Download presentation
Presentation is loading. Please wait.

1
Thalassaemia in Children’s Hospital By: Khounthavy

2
INITIAL EVALUATION

3
Evaluating Anemia Patient Age, Height, Body weight Lymphadenomegaly, Hepatosplenomegaly Fatigue/Heart Sound Tongue size …. CBC (18P) –WBC/Hb/Hct/PLT MCV MCH Reti(%) –Absolute Reticulocyte Count (Reticulocyte Index) Iron Profile –Serum Ferritin / Serum Iron / TIBC Peripheral Blood Smear (Morphology) Hemoglobin Typing ??
 –WBC/Hb/Hct/PLT MCV MCH Reti(%) –Absolute Reticulocyte Count (Reticulocyte Index) Iron Profile –Serum Ferritin / Serum Iron / TIBC Peripheral Blood Smear (Morphology) Hemoglobin Typing .")
4
Nelson Pediatrics Table 447-1

5
Nelson Pediatrics Figure 447-2

6
Response of Anemia –Kidney -> EPO –EPO -> Bone Marrow –Bone marrow : Produces more RBCs –Reticulocyte : Young RBC (RBC nyang bor souk) Anemia with Low Reti –Bone Marrow function not normal –IDA, Vit B12 Def Anemia with High Reti –Bone Marrow function intact –Blood loss, Hemolysis
 Anemia with Low Reti –Bone Marrow function not normal –IDA, Vit B12 Def Anemia with High Reti –Bone Marrow function intact –Blood loss, Hemolysis")
7
Absolute Reticulocyte Count –(% of Reti) X (Pt’s Hct / Normal Hct) Reticulocyte Index –(Absolute Reticulocyte Count) / (Maturation Factors) Maturation Factors –Hct>35%: 1.0 –35%>Hct>25%: 1.5 –25%>Hct>20%: 2.0 –20%>Hct : 2.5
 X (Pt’s Hct / Normal Hct) Reticulocyte Index –(Absolute Reticulocyte Count) / (Maturation Factors) Maturation Factors –Hct>35%: 1.0 –35%>Hct>25%: 1.5 –25%>Hct>20%: 2.0 –20%>Hct : 2.5")
8
WWW.Medcalc.com

11
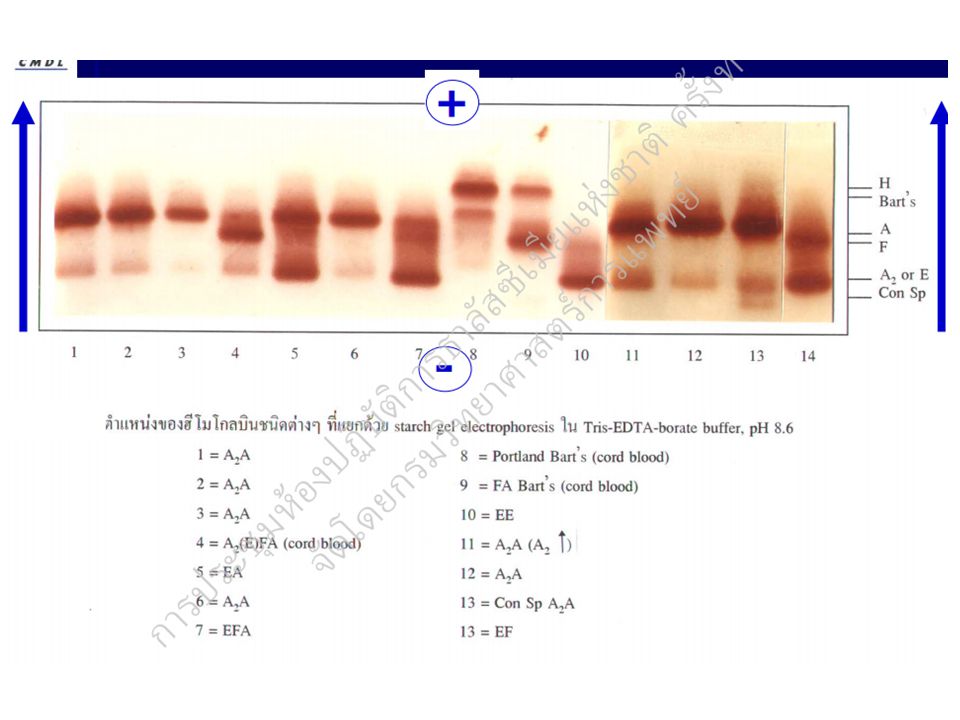
Hemoglobin typing Recommended after 1 year-old Electrophoesis or HPLC –Children’s Hospital ; Electrophoesis –Thai ; HPLC

