Download presentation
Presentation is loading. Please wait.

1
Anemia in Chronic Kidney Disease Dr Abdullah AlHwiesh Associate Professor Consultant Internist/Nephrologist Dammam University AlKhober

2
Outline Impact of anemia in patients (CKD) Prevalence of anemia in CKD
Cardiovascular effects of anemia in CKD Target hemoglobin in CKD Erythropoietin stimulating agents (ESAs) available New anemia therapies Summary of clinical practice guidelines
 available. New anemia therapies. Summary of clinical practice guidelines.")
3
What is anemia? Diagnosis of anemia should be made
and further evaluation if: Hb < 13.5 g/dl in adult males Hb < 12 g/dl in adult females

4
Impact of anemia in CKD Symptoms Diminished quality of life
Associated with LVH

5
Impact of anemia in CKD deterioration in cardiac function decreased cognition and mental acuity. fatigue, weakness, lethargy, anorexia, and sleep disturbances.

6
Impact of anemia in CKD increased risk of morbidity and mortality
increased risk of hospitalizati mortality in patients with predialysis

7
General Population General Population Transplant Transplant Dialysis Dialysis USRDS 2006

8
AJKD 2002: 39(2)
")
9
Mortality increases exponentially as GFR declines
15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 From Any Cause (per 100 person-yr) Age Standardized Rate of Death Data from 1 million KP patients published by Go and colleagues, outlines a relationship that many of us will be familiar with. As GFR declines, all cause mortality increases > <15 Estimated GFR (ml/min/1.73 m2) Number of Events , , , , ,842 1M Kaiser Permanente patients Go et al NEJM :
 Age Standardized Rate of Death. Data from 1 million KP patients published by Go and colleagues, outlines a relationship that many of us will be familiar with. As GFR declines, all cause mortality increases. > <15. Estimated GFR (ml/min/1.73 m2) Number of Events 25,803 11,569 7,802 4,408 1,842. 1M Kaiser Permanente patients. Go et al NEJM :")
10
Adjusted Prevalence of Anemia (NHANES III)
")
11
Anemia Prevalence by CKD Stage
NHANES III NHANES Patients With Anemia* (%) CKD Stage *NHANES participants aged ≥20 y with anemia as defined by WHO criteria: hemoglobin (Hgb) <12 g/dL for women, and Hgb <13 g/dL for men.
 CKD Stage. *NHANES participants aged ≥20 y with anemia as defined by WHO criteria: hemoglobin (Hgb) <12 g/dL for women, and Hgb <13 g/dL for men.")
12
9 percent at an estimated GFR of 30 mL/min per 1.73 m2
based upon over 15,000 participants in the NHANES survey, the prevalence of anemia (Hbg <12 g/dL in men and <11 g/dL in women) 1% GFR 60 ml/min per 1.73 m2 9 percent at an estimated GFR of 30 mL/min per 1.73 m2 33 to 67 percent at an estimated GFR of 15 mL/min per 1.73 m2
 1% GFR 60 ml/min per 1.73 m2. 9 percent at an estimated GFR of 30 mL/min per 1.73 m2. 33 to 67 percent at an estimated GFR of 15 mL/min per 1.73 m2.")
14
Anemia is involved in cardiac remodeling
Reduced hemoglobin Tissue hypoxia Increased cardiac work Left ventricular hypertrophy Ischemic heart disease Worsening or precipitation of: Congestive heart failure Angina pectoris Myocardial infarction Metivier F, et al. Nephrol Dial Transplant. 2000; 15(suppl 3): 14-18
:")
19
Early versus late initiation of EPO
R,C,T early versus deferred initiation of erythropoietin in nondiabetic predialysis patients with serum creatinine 2 to 6 mg/dL and hemoglobin 9 to 11.6 g/dL. The early treatment arm was immediately started on 50 U/kg/wk of erythropoietin alpha with appropriate titration aiming for hemoglobin of ≥13 g/dL Internati onal Society of Nephrology 2006

