Download presentation
Presentation is loading. Please wait.

1
Liver Functions and Abnormalities
ALT, AST, AP Bilirubin - Direct and Indirect, PT, INR, Albumin, GGT Viral Hepatitis profile, ANA , SMA, AMA , Globulins , Ammonia, Ferritin, Transferrin saturation ,Iron profile , Ceruloplasmin, Alfa –Fetoprotein , Alpha 1 Antitrypsin Plain abdomen , U/S, CT, MRI,MRCP, ERCP Liver biopsy

2
ALT, AST, Bilirubin, AP Becoming “Routine “
Screening for Liver disease (not liver function) Useful , non invasive Assess severity Predominant Hepatocellular and Cholestatic. Follow up liver disease Evaluate response to treatment . May predict outcome Drawbacks: Lack sensitivity(Normal results in liver disease (NAFLD , HCC or Cirrhosis ) Not specific for liver disease (elevated in heart or muscle injury …) They don’t lead to a specific diagnosis… we need to repeat them with a battery of other tests
 Useful , non invasive. Assess severity. Predominant Hepatocellular and Cholestatic. Follow up liver disease. Evaluate response to treatment . May predict outcome. Drawbacks: Lack sensitivity(Normal results in liver disease (NAFLD , HCC or Cirrhosis ) Not specific for liver disease (elevated in heart or muscle injury …) They don’t lead to a specific diagnosis… we need to repeat them with a battery of other tests.")
3
Abnormal Liver Function Tests !! ( ALT, AST & AP )
“ LFTs “Doesn’t measure Liver Fxn but “ screen” for liver disease Normal results in Liver disease !! Abnormal results in healthy liver !! 9 % Asymptomatic patients have mildly elevated AST or ALT In ~ 30 % will be normal by just repeating it The higher the BMI, weight and visceral obesity the more abnormal In most cases an underlying serious liver disease is Unlikely Patients with abnormal Transferase subjected to Liver biopsy : (~ 84 % Steatosis , Steatohepatitis , ~ 6 % Fibrosis and Cirrhosis and ~ 10 % normal liver histology ) Currently in the US : Commonest causes : NAFLD , Alcoholic Liver disease and Chronic Hepatitis C .
 Currently in the US : Commonest causes : NAFLD , Alcoholic Liver disease and Chronic Hepatitis C .")
4
Alanine and Aspartate Transaminase
Aminotransferases Alanine and Aspartate Transaminase (ALT ) & (AST ) Intra Cellular Enzymes in the hepatocytes Involved in amino acid metabolism . Released into circulation when the hepatocytes are injured ALT : Primarily found in the liver but in small amount in skeletal muscles . AST : Not only found in the liver but also in the cardiac muscle, skeletal muscle, kidneys, brain, pancreas, lungs… ALT & AST elevation is non specific , the exception is when AST/ALT ratio is more than 2 suggesting alcoholic liver disease …because pyridoxal-5'-phosphate ( the active form of pyridoxine = Vit B6 ) is needed for ALT synthesis but is less essential for AST synthesis , this is deficient in chronic alcoholics . This deficiency also explains why in alcoholic patients , ALT & AST elevation are not that high (< 300 IU/L)
 & (AST ) Intra Cellular Enzymes in the hepatocytes Involved in amino acid metabolism . Released into circulation when the hepatocytes are injured. ALT : Primarily found in the liver but in small amount in skeletal muscles . AST : Not only found in the liver but also in the cardiac muscle, skeletal muscle, kidneys, brain, pancreas, lungs… ALT & AST elevation is non specific , the exception is when AST/ALT ratio is more than 2 suggesting alcoholic liver disease …because pyridoxal-5 -phosphate ( the active form of pyridoxine = Vit B6 ) is needed for ALT synthesis but is less essential for AST synthesis , this is deficient in chronic alcoholics . This deficiency also explains why in alcoholic patients , ALT & AST elevation are not that high (< 300 IU/L)")
5
Elevated Transaminases … What next ?
History: Medications, OTC, Alcohol, Herbs Duration and trend Ask about IVDU, Blood transfusion, Tattoo’s , Travel Hx and alcohol F Hx: Hemochromatosis, PBC, Wilson’s and Alpha One Anti Trypsin Symptoms : ( Jaundice , fever, weight loss, pruritus, arthralgia, rash, abdominal / RUQ pain ) Steatorrhea, Loose fatty stools with cholestasis Physical exam : RUQ Tenderness and Murphy’s sign. Hepatomegaly, Splenomegaly Jaundice, muscle wasting , spider angioma, palmer erythema, gynecomastia, Ascites , pleural effusion Duputryn’s contracture, parotid swelling, Lab: ? Hepatocellular or Cholestatic ??
