if any clinical findings. Further frequent symptom: sensation of fullness when bending forward or a vague, chronic cough. However, if venous decompression is able to occur, there will be no prominent veins or facial swelling the diagnosis may not even be considered.

29
Depiction of the azygous vein (denoted by asterisk)
Depiction of the azygous vein (denoted by asterisk). Diagram on the left indicates point at which the azygous enters the SVC and its relationship to intercostal vessels.
. Diagram on the left indicates point at which the azygous enters the SVC and its relationship to intercostal vessels.")
30
Treatment aim: alleviating congestive symptoms while simultaneously attempting to make a definitive diagnosis. In cases where suspected or confirmed lung cancer or lymphoma is the cause, institution of radiation therapy may help lessen venous congestion and reduce upper torso, head, and neck venous pressure. Previously, superior vena cava syndrome was considered an emergency. Today, emergent radiation therapy should be reserved for patients with life-threatening laryngeal or cerebral edema.

31
Patients with a confirmed or suspected diagnosis of SVC syndrome
based on clinical grounds should undergo CT scanning to define the degree of SVC obstruction and to evaluate for the possibility of thrombotic SVC occlusion (10). If no known tissue diagnosis of cancer has been done, a biopsy is typically performed as an outpatient or inpatient. Adjunctive treatment modalities such as steroids and diuretic therapy may be used, particularly if head and neck edema is a prominent feature.
. If no known tissue diagnosis of cancer has been done, a biopsy is typically performed as an outpatient or inpatient. Adjunctive treatment modalities such as steroids and diuretic therapy. may be used, particularly if head and neck edema is a prominent feature.")
32
Superior vena cava syndrome caused by lung carcinoma
Superior vena cava syndrome caused by lung carcinoma. Notice the ruddy appearance of the patient's face caused by elevation of the arm - Pemberton's sign.

33
Superior vena cava syndrome
1. A complaint of facial swelling should be enough to make the emergency physician consider the diagnosis of SVC syndrome. Partial SVC occlusion or compression above the azygous vein may not lead to any physical exam findings. 2. Hoarseness may be a subtle clue when laryngeal edema has developed. 3. Stoke’s sign - Face and neck swelling seen in SVC syndrome 4. Relatively rare but pathognomonic of SVC syndrome is supine facial cyanosis: development of facial cyanosis when the patient is placed in the supine position. 5. Subtle presentations are common and include fatigue (due to poor venous return), dyspnea, chest pain, headache, face and neck swelling, and facial flushing. 6. Incidence of thrombotic SVC syndrome is on the rise. 7. Symptoms tend to be worse upon awakening secondary to venous pooling.
, dyspnea, chest pain, headache, face and neck swelling, and facial flushing. 6. Incidence of thrombotic SVC syndrome is on the rise. 7. Symptoms tend to be worse upon awakening secondary to venous pooling.")
34
Clinical presentation of a patient with superior vena cava syndrome.

36
Injury/Microorganisms Microcirculatory disturbances
DIC Injury/Microorganisms Activation of -PMN -Macrophage -Endothelium Cytokines Systemic activation of coagulation fibrin formation Toxins Microclot formation Consumption of coagulation factors and inhibitors Secondary fibrinolysis Microcirculatory disturbances Bleeding Organfailure

37
Thrombotic microangiopathies
A THROMBOTIC THROMBOCYTOPENIc PURPURA (TTP) ÉS A HAEMOLYTIC URAEMIC SYNDROM (HUS) Have microvascular platelet aggregation in common But.: TTP can be regarded as a systemic dsorder, HUS: is localized to the kidneys. TTP és HUS have very many similarities . Similar starting events :… TTP/HUS complex
 ÉS A HAEMOLYTIC URAEMIC SYNDROM (HUS) Have microvascular platelet aggregation in common. But.: TTP can be regarded as a systemic dsorder, HUS: is localized to the kidneys. TTP és HUS have very many similarities . Similar starting events :….. TTP/HUS complex.")
38
TTP and HUS consumptive thrombocytopenia
microangiopathic haemolytic anaemia ischaemic symptoms TTP HUS TTP HUS

