Download presentation
Presentation is loading. Please wait.

1
Minimal Requirement for hematology
血液腫瘤科 廖浚凱 Aug 15, 2012

2
Outline Anemia Blood smear

3
Erythrocyte Development
EPO: 90% from kidney 10% from liver The hemoglobin concentration in adults has a Gaussian distribution. The mean hematocrit value for adult males is 47% (± SD 7) and that for adult females is 42% (± 5). Any individual hematocrit or hemoglobin value carries with it a likelihood of associated anemia. Thus, a hematocrit of 39% in an adult male or <35% in an adult female has only about a 25% chance of being normal.
 and that for adult females is 42% (± 5). Any individual hematocrit or hemoglobin value carries with it a likelihood of associated anemia. Thus, a hematocrit of 39% in an adult male or <35% in an adult female has only about a 25% chance of being normal.")
4
Hemoglobin Fe + protoporphyrin α2β2 ↓ ↓ heme globin ↓ Hb

5
Two main approaches for anemia that are not mutually exclusive:
1. Kinetic approach 2. Morphological approach

6
Kinetic approach of Anemia
Production? Survival/ Destruction? The key test is the …..

7
Reticulocyte Production Index— an estimate of marrow production relative to normal
Hct Corrected Ret= Ret(%) * 45 Corrected Ret RPI= Maturation index
 * 45. Corrected Ret. RPI= Maturation index.")
8
RPI (kinetic approach)
RPI are the most helpful: extremely low (<0.1%) AA/ PRCA are the first considerations extremely high (>3%) Blood loss/ hemorrhage Hemolytic anemia (although 25% AIHA have normal RPI)
 AA/ PRCA are the first considerations. extremely high (>3%) Blood loss/ hemorrhage. Hemolytic anemia (although 25% AIHA have normal RPI)")
10
Morphological Approach-1
MCV>115 Vit B12, Folate Drugs that impair DNA synthesis (AZT, chemotherapy, azathioprine) MDS MCV Ditto Reticulocytosis Hypothyroidism Alcoholism/ liver dz
 MDS. MCV Ditto. Reticulocytosis. Hypothyroidism. Alcoholism/ liver dz.")
11
Morphological Approach-2
Normocytic (MCV ) Anemia of chronic disease (ACD) Mixed deficiencies Renal failure BM dz (ex AA, MDS, MM…) Microcytic (MCV<80) Iron deficiency anemia Thalassemia Anemia of chronic disease (ACD, 30-40%) Sideroblastic anemia Pb intoxification
 Anemia of chronic disease (ACD) Mixed deficiencies. Renal failure. BM dz (ex AA, MDS, MM…) Microcytic (MCV<80) Iron deficiency anemia. Thalassemia. Anemia of chronic disease (ACD, 30-40%) Sideroblastic anemia. Pb intoxification.")
12
Iron and IDA