 Steatorrhea, Loose fatty stools with cholestasis. Physical exam : RUQ Tenderness and Murphy’s sign. Hepatomegaly, Splenomegaly. Jaundice, muscle wasting , spider angioma, palmer erythema, gynecomastia, Ascites , pleural effusion. Duputryn’s contracture, parotid swelling, Lab: Hepatocellular or Cholestatic")
6
Hepatocellular or Cholestatic
Predominant ALT & AST: ALT & AST are released into circulation when hepatocytes are injured …If predominant …Think Hepatocellular … Hepatitis Profile, ANA , SMA, SPEP , AMA , Iron Transferrin saturation and Serum Ferritin... U/S for Fatty Liver … Predominant AP : AP is released into the blood stream when there is obstruction to bile flow …Check GGT = Liver source Cholestatic “ interference with bile flow ” Extra Hepatic ? or Intra Hepatic ? ?

7
Hepatocellular : Predominant ALT & AST
1. NAFLD : Steatosis ( NAFL ) and Steatohepatitis (NASH) : -> Imaging 2. Alcoholic Liver Disease suggested by AST/ALT ratio > 2 or > 3 , Elevated GGT in those patients also suggests alcohol abuse . 3. Chronic Hepatitis C and B ( ~ 85 % of acute HCV Chronic Hepatitis ) Hemochromatosis : Iron panel, Transferrin saturation -> Biopsy Medications: Including OTC & Tylenol (Statins ,NSAIDs, Abx , Anti Seizure, Anti TB , HIV, MTX, AZA, Amiodarone , Methyldopa , Nitrofurantin, PTU Captopril … ) Herbs …. A I H : Young Females with “hepatitis” ANA, SMA, SPEP, Globulin Biopsy Alpha One Anti Trypsin Deficiency : Young, Emphysema PBC : Middle age Female with pruritis , Very high AP … AMA Liver biopsy Wilson’s : Young , Low Ceruloplasmin, Kayser Fleisher rings , 24 hour urinary cupper
 and Steatohepatitis (NASH) : -> Imaging. 2. Alcoholic Liver Disease suggested by AST/ALT ratio > 2 or > 3 , Elevated GGT in those patients also suggests alcohol abuse . 3. Chronic Hepatitis C and B ( ~ 85 % of acute HCV Chronic Hepatitis ) Hemochromatosis : Iron panel, Transferrin saturation -> Biopsy. Medications: Including OTC & Tylenol (Statins ,NSAIDs, Abx , Anti Seizure, Anti TB , HIV, MTX, AZA, Amiodarone , Methyldopa , Nitrofurantin, PTU Captopril … ) Herbs …. A I H : Young Females with hepatitis ANA, SMA, SPEP, Globulin Biopsy. Alpha One Anti Trypsin Deficiency : Young, Emphysema. PBC : Middle age Female with pruritis , Very high AP … AMA Liver biopsy. Wilson’s : Young , Low Ceruloplasmin, Kayser Fleisher rings , 24 hour urinary cupper.")
8
Cholestasis : Predominant AP Check for Obstruction by U/S ( or CT)
“ interference with bile flow Check for Obstruction by U/S ( or CT) U/S : if shows Dilated Bile Ducts = (Extra hepatic Cholestasis ) MRCP ( Choledocolithiasis “ most common “ , Malignant disease of the pancreas, GB, CBD, or of the ampulla , Chronic pancreatitis causing CBD stricter, PSC Primary Sclerosing Cholangitis (intra and extra hepatic in 2/3 cases )… look for IBD ) … ERCP. U/S does NOT show bile duct obstruction (Intra Hepatic Cholestasis) ( PBC, PSC, Drug induced Cholestasis ) for PBC check AMA , if positive AMA LIVER BIOPSY to confirm If negative U/S and negative AMA …check for PSC ( Primary Sclerosing Cholangitis by MRCP (~ 1/3 intra hepatic ) Drug induced Cholestasis: ( Phenothiazine's, Tricyclic's, Bactrim, Ampicillin, Dicloxacillin, Augmentin, Erythromycins …Androgens , Estrogens ) usually this is reversible
 U/S : if shows Dilated Bile Ducts. = (Extra hepatic Cholestasis ) MRCP. ( Choledocolithiasis most common , Malignant disease of the pancreas, GB, CBD, or of the ampulla , Chronic pancreatitis causing CBD stricter, PSC Primary Sclerosing Cholangitis (intra and extra hepatic in 2/3 cases )… look for IBD ) … ERCP. U/S does NOT show bile duct obstruction. (Intra Hepatic Cholestasis) ( PBC, PSC, Drug induced Cholestasis ) for PBC check AMA , if positive AMA LIVER BIOPSY to confirm. If negative U/S and negative AMA …check for PSC ( Primary Sclerosing Cholangitis by MRCP (~ 1/3 intra hepatic ) Drug induced Cholestasis: ( Phenothiazine s, Tricyclic s, Bactrim, Ampicillin, Dicloxacillin, Augmentin, Erythromycins …Androgens , Estrogens ) usually this is reversible.")