39
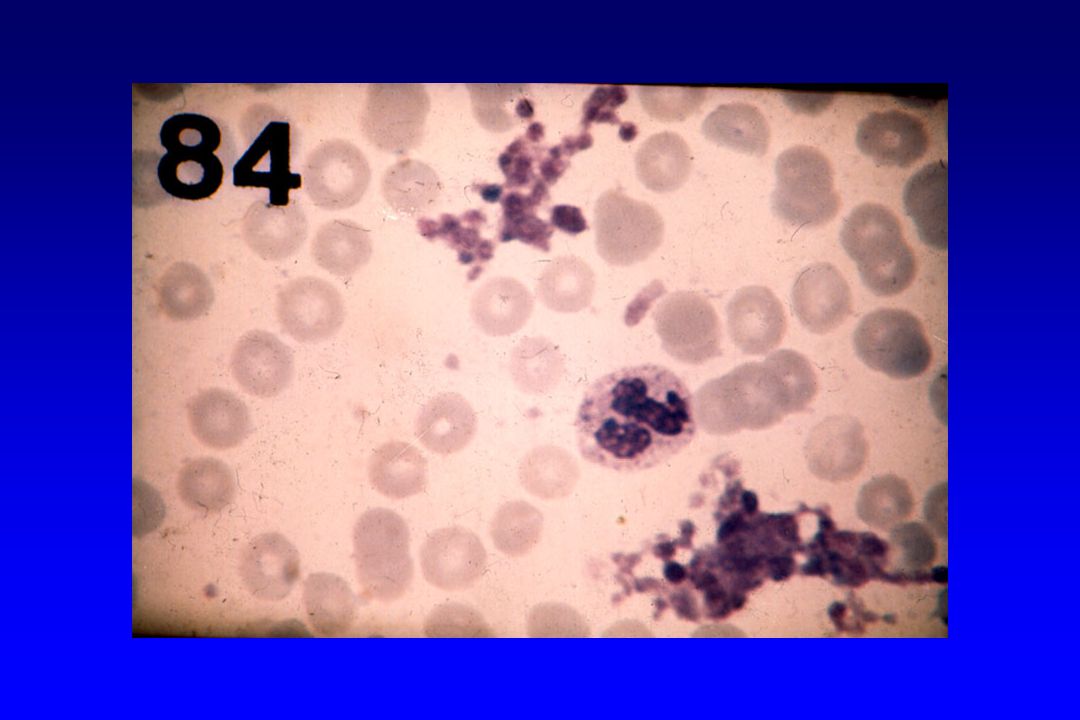
Diagnostics, morphology
Megakaryocytic thrombocytopenia Fragmentocytes

40
Thrombotic thrombocytopenic purpura ( Moschcowitz syndrome, 1924)
Incidence: 30 patients have to be treated in Hungary yearly Mortality of untreated cases : %. A diagnostic criteris: (first 2 criteria are sufficient) Severe consumptive thrombocytopenia, - plenty of megakaryocytes Fragmentocytic haemolytic anaemia, direct Coombs neg Fluctuating neurologic symptoms Kidney involvement – renal failure Fever
 Severe consumptive thrombocytopenia, - plenty of megakaryocytes. Fragmentocytic haemolytic anaemia, direct Coombs neg. Fluctuating neurologic symptoms. Kidney involvement – renal failure. Fever.")
41
TTP – clinical pentade Moschcowitz: 1924 consumptiive thrombocytopenia
microangiopathic hemolytic anaemia fluctuating neurológical symptoms Kidney involvement – renal failure fever triad: %, pentade: 40 %

42
TTP -frequency incidence: 1-7 / 1 million inhabitants / year
Typical age: decade female : male ratio: 3 : 2 Mortality before1960: > 90 % Mortality after : %

43
TTP – clinical forms Acute (single episode) TTP: no relapse
Intermittent TTP: relapse occurring irregularly Chronic cyclic TTP: relapse at regular intervals

