Download presentation
Presentation is loading. Please wait.

1
Transfusion Medicine in Emergency Medicine Scott Koepsell M.D., Ph.D. March 7, 2015 I have no conflicts of interest to disclose

2
Agenda Transfusion history/components Trauma/hemorrhage versus anemic patients Evidence based recommendations Questions/Discussion

3
Blood Bank History 1936 Chicago’s Cook County Hospital 1941 Irwin Memorial Blood Bank, SF WWII –Returning surgeons demanded blood –Initially whole blood in glass bottles, but also lyophilized plasma as well 1970s – component blood products

4
Blood Components Plasma can be manufactured into cryo

5
Blood Components: RBCs Uncrossmatched RBCs, Group O –0.4% chance of acute hemolytic reaction –2.6% chance of delayed hemolytic reaction O-positive for males and woman >50 usually ok AJCP 2010;134:202-206

6
Blood Components Plasma – AB or A –Group A plasma usually has low anti-B –Only about 10% of population is Group B or AB –Group A plasma is likely safe for all adult patients Platelets or cryoprecipitate – Any type J Trauma Acute Care Surg 2012; 74:69-75

7
Blood Components What product to give to which patients? –Trauma with bleeding –Non-trauma with bleeding –Anemia

8
Severely Injured or Trauma Patients Warm Fresh Whole Blood (WFWB) has been shown to increase survival with combat- related injuries Not really available in USA, but early administration of plasma in trauma likely lowers mortality J Trauma 2009:6(S4):S69-76 Reviewed in Hematology 2013: 656-659
 has been shown to increase survival with combat- related injuries Not really available in USA, but early administration of plasma in trauma likely lowers mortality J Trauma 2009:6(S4):S69-76 Reviewed in Hematology 2013:")
9
Severely Injured or Trauma Patients Many hospitals have adopted a massive transfusion policy that includes plasma and platelets –Subject to logistics and cost PROPPR trial showed 1:1:1 resuscitation or 1:1:2 had equivalent mortality at 24 hours and at 30 days JAMA 2015: 313(5):471-482
:")
10
Non-trauma bleeding patient 48 yo male presents to ED with coffee- ground emesis –PMH: EtOH abuse, cirrhosis –Vitals: T 37.5 P 105 R 18 BP 110/70 –PE: spider angiomata, ascites –Lab: INR 1.7, Na 130, Hgb 7.5

11
Non-trauma bleeding patient NG tube placed: blood-tinged fluid returned (~20 mL) GI consulted and on their way Would you transfuse this patient (Hgb 7.5 g/dL)?
 GI consulted and on their way Would you transfuse this patient (Hgb 7.5 g/dL)")
12
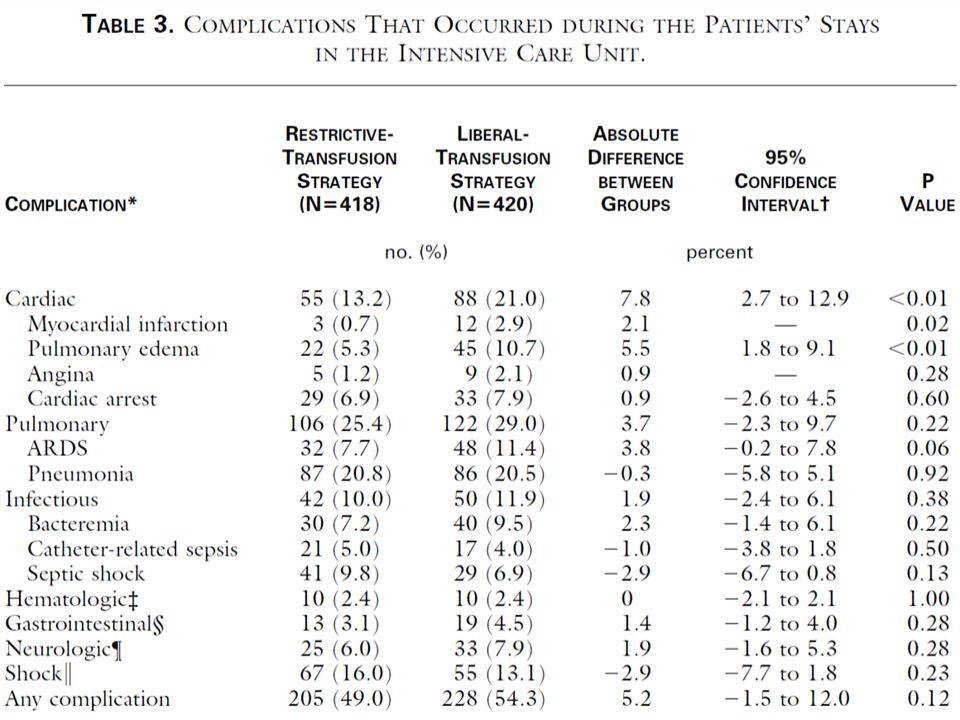
Evidence Based Transfusion Medicine Prospective, randomized trial of 921 patients with severe acute upper GI bleeding –461 Restrictive (<7 g/dL) –460 Liberal (<9 g/dL) NEJM 2013; 368: 11-21
 –460 Liberal (<9 g/dL) NEJM 2013; 368: 11-21")
13
Evidence Based Transfusion Medicine NEJM 2013; 368: 11-21