10
Alkaline Phosphatase Sources: (liver, bone, placenta and kidney)
A P Fractionation GGT ( γ - Glutamyl Transpeptidase) ~ liver specific High levels of AP > four fold the normal ~ 500 usually seen in prolonged Cholestasis in most cases. Elevated In extra and intrahepatic obstruction , the extent does not differentiate between either, does can not help identify etiology (CBD stone or stricture, Ca, PSC , Drug-induced hepatitis , PBC ) Modest increases in AP ~ Three times the normal ~ 350 are nonspecific and may occur in any liver disorders (acute viral hepatitis, chronic hepatitis, cirrhosis, infiltrative liver diseases and CHF) Isolated AP elevation or disproportionate elevation of AP to AST, ALT (Obstructed Bile duct 2 to Gall stones or tumor, Infiltrative diseases e.g. Sarcoidosis, TB, Mets… ) High GGT :In alcoholics even with normal Transaminases and Bilirubin , The possible explanation is the induction of hepatic microsomal GGT by alcohol , also alcohol may cause leakage of GGT from hepatocytes.
 ~ liver specific. High levels of AP > four fold the normal ~ 500 usually seen in prolonged Cholestasis in most cases. Elevated In extra and intrahepatic obstruction , the extent does not differentiate between either, does can not help identify etiology (CBD stone or stricture, Ca, PSC , Drug-induced hepatitis , PBC ) Modest increases in AP ~ Three times the normal ~ 350 are nonspecific and may occur in any liver disorders (acute viral hepatitis, chronic hepatitis, cirrhosis, infiltrative liver diseases and CHF) Isolated AP elevation or disproportionate elevation of AP to AST, ALT (Obstructed Bile duct 2 to Gall stones or tumor, Infiltrative diseases e.g. Sarcoidosis, TB, Mets… ) High GGT :In alcoholics even with normal Transaminases and Bilirubin , The possible explanation is the induction of hepatic microsomal GGT by alcohol , also alcohol may cause leakage of GGT from hepatocytes.")
11
Albumin and PT reflects the Synthetic Capacity Of Liver
Albumin: Synthesized by hepatocytes , has a Long half life ~ 20 days, 4 % degraded daily , therefore …slow turnover Albumin is not good indicator of acute or mild disease Normal Albumin = Acute process (Viral Hepatitis) Gall stone Obstruction Low Albumin = Chronic process (Cirrhosis ) PT: measures factors II, V, VII, and X , Made almost exclusively in the liver short half life , rapid turnover , good indicator of liver synthetic function. Increased PT = * Vitamin K deficiency (prolonged jaundice or malabsorption ) or * end stage liver failure if does not correct with Parenteral Vit K = Severe liver dysfunction .
 Gall stone Obstruction. Low Albumin = Chronic process (Cirrhosis ) PT: measures factors II, V, VII, and X , Made almost exclusively in the liver short half life , rapid turnover , good indicator of liver synthetic function. Increased PT = * Vitamin K deficiency (prolonged jaundice or malabsorption ) or. * end stage liver failure if does not correct with Parenteral Vit K = Severe liver dysfunction .")
12
Hematologists are trying “ Non invasive markers “ for Fibrosis
Fibro test and Fibro Sure : Predicts Chronic Liver Inflammation or Fibrosis in NAFLD ( Alpha 2 Macroglobulin, Alpha 2 Globulin (Haptoglobin), Gamma Globulin, Apo lipoprotein A1, Gamma Glutamyl Transferase and Bilirubin ) NAFLD Fibrosis Score Calculator : Age, BMI, PLT, Hyperglycemia, Albumin, AST/ALT ratio Hepascore Predictor of Liver Fibrosis In Chronic Hepatitis C (Bilirubin , GGT, Hyaluronic Acid, Alfa 2 Macroglobulin, Age & Gender ) “ NAFLD Fibrosis Score is a clinically useful tool for identifying NAFLD patients with higher likelihood of having bridging fibrosis and/or cirrhosis. “ (Strength – 1, Evidence - B)
, Gamma Globulin, Apo lipoprotein A1, Gamma Glutamyl Transferase and Bilirubin ) NAFLD Fibrosis Score Calculator : Age, BMI, PLT, Hyperglycemia, Albumin, AST/ALT ratio. Hepascore. Predictor of Liver Fibrosis In Chronic Hepatitis C. (Bilirubin , GGT, Hyaluronic Acid, Alfa 2 Macroglobulin, Age & Gender ) NAFLD Fibrosis Score is a clinically useful tool for identifying NAFLD patients with higher likelihood of having bridging fibrosis and/or cirrhosis. (Strength – 1, Evidence - B)")
13
Hyperbilirubinemia Bilirubin Unconjugated and conjugated
Isolated Unconjugated Hyperbilirubinemia Other liver functions are normal Increased Production : Hemolysis: ( Increased Reticulocytes and Haptoglobin ) Impaired Uptake: Meds …Rifampicin . Impaired conjugation : Gilbert's & the rare Criggler Najjar Isolated Conjugated Hyperbilirubinemia ( Decrease execration into the bile duct or defective liver storage ) Rare Dubin Johnson and Rotor Syndrome
 Impaired Uptake: Meds …Rifampicin . Impaired conjugation : Gilbert s & the rare Criggler Najjar. Isolated Conjugated Hyperbilirubinemia. ( Decrease execration into the bile duct or defective liver storage ) Rare Dubin Johnson and Rotor Syndrome.")