13
Distribution of Iron in Adults
In the balanced state, 1 to 2 mg of iron enters and leaves the body each day. Dietary iron is absorbed by duodenal enterocytes. It circulates in plasma bound to transferrin. Most of the iron in the body is incorporated into hemoglobin in erythroid precursors and mature red cells. Approximately 10 to 15 percent is present in muscle fibers (in myoglobin) and other tissues (in enzymes and cytochromes). Iron is stored in parenchymal cells of the liver and reticuloendothelial macrophages. These macrophages provide most of the usable iron by degrading hemoglobin in senescent erythrocytes and reloading ferric iron onto transferrin for delivery to cells.
 and other tissues (in enzymes and cytochromes). Iron is stored in parenchymal cells of the liver and reticuloendothelial macrophages. These macrophages provide most of the usable iron by degrading hemoglobin in senescent erythrocytes and reloading ferric iron onto transferrin for delivery to cells.")
14
Storage iron Circulating iron RBC iron Tissue iron
Figure 105-2: Laboratory studies in the evolution of iron deficiency. Measurements of marrow iron stores, serum ferritin, and total iron-binding capacity (TIBC) are sensitive to early iron-store depletion. Iron-deficient erythropoiesis is recognized from additional abnormalities in the serum iron (SI), percent transferrin saturation, the pattern of marrow sideroblasts, and the red cell protoporphyrin level. Patients with iron deficiency anemia demonstrate all the same abnormalities plus hypochromic microcytic anemia.
 are sensitive to early iron-store depletion. Iron-deficient erythropoiesis is recognized from additional abnormalities in the serum iron (SI), percent transferrin saturation, the pattern of marrow sideroblasts, and the red cell protoporphyrin level. Patients with iron deficiency anemia demonstrate all the same abnormalities plus hypochromic microcytic anemia.")
15
IDA Presentation Presentation Diagnosis Progressive MCV ↘
Progressive RBC ↘ Typically high RDW Typically high MCV/RBC Typically mild PLT ↑ Ferritin: low (N=20-300) Iron/TIBC <16% (N=~33%) BM iron stain
 Iron/TIBC <16% (N=~33%) BM iron stain.")
16
Causes of IDA Increased iron requirement Inadequate iron supply
Hypermenorrhea GI blood loss– hemorrhoid, PUD, GI cancer, angiodysplasia Factitious removal Hemolysis Hemodialysis Hookworm infestation Rapid growth of teenage Pregnancy and lactation Poor nutritional intake Malabsorption Gastrectomy (may also has Vit B12 deficiency)
")
17
Iron Supply Oral: usually 3 months to restore iron storage IV
Ferrum chewable (Fe 3+) 100mg/tab Hematonic (Fe 2+) 50mg/tab IV Atofen (!! Risk of allergy and anaphylaxis—0.6%)
 100mg/tab. Hematonic (Fe 2+) 50mg/tab. IV. Atofen (!! Risk of allergy and anaphylaxis—0.6%)")
18
Thalassemia

20
Hb Gene Harrison’s Principles of Internal Medicine 15th Ed. 2001
Figure 106-1: The globin genes. The -like genes ( , ) are encoded on chromosome 16; the -like genes ( , , , ) are encoded on chromosome 11. The and genes encode embryonic globins.
 are encoded on chromosome 16; the -like genes ( , , , ) are encoded on chromosome 11. The and genes encode embryonic globins.")
21
Thalassemia Presentation
Diagnosis Exclude IDA Hb electrophoreis: Hb A2>3.5% or HbF>2% β-thalassemia HbH(+) α-thalassemia with ¾ defect (HbH dz) HbA2 and HbF: N α-thalassemia with ¼ or 2/4 defect Gene diagnosis Constant low MCV Constant high RBC Typically low RDW Typically low MCV/RBC Typically iron storage ↗
 α-thalassemia with ¾ defect (HbH dz) HbA2 and HbF: N α-thalassemia with ¼ or 2/4 defect. Gene diagnosis. Constant low MCV. Constant high RBC. Typically low RDW. Typically low MCV/RBC. Typically iron storage ↗")
22
Gene Level of Thalassemia in Taiwan
α-thalassemia: Prevalence 4% --SEAα0 deletion -α3.7 deletion -α4.2 deletion HbQS or HbCS β-thalassemia: Prevalence 2% Codon 41/42 TCTT deletion β0 IVS II 654 C-> T point-mutation β0 Codon 17 A-> T β0 Promoter 28 A-> G β+ HbE (Codon 26 G-> A) β+ ??% α + β-thalassemia (Severity?)
 β+ % α + β-thalassemia (Severity )")
23
優生學的理由 β –Major (終身輸血) Hb H disease (黃疸) Hydrops fetalis (死胎)
 Hb H disease (黃疸) Hydrops fetalis (死胎)")
24
Thalassemia Treatment
Mild: None Severe: Folic acid RBC transfusions + iron chelators Allo-SCT