12
Nelson Pediatrics

14
Normal Hb A= 2 2 (97%) HbA 2 = 2 2 (2.5%) Hb F= 2 2 (0.5%) -Thalassemia 4 =HbH 4 =HbBart’s -Thalassemia Increased HbA 2 (4-6%)
 HbA 2 = 2 2 (2.5%) Hb F= 2 2 (0.5%) -Thalassemia 4 =HbH 4 =HbBart’s -Thalassemia Increased HbA 2 (4-6%)")
15
11 22 11 22 11 22 11 22 11 CS thal 1 trait thal 2 trait Hb H-CS disease Hb Bart’s hydrops fetalis Normal thal 2 homozygote Hb H disease

16
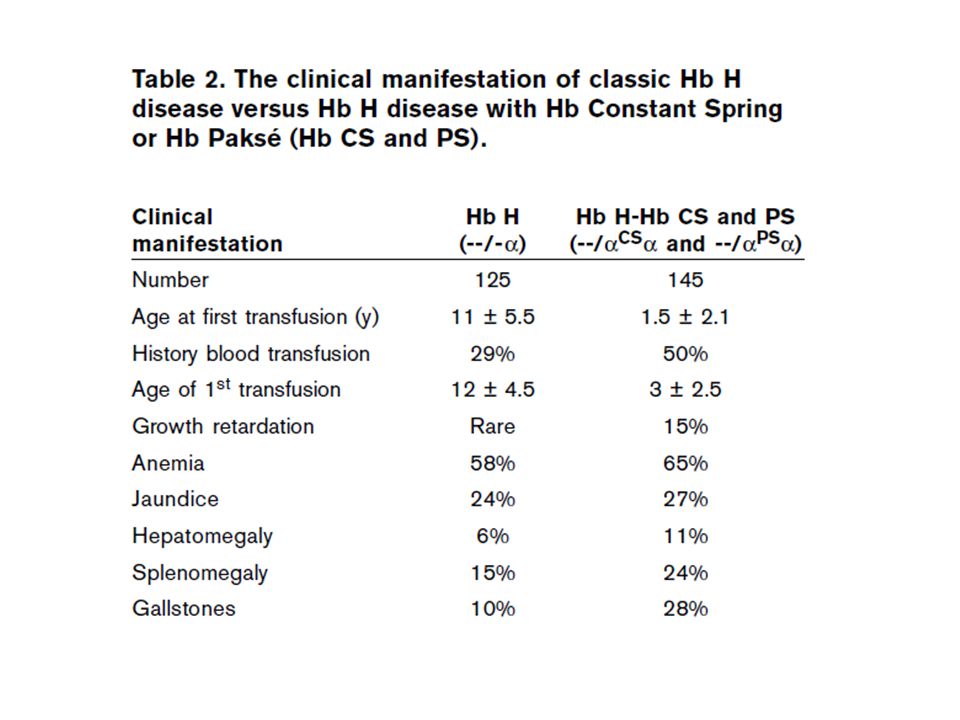
1 deletion of 4 genes –Silent 2 deletion of 4 genes –Moderate type 3 deletion of 4 genes –Hemoglobin H (β 4 ) –Tetramer of Beta Chain 4 deletion of 4 genes –Hydrops fetalis; Hemoglobin bart (γ 4 ) –Tetramer of Gamma Chain –Most severe (Fetal death) Non-deletional mutation in alpha gene –Hemoglobin CS Alpha-Thalassaemia
 –Tetramer of Beta Chain 4 deletion of 4 genes –Hydrops fetalis; Hemoglobin bart (γ 4 ) –Tetramer of Gamma Chain –Most severe (Fetal death) Non-deletional mutation in alpha gene –Hemoglobin CS Alpha-Thalassaemia")
17
Hydrops Fetalis

19
Beta-Thalassaemia

21
Variable Severity in -Thalassemia Disorder

22
Hemoglobin E Substitution of glutamic acid by lysine at codon 26 of Beta-globin gene Frequency ; 60% in Thai, Laos, Cambodia