14
Hyperbilirubinemia Unconjugated and conjugated
Balance between production, conjugation and excretion In Liver Diseases ( both fractions are elevated ) Conjugated ( Direct) Hyperbilirubinemia Hepatocellular and Cholestatic ( Liver Or Biliary Disease ) Unconjugated ( Indirect) Hyperbilirubinemia Hemolytic Diseases
 Conjugated ( Direct) Hyperbilirubinemia. Hepatocellular and Cholestatic. ( Liver Or Biliary Disease ) Unconjugated ( Indirect) Hyperbilirubinemia. Hemolytic Diseases.")
15
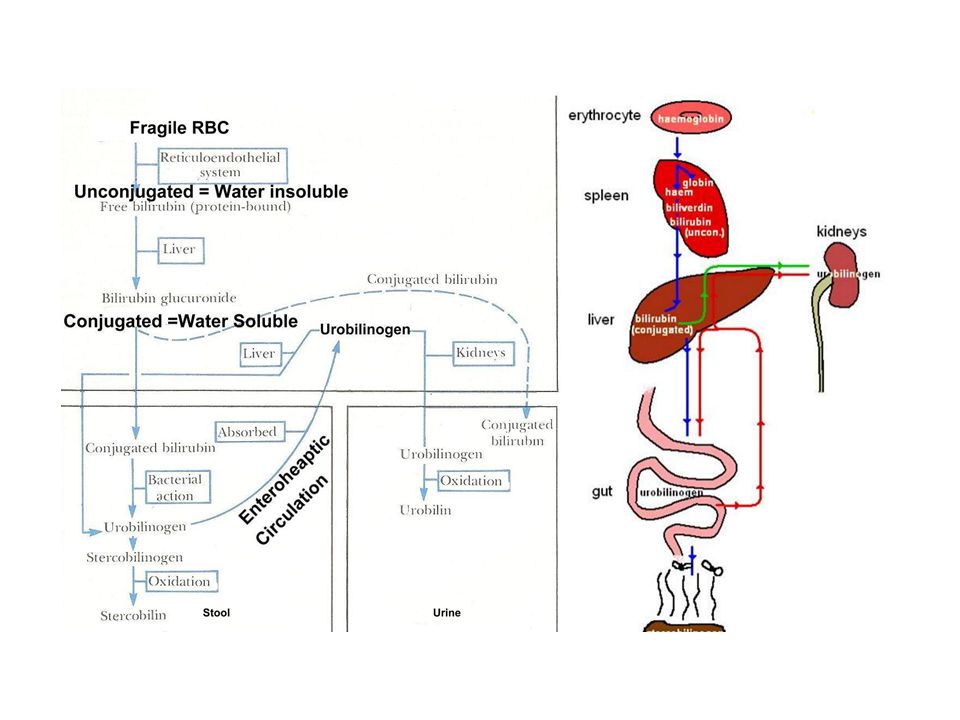
Bilirubin Metabolism RBC dies Hemo globin …bound to Haptoglobin …Transported to RES (Globin, iron, and Heme ) Heme oxidized to Biliverdin converted to Unconjugated Bilirubin (Water insoluble ) tightly bound to albumin cannot be execrated transported to liver , conjugated by Glucoronyl Transferase to Glucuronic acid (Conjugated Bilirubin is water soluble ) stored in Gall Bladder eventually excreted into the duodenum and passes into the large intestine, Bacteria converts it to Urobilinogen , oxidized to Urobilin and Stercobilin …which gives feces its brownish color. 95% of the Conjugated Bilirubin reabsorbed from small intestine (Enterohepatic Circulation) Re-secreted into the liver and into the small intestine again Some of the Urobilinogen is reabsorbed and 95% of this reabsorbed is re-secreted in the bile (part of Entero hepatic circulation )
 tightly bound to albumin cannot be execrated transported to liver , conjugated by Glucoronyl Transferase to Glucuronic acid (Conjugated Bilirubin is water soluble ) stored in Gall Bladder eventually excreted into the duodenum and passes into the large intestine, Bacteria converts it to Urobilinogen , oxidized to Urobilin and Stercobilin …which gives feces its brownish color. 95% of the Conjugated Bilirubin reabsorbed from small intestine (Enterohepatic Circulation) Re-secreted into the liver and into the small intestine again. Some of the Urobilinogen is reabsorbed and 95% of this reabsorbed is re-secreted in the bile (part of Entero hepatic circulation )")
17
About 5% of the reabsorbed urobilinogen is excreted in urine following further oxidation to Urobilin which gives urine its characteristic yellow color. Urine Bilirubin : All Bilirubin in urine is conjugated( water soluble ) urine Bilirubin means (liver disease or blocked Bile ducts ) because there is increased serum Bilirubin , some of this conjugated Bilirubin will leak out of hepatocyte and show in urine and gives it’s dark amber color The Unconjugated Bilirubin is water insoluble , bound to albumin , and not execrated in urine ( except in severe renal disease ) Urine Urobilinogen : In hemolytic anemia -> excessive RBC‘s broken down increased Unconjugated Bilirubin (Not water soluble) therefore no increase in Urine Bilirubin . Because there is no problem with the liver or Biliary tract , the excess conjugated Bilirubin is excreted into bile -> metabolized to urobilinogen … Reabsorbed Increase in urine urobilinogen. Other causes of Urine Urobilinogen: ( liver diseases, hepatitis, cirrhosis, Mets )
 urine Bilirubin means (liver disease or blocked Bile ducts ) because there is increased serum Bilirubin , some of this conjugated Bilirubin will leak out of hepatocyte and show in urine and gives it’s dark amber color. The Unconjugated Bilirubin is water insoluble , bound to albumin , and not execrated in urine ( except in severe renal disease ) Urine Urobilinogen : In hemolytic anemia -> excessive RBC‘s broken down increased Unconjugated Bilirubin (Not water soluble) therefore no increase in Urine Bilirubin . Because there is no problem with the liver or Biliary tract , the excess conjugated Bilirubin is excreted into bile -> metabolized to urobilinogen … Reabsorbed Increase in urine urobilinogen. Other causes of Urine Urobilinogen: ( liver diseases, hepatitis, cirrhosis, Mets )")