25
Megaloblastic Anemia

26
Figure 107-2: The assimilation of cobalamin
Figure 107-2: The assimilation of cobalamin. On entering the stomach, dietary cobalamin (Cbl) forms a complex with R binding protein. As this protein is digested in the small intestine, cobalamin is transferred to intrinsic factor (IF). This complex passes through the intestine until it reaches specific receptors on the mucosa of the distal ileum. The internalized Cbl is then transferred to transcobalamin II (TC II), which circulates in the plasma until it binds to receptors on cells throughout the body and is internalized.
 forms a complex with R binding protein. As this protein is digested in the small intestine, cobalamin is transferred to intrinsic factor (IF). This complex passes through the intestine until it reaches specific receptors on the mucosa of the distal ileum. The internalized Cbl is then transferred to transcobalamin II (TC II), which circulates in the plasma until it binds to receptors on cells throughout the body and is internalized.")
27
Megaloblastic Anemia Presentation
Diagnosis High high MCV Pancytopenia Hypersegmented PMN Typically high RPI, hemolysis (LDH ↗), indirect hyperbilirubinemia Tinnitus or other neurological presentation Vegetarism (奶, 蛋, 維他命) Gastrectomy or Pernicious anemia ??Schilling test Low Vit B12 or folic acid Vit B12: 270~400: empirical try Vit B12< 270: definite deficiency
, indirect hyperbilirubinemia. Tinnitus or other neurological presentation. Vegetarism (奶, 蛋, 維他命) Gastrectomy or Pernicious anemia. Schilling test. Low Vit B12 or folic acid. Vit B12: 270~400: empirical try. Vit B12< 270: definite deficiency.")
28
Remember Pancytopenia
P: PNH A: Asplatic anemia N: Neoplasm/ Near neoplasm (including MDS) C: Cirrhosis/ Connective tissue disease Y: Vit B12/ Folic acid T: Toxin/ Drug O: Overwhelming sepsis (Hemophagocytic syndrome)/ Others
 C: Cirrhosis/ Connective tissue disease. Y: Vit B12/ Folic acid. T: Toxin/ Drug. O: Overwhelming sepsis (Hemophagocytic syndrome)/ Others.")
29
Vit B12/Folate Deficiency Anemia Treatment
Vit B12 deficiency: Vit B12 1 mg im qd *5 q1wk *4 q1m*3 q6m R/I pernicious anemia (Anti-parietal Ab, anti-IF Ab and PES) Thyroid dz Gastric cancer Folate deficiency: Improved diet, folic acid
 Thyroid dz. Gastric cancer. Folate deficiency: Improved diet, folic acid.")
30
Usually rapid response Most important F/U Reticulocyte, LDH
Harrison’s Principles of Internal Medicine 15th Ed. 2001 Figure 107-3: Hematologic response of a patient with pernicious anemia to an intramuscular injection of 100 g cobalamin on day 0.

31
Hemolytic Anemia

32
Is there hemolysis? Damaged RBCs on smear Marrow response to hemolysis
spherocytes (immune hemolysis, HS) RBCs fragments (microangiopathic anemias) Marrow response to hemolysis polychromasia on smear reticulocytosis erythroid hyperplasia in marrow Biochemical evidence of RBCs destruction Indirect hyperbilirubinemia increased LDH decreased/absent haptoglobin
 RBCs fragments (microangiopathic anemias) Marrow response to hemolysis. polychromasia on smear. reticulocytosis. erythroid hyperplasia in marrow. Biochemical evidence of RBCs destruction. Indirect hyperbilirubinemia. increased LDH. decreased/absent haptoglobin.")
33
Extravascular vs Intravascular hemolysis
Extravascular Intravascular Test Hemolysis Hemolysis LD á áá bilirubin á á haptoglobin N to absent absent hemoglobinuria absent present free Hb in plasma absent present urine hemosiderin absent present