20
The primary end point doubling of creatinine renal replacement death
Internati onal Society of Nephrology 2006

25
Clinical Benefit of Anemia Correction: CHF and CKD
Patients With CHF and Anemia (n = 126, 91% CKD) Parameter Before After Hgb (g/dL) 10.3 13.1 Serum creatinine (g/dL) 2.4 2.3 ∆GFR (mL/min/mo) -0.95 0.27 NYHA class (0-4) 3.8 2.7 Fatigue/SOB index (0-10) 8.9 Hospitalizations 3.7 0.2 Systolic BP (mm Hg) 132 131 Diastolic BP (mm Hg) 75 76 NYHA class = New York Heart Association classification; SOB = shortness of breath. Silverberg et al. Perit Dial Int. 2001;21(suppl 3):S236-S240.
 Parameter. Before. After. Hgb (g/dL) Serum creatinine (g/dL) ∆GFR (mL/min/mo) NYHA class (0-4) Fatigue/SOB index (0-10) 8.9. Hospitalizations Systolic BP (mm Hg) Diastolic BP (mm Hg) NYHA class = New York Heart Association classification; SOB = shortness of breath. Silverberg et al. Perit Dial Int. 2001;21(suppl 3):S236-S240.")
26
Prevalence of LVH increases with decreased kidney function
Levin et al. Am J Kidney Dis. 1999;34:

27
LVH is present in 74% of patients at initiation of dialysis
Foley et al. Kidney Int. 1995; 47:

30
LVH and anemia of CKD Clear association between anemia and LVH
Can correction of anemia of CKD result in LVH regression?

38
When to start ESA treatment
Anemia develops early in CKD ESA treatment: Reduces symptoms Improves quality of life May help for LVH May increase thrombotic risks and BP Decision to initiate treatment based on clinical balancing of risks and benefits

39
What is the target Hemoglobin?

40
Choir (Correction of Anemia with Epoetin Alfa in Chronic Kidney Disease)
Open label, RCT,130 centers in US, epoetin alfa SC weekly CKD (eGFR ml/min/1.73m2); Hb < 11g/dl High Hb target: 13.5 g/dl Low Hb target: 11.3 g/dl Study terminated early because conditional power poor for showing a benefit of high Hb was <5%
; Hb < 11g/dl. High Hb target: 13.5 g/dl. Low Hb target: 11.3 g/dl. Study terminated early because conditional power poor for showing a benefit of high Hb was <5%")
41
Choir Main results: 34% increased risk of composite outcome of death, MI, hospitalization for CHF, stroke (p= 0.03) No significant difference in patients requiring RRT Similar quality of life measures Singh AK et al. N Engl J Med Nov 16;355(20):
:")
42
Singh AK et al. N Engl J Med. 2006 Nov 16;355(20):2085-98
:")
43
Choir Drop out rate is high High Hb target achieved in few patients