44
Differentialdiagnosis:
DIC HELLP sy ITP Evans sy Antiphospholipid sy Liver diseases Paroxysmal nocturnal haemoglobinuria (PNH) Other causes of mechanical hemolysis (arteficial valve, etc.)
 Other causes of mechanical hemolysis (arteficial valve, etc.)")
45
Haemolytic uremic syndrome
A diagnostic criteria: all the three have to be present) Thrombocytopenia, number megakaryocytes in the BM normal or increased. Fragmentocytic haemolytic anaemia, a direkt Coombs test negatíve (kivéve: neuraminidase infekciókhoz társuló secunder formák). Variable degree of kidney involvement, kidney failure Clinical forms: Diarrhoea-asszociated or típical HUS: benign form, mortality less than 10 % . Sporadic or atypical HUS, high mortality, (ca..70 %.) no accurate data on incidence.
 Thrombocytopenia, number megakaryocytes in the BM normal or increased. Fragmentocytic haemolytic anaemia, a direkt Coombs test negatíve (kivéve: neuraminidase infekciókhoz társuló secunder formák). Variable degree of kidney involvement, kidney failure. Clinical forms: Diarrhoea-asszociated or típical HUS: benign form, mortality less than 10 % . Sporadic or atypical HUS, high mortality, (ca..70 %.) no accurate data on incidence.")
46
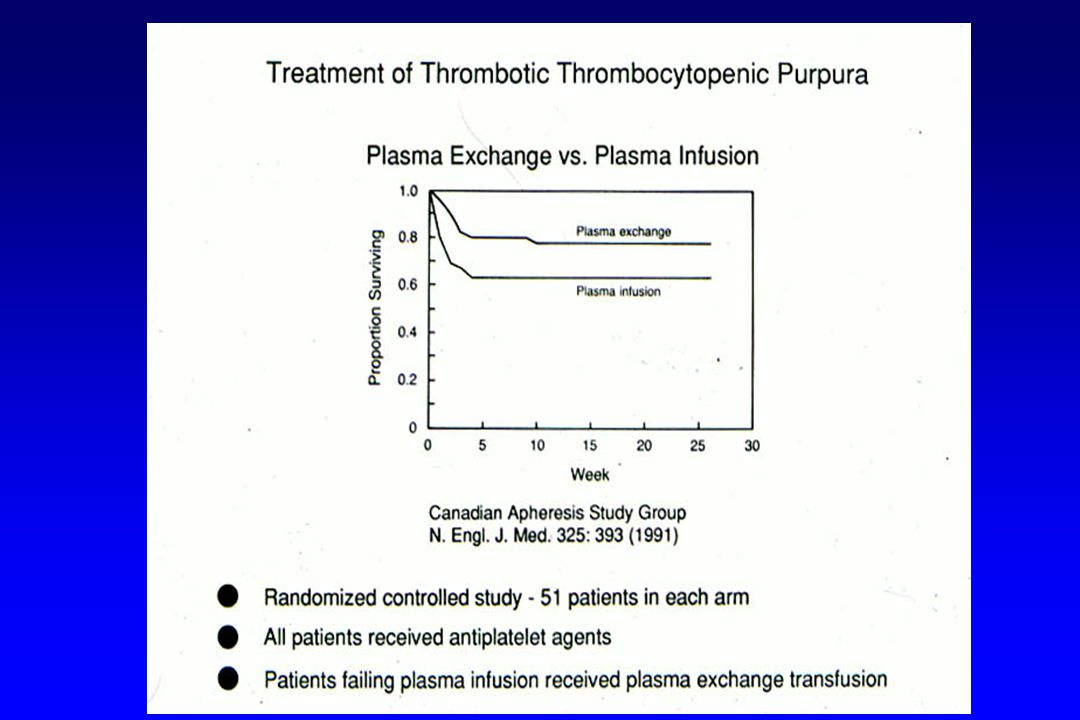
Treatment of TTP and HUS
aim: curative. Only in hospitals with intensive care units Treatment: Plasmaexchange, daily,, substitution with fresh frozen plazma or cryo-supernatant : thus % of patients might be cured. Alternativ therapy: Fresh frozen plasma or infusion of fresh frozen plasma: signifivcatnlyx less effective than plasma exchange, Futher drug therapies Corticosteroids - Thrombocyta aggregácion inhibitors? - Vincristine - Immunosuppressive drugs - potentially high dose iv. Ig