34
An approach to hemolytic anemia
Immune Non-immune Congenital Acquired Autoimmune Alloimmune Drug-induced Defects of: Membrane/ skeleton (eg. Hereditary spherocytosis) Enzymes (eg. G6PD deficiency) Hemoglobinopathy PNH Infections sepsis malaria Mechanical Prosthetic heart valve Microangiopathic HA (TTP, HUS, DIC) Hypersplenism
 Enzymes. (eg. G6PD deficiency) Hemoglobinopathy. PNH. Infections. sepsis. malaria. Mechanical. Prosthetic heart valve. Microangiopathic HA (TTP, HUS, DIC) Hypersplenism.")
35
D/D of AIHA Warm AIHA Cold AIHA
RBC’s coated with IgG, Fix complement poorly (usually C3 only) RBC’s coated with IgM which fixes complement Younger age Older age extravascular hemolysis (Spleen is primary site of destruction) Intravascular hemolysis (Liver is primary site of destruction) Spherocytes on PB smear Agglutination on PB smear 70% associated with other illnesses 90% associated with other illnesses Treatment: steroids, Splenectomy Rituximab Immunosuppressants Treatment: avoidance of cold Poor response to steroids, splenectomy Plasmapheresis in refractory cases
 RBC’s coated with IgM which fixes complement. Younger age. Older age. extravascular hemolysis. (Spleen is primary site of destruction) Intravascular hemolysis. (Liver is primary site of destruction) Spherocytes on PB smear. Agglutination on PB smear. 70% associated with other illnesses. 90% associated with other illnesses. Treatment: steroids, Splenectomy. Rituximab. Immunosuppressants. Treatment: avoidance of cold. Poor response to steroids, splenectomy. Plasmapheresis in refractory cases.")
36
D/D of ACD and IDA ACD may concurrently coexist with true iron deficiency (In this situation, iron/TIBC is more reliable than ferritin)
 .")
37
貧血 分類: 重要指標: 依血球大小及形態: 依製造功能 網狀性紅血球值〈Reticulocyte count〉 乳酸脫氫脢〈LDH〉
紅血球偏小性貧血:海洋性貧血、缺鐵性貧血、慢性疾病相關之貧血 正常紅血球大小之貧血 紅血球偏大性貧血:維他命B12缺乏或葉酸缺乏性貧血、網狀紅血球增加之貧血〈溶血急性出血〉 依製造功能 製造不足: 骨髓造血功能不足、再生不良性貧血、造血元素缺乏性貧血、缺鐵性貧血、純紅血球製造不良、其他疾病合併骨髓侵犯 紅血球生成素〈Erythropoietin〉不足:腎衰竭、內分泌失調、營養 不良、 蛋白質不足 破壞或流失增加:溶血性貧血、出血、脾臟腫大性貧血 重要指標: 網狀性紅血球值〈Reticulocyte count〉 乳酸脫氫脢〈LDH〉 膽紅素〈Bilirubin〉 血紅素結合素〈Heptoglobin〉

38
Blood smear teaching

39
Burr cells Altered lipid in cell membrane artifact Uremia gastric CA
transfused old blood

40
Elliptocytes/ovalocytes
Abnormal cytoskeletal proteins Hereditary elliptocytosis

41
Howell Jolly body Nuclear remnant - DNA hemolytic anemia
Absent or hypofunction spleen

42
Schistocyte/helmet cells
Fragmented (mechanical or phagocytosis) DIC TTP HUS Vasculitis prosthetic heart valve severe burns
 DIC. TTP. HUS. Vasculitis. prosthetic heart valve. severe burns.")
43
Sickle cells Molecular aggregation of Hgb-S SS, SC, S-thal
rarely S-trait

44
NRBC Common in newborn severe degree of hemolysis

45
Spherocyte Absent central pallor look smaller Hereditary spherocytosis
immune hemolytic anemia

46
Target cells Increased redundancy of membrane hemoglobinopathies
thalassemia liver disease

47
Tear drop cells Distorted drop shaped Smear artifact myelofibrosis
promyeloblastic leukemia space occupying lesions of marrow

48
Rouleaux formation Increased serum protein levels Multiple myeloma

49
Red cell Agglutination

50
血球成熟之變化 性質 成熟之變化 細胞 大小 大->小(megakaryoblas除外) 細胞質 量 顏色 顆粒 少->多
細胞 大小 大->小(megakaryoblas除外) 細胞質 量 顏色 顆粒 少->多 深藍->淡藍->橘紅(如RBC) 多->少或消失 細胞核 染色質 顏色 圓,卵圓->內凹,變小->分葉->消失 細->粗 紅紫->藍紫 核/質比 比例減少
 細胞質 量. 顏色. 顆粒. 少->多. 深藍->淡藍->橘紅(如RBC) 多->少或消失. 細胞核 染色質 顏色. 圓,卵圓->內凹,變小->分葉->消失. 細->粗. 紅紫->藍紫. 核/質比. 比例減少.")
51
血球染色特徵 細胞成分 顏色 核仁 染色質 紅血球 淡藍 紫色 粉紅色 網狀紅血球顆粒 芽球細胞質 血小板 灰藍色 深藍色 初級顆粒
嗜中性顆粒 嗜酸性顆粒 嗜鹼性顆粒 毒性顆粒 紅紫色 橘紅色 黑紫色 藍黑色 Auer 小體 Cabot氏環 Howell-Jolly小體 Dohl小體 鮮藍色