44
Choir Singh AK et al. N Engl J Med Nov 16;355(20):
:")
45
Choir Singh AK et al. N Engl J Med Nov 16;355(20):
:")
52
CREATE Drueke TB, et al. N Engl J Med. 2006 Nov 16;355(20):2071-84
The survival without dialysis And this is the data showing the survival without dialysis. Just to point out that, again, there was in the higher hemoglobin group, a faster or greater rate of having to go on to renal replacement therapy than in the lower hemoglobin group. Drueke TB, et al. N Engl J Med Nov 16;355(20):
:")
54
ACORD Open label, RCT, 64 centers in 16 countries, N=170
Epoetin beta SC weekly Creatinine clearance > 30ml/min High Hb target: g/dl Low Hb target: g/dl after Hb < 10.5 g/dl twice or<10.0 g/dl once Ritz E et al. Am J Kidney Dis Feb;49(2):
:")
55
ACORD Main results: No significant difference in LVMI
No significant difference in decline in creatinine clearance Better QOL in high Hb group Ritz E et al. Am J Kidney Dis Feb;49(2):
:")
56
Ritz E et al. Am J Kidney Dis. 2007 Feb;49(2): 194-207
:")
57
KDOQI. Am J Kidney Dis. 2007 Sep;50(3):471-530.
Meta-analysis: Non-Dialysis CKD Patients The last new recommendation was that in dialysis and nondialysis patients with CKD receiving ESA therapy, the hemoglobin target, again, should not be greater than 13.0 g/dL. And this was termed a clinical practice guideline based upon the new moderately strong evidence showing absence of benefit and potential harm, again when hemoglobin levels are targeted to be above 13 g/dL. And again, I will emphasize the point that I just made that these guidelines are not meant to imply that there is harm to occasionally having a hemoglobin level in this range as you are targeting therapy in the range of 11 to 12 g/dL. As we sat through and pondered these potential guidelines, we asked the evidence review team which supports the DOQI process to do its own meta-analysis, and this was published as part of the supplement in the recent AJKD, and these are shown here. We separated nondialysis CKD patients shown here. Looking at relative overall mortality risk, there was no statistically significant difference in the high-hemoglobin versus the low-hemoglobin group. When the analysis was done—and the studies are shown here—looking at the relative risk of adverse cardiovascular events, there was in fact a statistically significant increase in cardiovascular events in the high-hemoglobin group or favoring control—again, assembling these various studies including CHOIR and CREATE that looked at non-dialysis-dependent CKD.

58
KDOQI. Am J Kidney Dis. 2007 Sep;50(3):471-530.
Meta-analysis: Dialysis CKD Patients Similarly, in dialysis patients shown here, same kind of meta-analysis, many fewer studies. The normal hematocrit trial with Tony Besarab was the the largest and had the largest number of patients. And there was no statistically significant difference in the combined meta-analysis of these studies.

59
(TREAT Study RDPCT 24 countries)
Treal of Darbepoetin Alfa in Type 2 Diabetes and Chronic Kidney disease (TREAT Study RDPCT 24 countries) CRF GFR 20-60ml,Dm and Anaemia 4038 2012 darpoboitin HB 13g/dl 2026 placepo Rescue if HB < 9 Death, MI,CHF,Srok,Hospitalizationfor MI NEJM2009
 CRF GFR 20-60ml,Dm and Anaemia darpoboitin. HB 13g/dl placepo. Rescue if HB < 9. Death, MI,CHF,Srok,Hospitalizationfor MI. NEJM2009.")
61
Death or cardiovascular event
602 Placepo 632 darbpoitin (hazard ratio 1.05; 95% confidence interval [CI], 0.94 to 1.17; P = 0.41). NEJM2009
. NEJM2009.")
63
Death Or ESRD 618 Palcepo 652 Darbepoetin (hazard ratio, 1.06; 95% CI, 0.95 to 1.19; P = 0.29 NEJM 2009

65
Fatal and non Fatal Strock
101 Darbepoetin 53 Placepo (hazard ratio, 1.92; 95% CI, 1.38 to 2.68; P<0.001 NEJM2009

67
The use of darbepoetin alfa in patients with diabetes, chronic kidney disease, and
moderate anemia who were not undergoing dialysis did not reduce the risk of either of the two primary composite outcomes death cardiovascular and was associated with an increased risk of stroke. NEJM 2009

68
KDOQI 2007 update In the opinion of the Work Group, selection of the Hb target and selection of the Hb level at which ESA therapy is initiated in the individual patient should include considerations of potential benefits and potential harms