18
Non Hepatic Causes of Elevated AST or ALT
AST and ALT are also increased in Non-liver disease (Myositis, Muscle Trauma , Heavy exercise , M I , Myocarditis, Pulmonary infarction, Thyroid disorders ,Celiac disease , Adrenal insufficiency Dermatomyositis, Anorexia Nervosa , Seizure disorder, Hyperthermia ) If …of muscle disorder or muscle source CPK , LDH and Aldolase are increased … If …Thyroid check TSH If
 If …of muscle disorder or muscle source CPK , LDH and Aldolase are increased … If …Thyroid check TSH. If.")
19
Aminotransferase Elevation
Mild increases (< 300 IU/L) Nonspecific … NAFLD, Alcoholic liver disease , Cirrhosis, HCC, Cholestasis Modest elevations (300 to 500) Chronic liver disorders (Alcoholic Hepatitis, Biliary Obstruction and Chronic Hepatitis ) Markedly high values > 500 IU/L = Acute Necrosis or injury Acute Viral Hepatitis , Drug-induced , Ischemic Hepatitis Acute setting of AIH , Gall stone obstruction Aminotransferases can be normal in : NAFLD , Cirrhosis , Chronic Hepatitis C , HCC & Hemochromatosis…
 Nonspecific … NAFLD, Alcoholic liver disease , Cirrhosis, HCC, Cholestasis. Modest elevations. (300 to 500) Chronic liver disorders. (Alcoholic Hepatitis, Biliary Obstruction and Chronic Hepatitis ) Markedly high values > 500 IU/L = Acute Necrosis or injury. Acute Viral Hepatitis , Drug-induced , Ischemic Hepatitis. Acute setting of AIH , Gall stone obstruction. Aminotransferases can be normal in : NAFLD , Cirrhosis , Chronic Hepatitis C , HCC & Hemochromatosis…")
20
Aminotransferases Acetaminophen & Toxins: Rises Rapidly to > 2000 Acute Viral Hepatitis : Rises Gradually to ~2000 A I H : Rises Gradually to ~ 1000 CBD stone / Obstruction : Rapidly rise ~ 1000 Alcoholism AST > ALT : Gradually ~ < 300

21
If the patient is asymptomatic with chronically mildly elevated ALT & AST < 100 , and with Negative Viral Hepatitis, Negative Auto Immune and other metabolic markers, If nothing suggests serious liver disease continued follow up is best option Liver biopsy : Persistent Aminotransferase more than double 100 …to clarify the diagnosis , in most patients No effective medical therapy

22
Maddrey's Discriminant Function Disease Specific Prognostic Score
((Alcoholic Hepatitis)) Mild < > Life Threatening (4.6 (Bilirubin in mg + ( Patient’s PT – control PT) Patients who score > 32 are at highest risk of dying with one month ( mortality as high as 30–50% ) Corticosteroid reduce mortality if ( MDF ) > 32 Acute Alcoholic injury on a background of alcoholic liver disease , may progress to decompensation , precursor of Liver cirrhosis ( Fever ~ 101 , RUQ Pain , Elevated PT , Jaundice , Leukocytosis, Elevated AST > double ALT , Elevated AP & GGT ,Bleeding , Encephalopathy … )
) Mild < > Life Threatening. (4.6 (Bilirubin in mg + ( Patient’s PT – control PT) Patients who score > 32 are at highest risk of dying with one month ( mortality as high as 30–50% ) Corticosteroid reduce mortality if ( MDF ) > 32. Acute Alcoholic injury on a background of alcoholic liver disease , may progress to decompensation , precursor of Liver cirrhosis. ( Fever ~ 101 , RUQ Pain , Elevated PT , Jaundice , Leukocytosis, Elevated AST > double ALT , Elevated AP & GGT ,Bleeding , Encephalopathy … )")
23
The higher the MELD score
(MELD Scoring ) Model for End-stage Liver Disease MELD is “ adopted by transplant centers in the US for prioritization of patients waiting for liver transplant “ MELD Scoring : “ chronic liver disease severity to predict survival “ Variables are (Bilirubin , INR , Creatinine ) MELD Score = 3.8[Ln serum Bilirubin (mg/dL)] [Ln INR] + 9.6[Ln serum Creatinine (mg/dL)] + 6.4 ( Ln is natural logarithm) The higher the MELD score The worse is the hepatic function and the higher 3-month mortality risk Score - Mortality — 71.3% 30–39 — 52.6% 20–29 — 19.6% 10–19 — 6.0% < 9 — %