47
Supportív therapy: RBC transfusion, Platelet transfusion is usually contraindicated! Treatment of infections Dialysis Intensive care unit (ritkán gépi lélegeztetés, parenterális táplálás) Treatment of precipitating cause in the case of secondary forms
 Treatment of precipitating cause in the case of secondary forms.")
48
Hematological indications of apheresis I.
Hyperleukocytosis Leukostasis High peripheral cell counts + chemotherapy causing acute cytolysis High peripheral cell counts + organomegaly causing severe compression symptoms Extremely hig cell numbers a. myeloproliferatív sy: WBC > 300 G/l b. lymphoproliferatív sy: WBC > 500 G/l Thrombocytosis With complications (threatening ot manifest thrombosis and/or bleeding plt > 1000 G/l + pregnancy plt > 1000 G/l + before a planned operation or coronarography ( maximally 2 aphereses végezhető) 4. thr > 1000 G/l + thrombophilia proven by a laboratory test TTP Apheresis shlould be stopped in the case of hematological remission or (brain)death
 4. thr > 1000 G/l + thrombophilia proven by a laboratory test. TTP. Apheresis shlould be stopped in the case of hematological remission or (brain)death.")
49
HUS Gasser: 1955 consumptive thrombocytopenia
microangiopathic haemolytic anaemia Acute renal failure

50
Typical HUS (diarrhoea associated)
verotoxin / shigatoxin Characteristic prodromal phase endemic Young age (< 5 years) low mortality rare relapse following kideny transplantation
 low mortality. rare relapse following kideny transplantation.")
51
Sporadic (atypical) HUS (not diarrhoea associated)
not verotoxin / shigatoxin associated No characteristic prodromal phase not endemic elder age (> 5 years) high mortality frequent relapse following kidney transplantation
 high mortality. frequent relapse following kidney transplantation.")
52
Etiology idiopathic familiar secundary
infections: verotoxin / shigatoxin neuraminidase HIV other Pregnancy and postpartum period Autoimmune disorders tumors, chemoterápy drug: kinin, ticlopidin, (clopidogrel), cyclosporin, tacrolimus, mitomycin, contraceptives, stb Allogeneic stem cell transplantation
, cyclosporin, tacrolimus, mitomycin, contraceptives, stb. Allogeneic stem cell transplantation.")
53
Feltételezett pathomechanizmus
prostacyclin termelés zavarai csökkent fibrinolysis exogen toxinok, enzimek thr aggregáló faktorok pap37 calpain endothel sejt apoptosis autoimmun mechanizmus autoantitest: endothel, CD36 immunkomplex vWF eltérései

54
Jelenlegi hypothesis (a distintegrin and metalloprotease with eight
TTP-s microthrombosisok: vWF + thr kóros vWF multimer eloszlás (ULvW) nyíróerő: vWF - direkt thr aggregáció áramlási cytometria: thr-hoz kötött vWF FFP vagy cryofelülúszó transzfúziója klinikai remissio vWF multimer eloszlás normalizálódása vWF cleaving protease: ADAMTS13 (a distintegrin and metalloprotease with eight thrombospondin-1-like domains) 9q34 kromoszóma ADAMTS13 enzimaktivitás csökkenése/hiánya autoantitest - ADAMTS13 enzim inhibitor congenitális enzimhiány
 nyíróerő: vWF - direkt thr aggregáció. áramlási cytometria: thr-hoz kötött vWF. FFP vagy cryofelülúszó transzfúziója. klinikai remissio. vWF multimer eloszlás normalizálódása. vWF cleaving protease: ADAMTS13. (a distintegrin and metalloprotease with eight. thrombospondin-1-like domains) 9q34 kromoszóma. ADAMTS13 enzimaktivitás csökkenése/hiánya. autoantitest - ADAMTS13 enzim inhibitor. congenitális enzimhiány.")
55
VWF Cleaving Protease (ADAMTS13)
Metalloprotease Thrombospondin 1 CUB S M P Cys D Spacer 1 2 3 4 5 6 7 8 Disintegrin A Disintegrin-like And Metalloprotease with ThromboSpondin-1 repeats