69
ESA hyporesponsiveness
Definition: Hb level consistently less than 11 g/dl despite reasonable doses of ESA

71
ESAs in the treatment of anemia in Chronic Kidney Disease
Recombinant version of endogenous human EPO, first ESA approved for tx anemia in CKD (1989) Epoetin alfa Lower binding affinity for EPO receptor, but 3 times longer half life Darbepoetin alfa
 Epoetin alfa. Lower binding affinity for EPO receptor, but 3 times longer half life. Darbepoetin alfa.")
72
ESAs in the treatment of anemia in Chronic Kidney Disease
First approved chemically synthesized ESA, large molecule, prolonged duration of action CERA

73
ESAs in the treatment of anemia in Chronic Kidney Disease
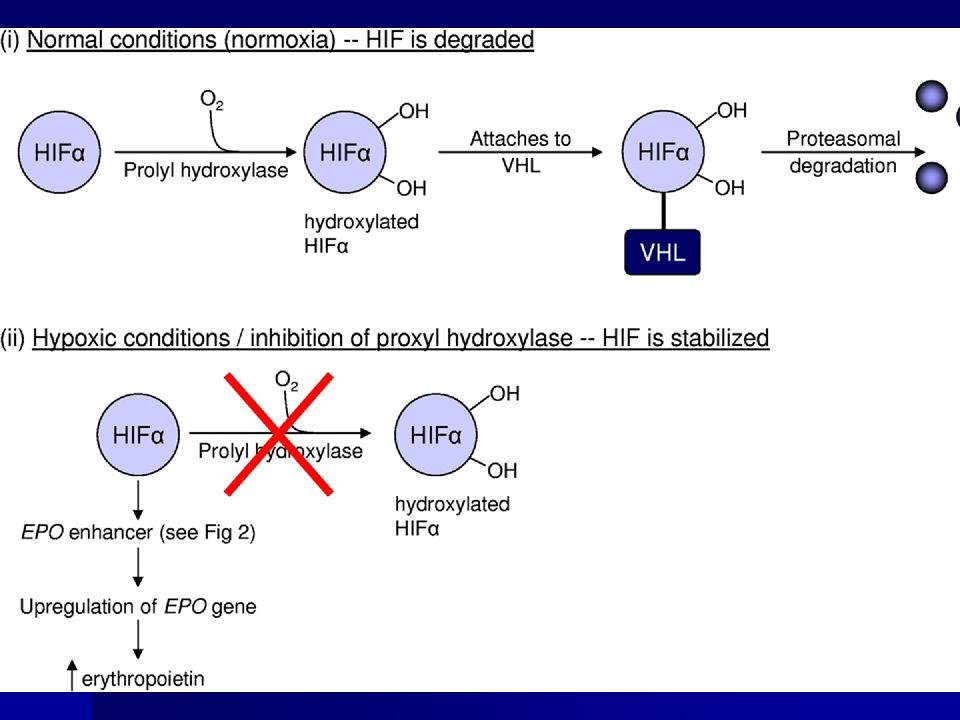
Pegylated synthetic peptide-based ESA, investigational Hematide Transcription factor, stimulates erythropoiesis and iron mobilization, investigational HIF stabilizer

74
Does half-life correlates with response?
Half-life ,h Agent 4-13 (20% longer in CRF patients) Epoetin alfa 49 (SC) Darbepoetin alfa 130 CERA 24 Hematide 10.4 HIF stabilizer
 Epoetin alfa. 49 (SC) Darbepoetin alfa CERA. 24. Hematide HIF stabilizer.")
75
PEGINESATIDE

76
a peptide could activate the erythropoietin
receptor and stimulate erythropoiesis was described first byWrighton et al15 in 1996

78
0.025-0.075 mg/kg. given once monthly

80
HIF STABILIZATION

82
1- fatal hepatic necrosis 2- up regulate VEGF (vascular endothelial growth factor), which may have potential adverse effects on enhancing tumor growth and proliferative diabetic retinopathy.
, which may have potential adverse effects on enhancing tumor growth and proliferative diabetic retinopathy.")
83
Extended dosing Extending dosing of EPO up to every 6 weeks is possible Darbepoietin and CERA have much longer half-lives