 Model for End-stage Liver Disease. MELD is adopted by transplant centers in the US for prioritization of patients waiting for liver transplant MELD Scoring : chronic liver disease severity to predict survival Variables are (Bilirubin , INR , Creatinine ) MELD Score = 3.8[Ln serum Bilirubin (mg/dL)] [Ln INR] + 9.6[Ln serum Creatinine (mg/dL)] ( Ln is natural logarithm) The higher the MELD score. The worse is the hepatic function and the higher 3-month mortality risk. Score - Mortality — 71.3% 30–39 — 52.6% 20–29 — 19.6% 10–19 — 6.0% < 9 — 1.9%")
24
Child - Pugh score ( for severity of liver disease )
Child - Pugh Classification Albumin, Bilirubin, Encephalopathy , Ascites & INR or Prolonged PT Points are assigned to each variable Score Calculated. Class One : 5-6 Points , Class B :7-9 Points , Class C :

25
Ammonia Nitrogenous compound (ingested protein) enter the colon degraded by bacteria ammonia absorbed and transported via the portal vein to the liver converts to glutamine / urea and excreted. In diseased liver with Porto systemic shunt , the diseased liver does not clear ammonia, Blood ammonia increases , which enters the systemic circulation - contributes to hepatic encephalopathy. May Increase Ammonia Levels: High-protein meals , GI bleeding , Muscle wasting , CKD, UTI with a urease-producing organism , Certain drugs ( Chemo, alcohol, valproate, diuretics, barbiturates and opioids) False High Ammonia : ( Hemolysis , Sample not chilled or iced , exposure to room temperature, delayed processing )
 enter the colon degraded by bacteria ammonia absorbed and transported via the portal vein to the liver converts to glutamine / urea and excreted. In diseased liver with Porto systemic shunt , the diseased liver does not clear ammonia, Blood ammonia increases , which enters the systemic circulation - contributes to hepatic encephalopathy. May Increase Ammonia Levels: High-protein meals , GI bleeding , Muscle wasting , CKD, UTI with a urease-producing organism , Certain drugs ( Chemo, alcohol, valproate, diuretics, barbiturates and opioids) False High Ammonia : ( Hemolysis , Sample not chilled or iced , exposure to room temperature, delayed processing )")
26
Serum Alpha-Fetoprotein
AFP : Glycoprotein produced the yolk sac and liver during fetal development . AFP in fetus decreases after birth to adult levels by 12 months. Normal ( Less than 10 or 20 ng/L. ) In HCC : AFP is elevated > ( > 1000 ) Other causes of elevated AFP : Pregnancy and pure Seminoma Malignancy: Non seminoma Germ cell Tumors Testicular Cancer ,Gastric , Biliary and Pancreatic cancer Benign causes : Chronic liver disease without HCC ( Cirrhosis, Acute or Chronic Viral Hepatitis ) AFP > 500 mcg/L In patient with chronic liver disease ( Cirrhosis ) Always HCC is a concern . HCC has been diagnosed at lower AFP level . small HCC ? normal AFP U/S : Q 6 months if suspicious Contrast CT or MRCP
 In HCC : AFP is elevated > 500 ( > 1000 ) Other causes of elevated AFP : Pregnancy and pure Seminoma. Malignancy: Non seminoma Germ cell Tumors. Testicular Cancer ,Gastric , Biliary and Pancreatic cancer. Benign causes : Chronic liver disease without HCC. ( Cirrhosis, Acute or Chronic Viral Hepatitis ) AFP > 500 mcg/L In patient with chronic liver disease ( Cirrhosis ) Always HCC is a concern . HCC has been diagnosed at lower AFP level . small HCC normal AFP. U/S : Q 6 months if suspicious. Contrast CT or MRCP.")