14
Evidence Based Transfusion Medicine NEJM 2013; 368: 11-21

15
Evidence Based Transfusion Medicine NEJM 2013; 368: 11-21 Major complication in the liberally transfused was further bleeding –45/444 vs 71/445, p=0.01 Hepatic hemodynamic studies showed an increased portal pressure in the transfused group

16
Non-trauma bleeding patient Not a lot of data exists, and clinical judgment that integrates laboratory and physical exam findings is key In some cases (stable upper GI bleeding), transfusion may be harmful Questions or comments?
, transfusion may be harmful Questions or comments")
17
Non-trauma patients In 1942 Dr. John Lundy “When the concentration of hemoglobin is less than 8 to 10 grams per 100 cubic centimeters of whole blood, it is wise to give a blood transfusion…” No data given for basis of recommendation

18
Blood transfusion dogma If < 10 g/dL then give 2 units –2 Unit dose of RBCs Based off hospital utilization guidelines in the mid- 20 th century Donating 1 units seems benign, so how could 1 unit transfusion help? If you are going to transfuse, then transfuse!! –Perpetuated in medical education for years –Empiric

19
Anemia, Case 1 68 year-old male presents to ED for SOB –PMH: COPD, HTN, DM, CKD, EtOH abuse –Vitals: T 38.1 P 98 BP 150/80R 20 O2 89% NC –PE: In mild distress, decreased R breath sounds & wheezing, clubbing, dry mucous membranes –Labs: WBC 13K, Hgb 9.0 g/dL, Cr 1.6 –Imaging: RLL consolidation

20
Case 1 While waiting for the patient to be admitted, would you transfuse this patient with RBCs at this point (Hgb 9.0 g/dL)? Would you transfuse this patient with RBCs if the Hgb 7.9 g/dL? Would you transfuse this patient with RBCs if the Hgb 7.0 g/dL?

21
Evidence Based Transfusion Medicine

22
Prospectively randomized 838 ICU patients –Restrictive transfusion: <7.0 g/dL Average Hgb 8.5 +/- 0.7 g/dL 2.6 +/- 4.1 RBC units transfused –Liberal transfusion: <10.0 g/dL Average Hgb 10.7 +/- 0.7 g/dL 5.6 +/- 5.3 RBC units transfused

23
NEJM: TRICC Trial

25
Evidence Based Transfusion Medicine Cochrane Reviews (2012) –19 trials involving 6264 patients Restrictive transfusion (7-8 g/dL) –Reduces risk of blood transfusion 39% –Reduces in hospital mortality (RR 0.77) –No impact on adverse events (mortality, cardiac events, myocardial infarction, stroke, pneumonia, thromboembolism)
 –19 trials involving 6264 patients Restrictive transfusion (7-8 g/dL) –Reduces risk of blood transfusion 39% –Reduces in hospital mortality (RR 0.77) –No impact on adverse events (mortality, cardiac events, myocardial infarction, stroke, pneumonia, thromboembolism)")
26
Evidence Based Transfusion Medicine 18 randomized trials involving 7593 patients –Restrictive transfusion (7-8 g/dL) Reduces risk of health care-associated infections (RR 0.82) with NNT 38 –Restrictive transfusion (<7 g/dL) Reduces risk of health care-associated infections (RR 0.80) with NNT: 20 –Most pronounced in patients presenting with sepsis JAMA 2014; 311:1317-1326
 Reduces risk of health care-associated infections (RR 0.82) with NNT 38 –Restrictive transfusion (<7 g/dL) Reduces risk of health care-associated infections (RR 0.80) with NNT: 20 –Most pronounced in patients presenting with sepsis JAMA 2014; 311:")
27
Anemia, Case 1 Questions or comments?

28
Anemia, Case 2 72 yo female presents to ED for SOB, fatigue, weight gain –PMH: CHF, CAD, HTN, CKD, anemia of chronic disease –Vitals: T 37.1 P 80 R 18 BP 135/75 O2 94% –PE: S3, pitting edema, crackles –Labs: Heart failure peptide 800 pg/mL, Hgb 7.2 –Imaging: CXR: Cardiomegaly, Kerley lines in lungs

29
Anemia, Case 2 While waiting for admission for diuresis/treatment of CHF would you transfuse for Hgb of 7.2 g/dL?

30
Evidence Based Transfusion Medicine CCM 2001; 29: 227-234 TRICC subset analysis of patients with pre-existing heart disease

31
Evidence Based Transfusion Medicine AABB –Adhere to a restrictive transfusion strategy (7- 8 g/dL) for hospitalized, stable patients –For stable patients with pre-existing cardiovascular disease, 8 g/dL –Transfuse slowly in patients with fluid overload Ann Intern Med 2012;157:49-58
 for hospitalized, stable patients –For stable patients with pre-existing cardiovascular disease, 8 g/dL –Transfuse slowly in patients with fluid overload Ann Intern Med 2012;157:49-58")
32
Anemia, Case 2 Questions or comments?