84
R,O,L,M ,16 week 37 Center 262pt <18 yr old GFR< 15-90
IU QWK 20,000 Iu Q2WK 20,000 IU Q 4WK IU Q4WK CJASN 2008

85
CJASN 2008

88
CJACN 2008

89
CJACN 2008

90
CJACN 2008

91
-0.21,0,44

92
The results of this study demonstrate that epoetin alfa can be
initiated Q4W. Although the half-life of epoetin alfa is shorter than other ESAs, it may ultimately be the life span of the red cell that determines the pharmacodynamic effect of these compounds.Therefore, epoetin alfa can provide the flexibility and convenience needed by nondialysis patients with anemia of CKD

93
Intrapatient Hb variability is not due to choice of ESA
Multicenter, randomized, double-blind study of 404 patients on HD Nissenson AR et al. ASN 2006

94
CERA and Hb Control in CKD Patients on Dialysis
Mean change in Hb levels from baseline over time Lunde NM et al. ASN 2007 (poster presentation)
")
95
Clinical practice guidelines: target hemoglobin
Better quality of life without an increase in adverse reactions are associated with Hgb >11 g/dL compared to values below this level There is also increasing evidence that there is little benefit, and even potential risk, with increased morbidity and mortality, to targeting and maintaining Hgb levels of >13 g/dL in dialysis and predialysis patients

96
Clinical practice guidelines
The 2007 DOQI update for the hemoglobin target recommends that the selected Hgb target should generally be in the range of 11 to 12 g/dL in all patients with CKD They also recommend that the Hgb target should not exceed 13 g/dL NKF-K/DOQI Clinical Practice Guidelines for Anemia of Chronic Kidney Disease. Am J Kidney Dis JASN 2007,50: 474

97
Guidelines for management of anemia in CKD
Start work up: If Hb < 11g/dl in females If Hb < 13 g/dl in males and postmenopausal females Hx and lab tests: blood loss, nutrition, adequacy of dialysis, OB, CBC, retc, iron studies, B12, folate, Hb electropheresis

98
Guidelines for management of anemia in CKD
ESA treatment is indicated if Hb <11 g/dl and no other cause of anemia EPO: 150 ug/kg/wk (SC), increase dose if given (IV) Darbepoietin: 0.45ug/kg/wk IV or SC, 0.75 ug/kg/2wks in predialysis
, increase dose if given (IV) Darbepoietin: 0.45ug/kg/wk IV or SC, 0.75 ug/kg/2wks in predialysis.")
99
Guidelines for management of anemia in CKD
Adequate response: Hb increases 1 g/dl/month Target Hb g/dl Avoid Hb > 13g/dl Monitor Hb

100
Guidelines for management of anemia in CKD
Titrate ESA dose: If Hb decrease < 1 g/dl/month, increase dose by 25-50% If Hb increases > 2-3 g/dl/month, decrease dose by 25-50% Side effects: worsening of BP control, access thrombosis

101
ESA hyporesponsiveness: iron deficiency
Iron deficiency: Tsat < 20%, S ferritin < 100 IV Iron supplement: iron sucrose or gluconate (1000 mg in 10 doses), maintain with 100mg Q 1-2 wks Monitor iron stores Do not supplement if ferritin> 800 ng/ml and/or Tsat >50%
, maintain with 100mg Q 1-2 wks. Monitor iron stores. Do not supplement if ferritin> 800 ng/ml and/or Tsat >50%")
102
Thank You

Similar presentations





































![Chronic kidney disease: [insert title here] Insert name, title, date here Insert acknowledgements here.](/12/3497998/big_thumb.jpg "Chronic kidney disease: [insert title here] Insert name, title, date here Insert acknowledgements here.>")







 Sofia Medical University. Background Erythropoiesis-stimulating agents are man-made versions of a natural protein known as erythropoietin.>")



 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")