27
Liver biopsy Indication: Undiagnosed liver abnormality /disease
Small sample obtained , useful if “ diffuse liver changes “ Provide histologic info , type and degree of liver injury and diagnosis Assess staging , prognosis and helps with mgmt. Relatively Safe 98 % , U / S Guided , bedside, local anesthesia Limitation: sample error , pathologist experience C/ I : Bleeding disorder, suspected vascular lesion… Biopsy : During surgery , Laparoscopy Transcutaneous Trans jugular IVC Hepatic Vein Liver

28
Imaging U/S : Safe, Cheap, Non invasive , provides Structural NOT Functional information . Best and most sensitive for Biliary System especially GB Initial Imaging of choice : Screening Biliary Tract Abnormality RUQ Pain :Evaluate Hepatobiliary tract and detect liver masses Initial imaging for Cholestasis : intra or extra hepatic ? Splenomegaly size Portal HTN Limitation: Obesity, Excessive Gas , Operator experience U/S : Trans Abdominal Endoscopic U/S (U/S transducer on the tip of the endoscope )
")
29
U/S : Gall Stones : Thick GB wall > 3mm Pericholecystic fluid
Impacted stone in GB neck, sludge U/S murphy’s . Obstruction : Extra hepatic dilated CBD … Diffuse disorders : Cirrhosis & Fatty liver Liver lesions: Focal lesions > One Cm + Cystic Echo Free Solid Masses : Echogenic - Abscess or Tumor (HCC or Mets )
")
30
CT: Small Liver Metastasis with iv contrast Hemangiomas
Fatty liver : Decreased Hepatic Attenuation Assess Pancreas MRI : without contrast : Images the blood vessels , ducts and hepatic tissue . Superior to CT and U/S for Dx Fatty liver ( Increased Fat Signal ) and for Hemochromatosis ,vascular abnormalities and Hemangiomas. MRCP: CBD abnormality esp. stones ERCP : Diagnose : Obstructive jaundice ,Chronic Pancreatitis , pancreatic tumor , Gallstones with dilated CBD , Bile duct tumor and suspected injury to bile ducts . Replaced by MRCP and Endoscopic U/S Invasive …Rarely performed without therapeutic intention.
 and for Hemochromatosis ,vascular abnormalities and Hemangiomas. MRCP: CBD abnormality esp. stones. ERCP : Diagnose : Obstructive jaundice ,Chronic Pancreatitis , pancreatic tumor , Gallstones with dilated CBD , Bile duct tumor and suspected injury to bile ducts . Replaced by MRCP and Endoscopic U/S. Invasive …Rarely performed without therapeutic intention.")