24
-Thal 1/Hb E ( -Thal) 2 -Thal 1 ( -Thal 1) 2 Hb Bart’s Hydrops Hb Constant Spring (Hb CS) Hb E -Thal 2 Hb H Disease c Hb CS Hb H Disease c Hb CS Hb AEBart, s Disease c Hb CS Hb AEBart, s Disease c Hb CS - - Hb E -Thal -Thal/Hb E -Thal 2/Hb E (More than 60 genotypes ) -Thal 1/ -Thal -Thal/Hb E c -Thal 2 - (Hb CS) 2 (Hb E) 2
 2 -Thal 1 ( -Thal 1) 2 Hb Bart’s Hydrops Hb Constant Spring (Hb CS) Hb E -Thal 2 Hb H Disease c Hb CS Hb H Disease c Hb CS Hb AEBart, s Disease c Hb CS Hb AEBart, s Disease c Hb CS - - Hb E -Thal -Thal/Hb E -Thal 2/Hb E (More than 60 genotypes ) -Thal 1/ -Thal -Thal/Hb E c -Thal 2 - (Hb CS) 2 (Hb E) 2")
25
NoCountry/ Region Total Population (m) 0 -thal (%) + -thal (%) -thal (%) Hb E (%) Hb S (%) 1Australia18.90.100.40.10 2Cambodia10.9433.43.0300 3China, south2001.4*9.6*1.0+0 4Hong Kong6.85.014.53.000 5Indonesia207+7.74.01.90 6Laos5.32.0342.0270 7Malaysia22.71.83.11.75.5+ 8Myanmar45.10.4322.2250 9Philippines74.72.018.41.0 0 10Singapore3.93.512.13.0+0 12Taiwan21.54.05.12.000 13Thailand61.85.0215.3330 14Vietnam78.72.69.11.416.70 Grand Total757.3 Southeast/East Asia (2005) (B. Modell)
.")
26
THALASSEMIA IN THAILAND - Thalassemia 20 - 30 % Hb Constant Spring 1 - 8 % ( - thalassemia 2 like effect ) - Thalassemia 3 - 9 % Hemoglobin E 10 - 53 % - Thal 1 - Thal 2
 - Thalassemia % Hemoglobin E % - Thal 1 - Thal 2")
27
Hemoglobin E diseases : 58 (67%) E/β: 32 (37%) EA: 9 (10%) AE-Bart diseases: 14 (16%) E/E: 2 (2%) Hemoglobin H diseases: 40 (47%) Hb H: 16 (19%) Hb H-CS: 10 (12%) AE-Bart diseases: 14 (16%) β Thalassaemia (β/ β) 2 (2%) Thalassaemia in MCH (Mother and Child Hospital) Total 148 patients 86 patients had done Hb typing
 E/β: 32 (37%) EA: 9 (10%) AE-Bart diseases: 14 (16%) E/E: 2 (2%) Hemoglobin H diseases: 40 (47%) Hb H: 16 (19%) Hb H-CS: 10 (12%) AE-Bart diseases: 14 (16%) β Thalassaemia (β/ β) 2 (2%) Thalassaemia in MCH (Mother and Child Hospital) Total 148 patients 86 patients had done Hb typing")
28
Please ask or consult to Dr. Sourideth Dr. Bounhak (Eunsang LEE) Dr. Khounthavy Dr. Vasana Dr. Phatana

29
MANAGEMENT

30
Consult If the Result is hard to interpret please consult to these doctors –Dr. Sourideth –Dr. Bounhak (Eunsang LEE) –Dr. Khounthavy –Dr. Vasana –Dr. Phatana
 –Dr. Khounthavy –Dr. Vasana –Dr. Phatana.")
31
Iron Deficiency Anemia Iron Tablet 4~6mg/kg/day 4 weeks later check CBC for recovery If recovered continue to more 8 weeks Iron Syrup for Infants in Lao

32
Thalassaemia New patient –Height, Body weight Should compare with age –History FHx, Transfusion Hx (from when, how many times, where?, regular or irregular Hemoglobin typing result? Transfusion effect? –Review of System Fatigue, Bone change, DOE, Skin color –Physical Examination Heart sound, Lung sound, Abdominal Examination

33
Thalassaemia Determining Regular Transfusion –Should determine carefully Patients are poor, Blood bank is poor –Check patient’s record safely Check the records of Bwt, Ht. –Is it increasing? Check the records of Blood tests –Is the Hb dropping? Check the records of P/Ex –Is the spleen getting bigger?