56
Laboratory abnormalities.
microangiopathic haemolytic anaemia fragmentocytosis, nucleated RBCs basophil punctation reticulocytosis negatív direct Coombs teszt Slightly elevated indirekt se-bi Reduced or non-detectable serum haptoglobin haemoglobinuria, haemosiderinuria thrombocytopenia thr << 50 G/l (TTP) thr < G/l (HUS)
 thr < 100 G/l (HUS)")
57
Laboratory abnormalities - 2
Significantly elvated serum-LDH (2-20x) se-kreatinin variable (TTP) increased (HUS) Hemostatic abnormalities normál prothrombin, PTI, fibrinogén Urine haematuria, proteinuria, cylinders CRP: normal or slightly increased Liver enzymes: normal or slightly increased
 se-kreatinin. variable (TTP) increased (HUS) Hemostatic abnormalities. normál prothrombin, PTI, fibrinogén. Urine. haematuria, proteinuria, cylinders. CRP: normal or slightly increased. Liver enzymes: normal or slightly increased.")
58
Differentialdiagnosis
TTP or HUS DIC (pre)eclampsia / HELLP sy systemic vasculitides thrombocytopenia or haemolysis of other causes
eclampsia / HELLP sy. systemic vasculitides. thrombocytopenia or haemolysis of other causes.")
59
Treatment results – empiric plasma therapy
Idiopathic TTP/HUS complete haematological remission: % Relapse within 10 years: % Secundary TTP/HUS Variable, depends on underlying cause

60
Evidence based plasmaexchange since the early 1990-s
: plazmaexchange / plasma transfusion : prospektíve randomized controlled study plasmaexhange or plazma transfusion? - Rock: N Engl J Med 1991;325:393 - Henon: Transfus Sci 1992; 13:63 PLASMAEXCHANGE!

62
Hematological indications of apheresis – II.
HUS 1. All adult cases 2. Childhood atypical HUS 3. Childhood therapy resistant HUS Apheresis should be stopped at the time of haematoligical remission independent of the renal status HELLP sy thrombocytopenia, haemolysis, SGOT >70 U/l, LDH>600 U/l, if: Symptoms persist hours follwing termiantion of pregnancy resistant to conservative treatment With postpartum eclampsia The usual gynecologic causes of DIC should be excluded before start of apheresis

63
Hematologial indication of apheresis – III.
Gammopathies hyperproteinaemia: total protein > 100 g/ 2. hyperviscosity sy: blood viscosity is more than 15 % above what is normal for the given Ht Acute renal failure caused by paraprotein 4. polyneuropathy Cryoglobulinaemia kryokrit > 1 %, if 1. Raynaud sy and/or necrotising cutan vasculitis 2. cryoglobulinaemic vasculitis Cold type AIHA haemolytic crisis Masszíve intravasal haemolysis Impending renal failure

64
Hypercalcaemia malignus betegségekben
Általános jellemzők

65
Hypercalcaemia non-Hodgkin lymphomákban
Gyakorisága: összes NHL 4%-a (9/219) (kifejezett mal. NHL: 30%) Mechanizmusa: calcitriol-mediált (19 esetben egyidejű hypercalcaemia és hypercalcitriolaemia) a növekedett calcitriol szint valószínűleg extrarenalis eredetű nincs jellemző csontváltozás
 (kifejezett mal. NHL: 30%) Mechanizmusa: calcitriol-mediált (19 esetben egyidejű hypercalcaemia és hypercalcitriolaemia) a növekedett calcitriol szint valószínűleg extrarenalis eredetű. nincs jellemző csontváltozás.")
66
In patients taking salicilates, ticlopidin or clopidogrel, no operation should be performed ( no stomatological procedure!)
")
67
A calcitriol-mediált hypercalcaemia kezelése
corticosteroid önmagában is hatásos további kezelési lehetőségek Csontokból calciummobilizáció gátlása (osteoclastok gátlása: calcitonin, biszfoszfonátok) bélből calciumfelszívódás csökkentése: Ca szegény étrend renalis calciumürítés csökkentése hypovolaemia korrekció FONTOS TOVÁBBÁ: - UV sugárzás kerülése - D vitamin bevitel kerülése
 bélből calciumfelszívódás csökkentése: Ca szegény étrend. renalis calciumürítés csökkentése hypovolaemia korrekció FONTOS TOVÁBBÁ: - UV sugárzás kerülése - D vitamin bevitel kerülése.")
71
Ferezissel eltávolított leukémiás massza ( 10 l feletti)
CML blasztos fázisban diagnosztizált 34 éves beteg esetében

Similar presentations