33
Anemia, Case 3 61 yo male presents to ED with chest pain –PMH: HTN, CKD, DM, anemia of chronic disease –Vitals: T 37.5 P 95 R 18 BP 110/70 –PE: diaphoretic –Lab: elevated troponin, Cr 2.9, Hgb 8.2 –ECG: no ST-segment elevation noted

34
Anemia, Case 3 61 yo male with acute MI –Would you transfuse this patient (Hgb 8.2)? –If so, 1 or 2 units?

35
Evidence Based Transfusion Medicine JAMA 2013;173(2):132-139 Meta analysis of 10 studies –“blood transfusion was associated with a higher risk for mortality independent of baseline hemoglobin level, nadir hemoglobin level, and change in hemoglobin level during the hospital stay. Blood transfusion was also significantly associated with a higher risk for subsequent myocardial infarction (risk ratio, 2.04; 95% CI, 1.06-3.93; P=.03)”
 .")
36
Evidence Based Transfusion Medicine Am J Cardiol 2011; 108:1108-1111 CRIT Trial –45 patients with acute MI and hemoglobin <10 g/dL on admission prospectively randomized Transfuse at hgb <10 (liberal) Transfuse at hgb <8 (restrictive)
 Transfuse at hgb <8 (restrictive)")
37
Am J Cardiol 2011; 108:1108-1111

38
Anemia, Case 3 No definite guidelines exist in the setting of ACS Volume status is likely an important variable Questions or comments?

39
Risk versus Benefit of RBC transfusion Blood transfusions carry more risk than previously appreciated –Not transfusion-transmitted infections i.e. risk of TT-Hepatitis B is 1:282,000 transfusions –Not well understood Why more end-organ failure and in hospital mortality with increasing transfusions? Why more infections?

40
Storage lesion of RBCs in bag may be the reason –42-day shelf life means increases in: Free iron (supports microbial growth) Free hemoglobin (vasoconstricts) Lipid microparticles (thrombogenic) No 2,3-DPG (requires 24 hours for equilibration) Damaged RBCs (overwhelms reticuloendothelial system) Less deformable RBCs (cannot flow through microvasculature)
 Free hemoglobin (vasoconstricts) Lipid microparticles (thrombogenic) No 2,3-DPG (requires 24 hours for equilibration) Damaged RBCs (overwhelms reticuloendothelial system) Less deformable RBCs (cannot flow through microvasculature)")
41
Transfusion Threshold 7 – 8 grams/dL represents a balance –Benefit: increased oxygen carrying capacity for tissues –Risk: increased complications (infection, fluid overload, etc)
")
42
Risk versus Benefit of RBC transfusion Bottom line –Restrictive transfusion thresholds (7-8 g/dL) improve non-trauma patient outcomes (even ICU patients, or upper GI bleed, or CAD) –Many hospitals have implemented restrictive transfusion policies for years without deleterious effects –Any transfusion for a hemoglobin > 8 g/dL ought to have evidence-based rationalization documented in the medical chart The appropriate dose is almost always 1 unit unless bleeding
 improve non-trauma patient outcomes (even ICU patients, or upper GI bleed, or CAD) –Many hospitals have implemented restrictive transfusion policies for years without deleterious effects –Any transfusion for a hemoglobin > 8 g/dL ought to have evidence-based rationalization documented in the medical chart The appropriate dose is almost always 1 unit unless bleeding")
43
Change is coming…

47
Discussion?

48
Ebola virus disease Categories of patients –Patient with febrile illness Patients under investigation for EVD Unknown or unsuspected EVD –Patient without illness but high level risk –Patient with confirmed EVD In all cases, history (travel/contact) is important in risk stratification
 is important in risk stratification")
49
Ebola virus disease Healthcare works encounter highly-infectious fluids (blood, urine etc) from patients with EVD –Remain highly infectious for weeks J Appl Microbiol. 109(5): 1531-9 –Viral loads reported to be up to 10 8 per ml –Infectious dose as few as 1 to 10 virions JAMA 1997: 278,(5),399-411
: –Viral loads reported to be up to 10 8 per ml –Infectious dose as few as 1 to 10 virions JAMA 1997: 278,(5),")
50
Ebola virus disease CDC guidance on PPE (recently updated to increase protection) Treatment largely remains supportive (electrolyte replacement, IV hydration) –Experimental therapies Convalescent plasma Antivirals ZMapp
 Treatment largely remains supportive (electrolyte replacement, IV hydration) –Experimental therapies Convalescent plasma Antivirals ZMapp")
51
Ebola virus disease - CP

53
Currently, Phase I safety trial of passive immune therapy during acute EVD –Clinicaltrials.gov NCT02295501 Online Ebola information (PPE, education etc) http://www.nebraskamed.com/biocontainment -unit/ebola
 -unit/ebola")
Similar presentations






 Dr Ian Williams Greater Metro South Brisbane Medicare.>")






 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")





 presents to the Emergency Room with a 2 day history of weakness.>")