33
Endoscopic retrograde cholangiopancreatography
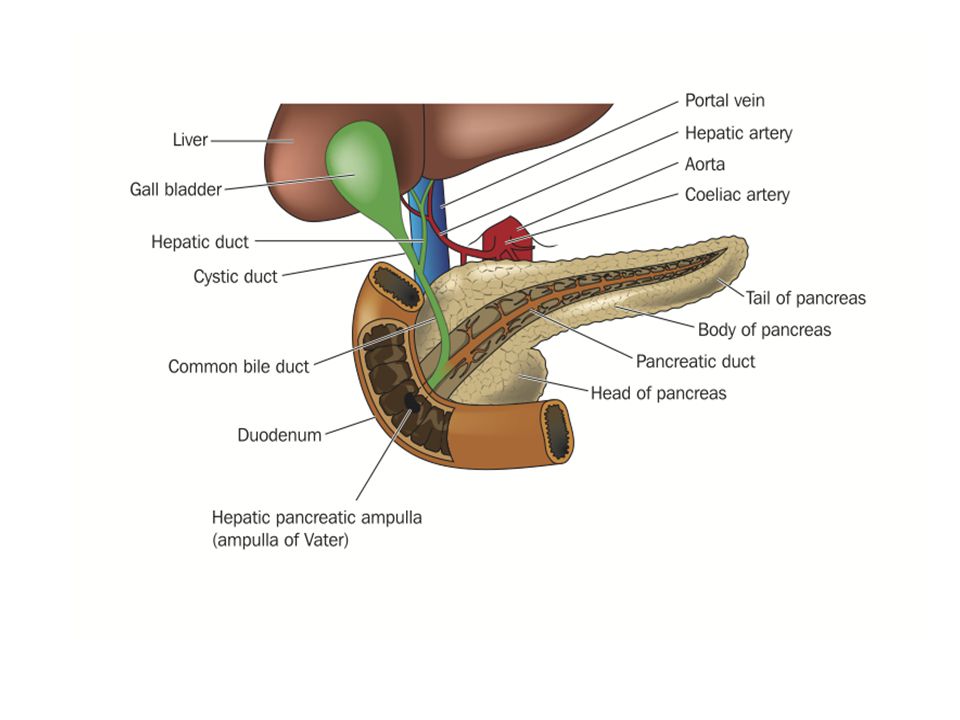
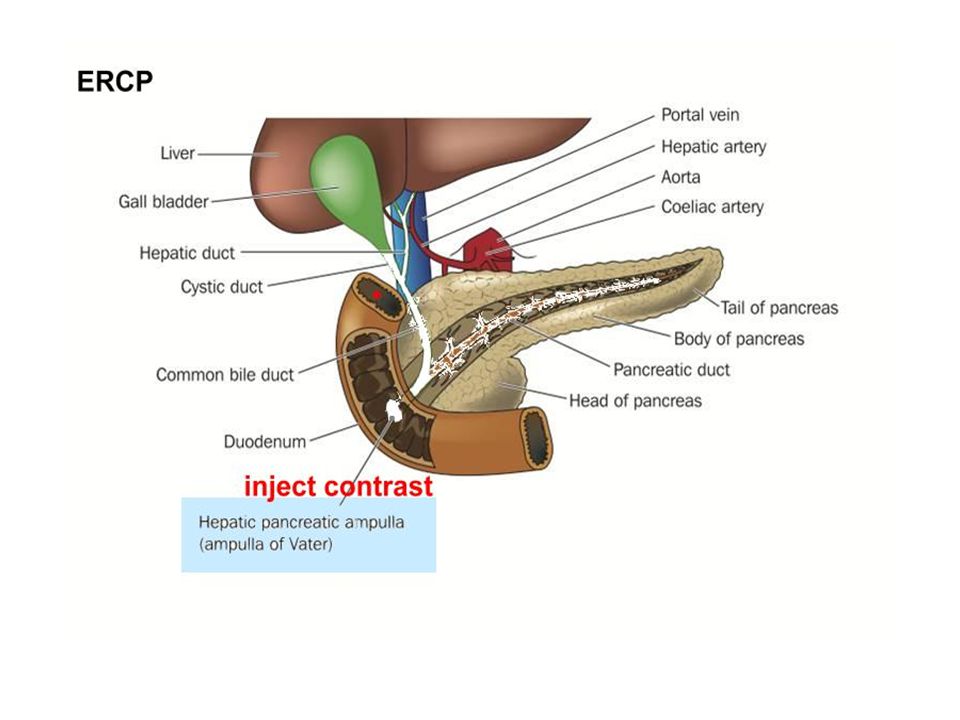
ERCP Endoscopic retrograde cholangiopancreatography Endoscopy stomach second part of duodenum …The papilla of Vater is Cannulated , contrast injected into biliary and pancreatic duct …detailed images to diagnose obstructing bile duct and pancreatic duct problems , Obstructive Gall Stones, Inflammatory Strictures , Scars , Traumatic Leakage , Ampullary Cancer and can obtain tissue biopsy . It can remove obstructing stones , dilating and /or stenting strictures PSC , and Sphictrerotomy for sphincter of oddi dysfunction Morbidity : with Diagnostic ERCP s 1% … with Sphictrerotomy up to 9 % Complication : Pancreatitis, Bleeding, Perforation, Cholangitis & Cholecystitis Pancreatitis risk is less with pancreatic stenting

Similar presentations








>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")

 that progresses to cirrhosis Replacement of liver tissue.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")






 K (3.5-5.2 mEq/L) GLU (64-128 mg/dL) BUN (7-20.>")