34
Transfusion Global GuidelineLaos High Transfusion (Pretransfusion Hb > 10) Low Transfusion (Pretransfusion Hb > 7) Start transfusion -Hb<7 two times or, -Failure of Development or, -Bone change or, -Complications Start transfusion -Hb<7 two times and, -Failure of Development and, -Bone change and, -Complications ** Unless more than 2 reasons
 Low Transfusion (Pretransfusion Hb > 7) Start transfusion -Hb<7 two times or, -Failure of Development or, -Bone change or, -Complications Start transfusion -Hb<7 two times and, -Failure of Development and, -Bone change and, -Complications ** Unless more than 2 reasons")
35
Follow up patient Check Height Body weight –Please compare it with the past Check complications –Especially the compare the size of spleen Check Transfusion Hx –How many times, Follow up interval Check Ferritin Hx –If transfused over 20 times should check –If checked more than 6~12 months should check again Hb –If on Regular transfusion Hb should be over 7 If Hb over 9 prolong the follow up interval 1 more week If Hb under 7 reduce the follow up interval –If Iron overload state, the transfusion effect decreases –If Hypersplenism state, the transfusion effect decreases Check WBC, PLT –If on L-one(Deferiprone) Check if Leukopenia (Neu<1,000) –Neutrophil count = WBC X granulocyte(%) –If Postsplenectomy Check if Thrombocytosis (PLT>1,000,000)
 Check if Leukopenia (Neu<1,000) –Neutrophil count = WBC X granulocyte(%) –If Postsplenectomy Check if Thrombocytosis (PLT>1,000,000)")
36
Iron Overload If Transfusion over 20 times –Should Check Ferritin L-one (Deferiprone) –Nausea / Joint pain / Leukopenia Nausea – reduce dose Joint pain – stop for 1~2weeks with NSAID Leukopenia – stop for 2 weeks and follow up WBC Desferal (Deferroxamine) –Allergic reaction / Slow Growth –SC injection FerritinDose Ferritin > 1,000L-one 50mg/kg Ferritin > 2,000L-one 75mg/kg Ferritin > 3,000L-one + Desferal
 –Nausea / Joint pain / Leukopenia Nausea – reduce dose Joint pain – stop for 1~2weeks with NSAID Leukopenia – stop for 2 weeks and follow up WBC Desferal (Deferroxamine) –Allergic reaction / Slow Growth –SC injection FerritinDose Ferritin > 1,000L-one 50mg/kg Ferritin > 2,000L-one 75mg/kg Ferritin > 3,000L-one + Desferal")
37
Splenectomy Indication 1)The requirement of transfusion is more than 220 ml PRC/kg/year (if Hct of PR C is 75%) 2) The pretansfusion Hb cannot be controlled over 7 even though 2~3 week interval regular transfusion 3) The patient who has hypersplenism lives in a remote area where regular transfusi on access is impossible 4) Severe complication (Pancytopenia, Pain and Tenderness)
The requirement of transfusion is more than 220 ml PRC/kg/year (if Hct of PR C is 75%) 2) The pretansfusion Hb cannot be controlled over 7 even though 2~3 week interval regular transfusion 3) The patient who has hypersplenism lives in a remote area where regular transfusi on access is impossible 4) Severe complication (Pancytopenia, Pain and Tenderness)")
38
Splenectomy Preparation –Work up CBC/Blood Chemi/Electro/PT.aPTT/BT.CT/RUA CXR Cardiac echo / Abd echo HBV profile / HIV –Pre-op Vaccination (Hib, Pneumo23, Meningo) –2 weeks before operation is recommended Transfusion –Need only 1 or 2 times of transfusion before operation –Target Hb>7 at operation day
 –2 weeks before operation is recommended Transfusion –Need only 1 or 2 times of transfusion before operation –Target Hb>7 at operation day")
39
Splenectomy Post-splenectomy –Daily dressing > Antibiotics –Ambulation –Prophylaxis antibiotics Penicillin V 200,000 Unit 2 times a day –Follow up 4 weeks after operation

40
HHA Support in Clinic Regular support to patients –2250 USD / 3 months –Around 40 patients –Budget executed by Ns KinKaeSoun (HY Byoun) Temporary support –1,000,000 kip / month –Can be executed by Laotian Dr –Consult to Ns KinKaeSoun Filter –If having complication of Transfusion support 2 pieces a time
 Temporary support –1,000,000 kip / month –Can be executed by Laotian Dr –Consult to Ns KinKaeSoun Filter –If having complication of Transfusion support 2 pieces a time")
Similar presentations








 Korean J Hematol 46: 41-44 Microcytic.>")









. Red blood cells contain hemoglobin, an iron-rich.>")




 Hb is found in RBCs its main function is to transport O2 to tissues. Structure: 2 parts : heme + globin Globin: four chains. Heme: porphyrin.>")