52
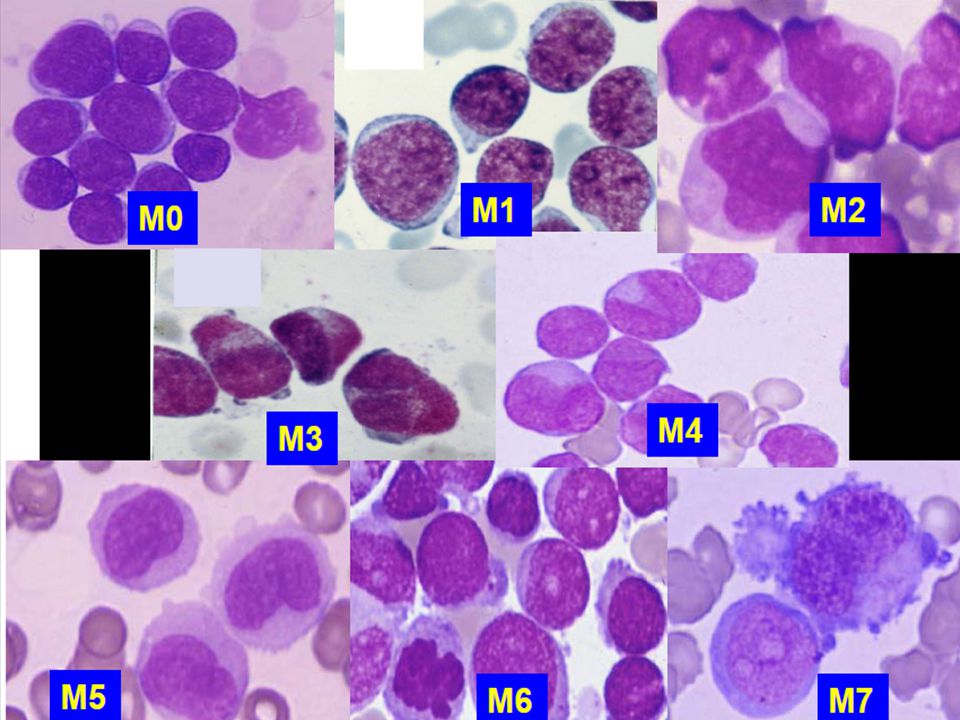
WBC series Granulocytes Monocyte Lymphocyte Neutrophil Neutrophil
Eosinophil Basophil Monocyte Lymphocyte T cell, B cell Neutrophil Blast Promyelocyte Myelocyte Metamyelocyte Band Segment

53
Granulocyte 0-5% 50-65%

56
Faggot cell Auer Rods Faggot Cells

57
Pancytopenia with macrocytic anemia
Causes megaloblastic anemia aplastic anemia acute leukemia myelodysplastic syndrome chronic liver disease (esp. liver cirrhosis) Work-up Serum VitB12 & folic acid reticulocytes bone marrow study
 Work-up. Serum VitB12 & folic acid. reticulocytes. bone marrow study.")
58
Macrocytic anemia with unmeasurable RBC
RBC & Hct : unmeasurable RBC agglutination Causes : autoimmune hemolytic anemia, mixed type or cold type Work-up peripheral blood smear serum bilirubin (T/D), AST, LDH, haptoglobin, urine analysis, reticulocytes Coombs’ test (direct and indirect) ANA, VDRL, cold hemagglutinin antibody
, AST, LDH, haptoglobin, urine analysis, reticulocytes. Coombs’ test (direct and indirect) ANA, VDRL, cold hemagglutinin antibody.")
59
有獎徵答

60
------------------------------------------------------------------------------------------------
檢驗項目 檢驗值 單位 H/L 參考值 ======================================================= WBC /CMM L M F3.5-11 RBC MILON/CMM L M F HGB g/dL L M F12-16 HCT % L M41-53 F36-46 MCV FL H MCH pg/Cell H MCHC g/dL RDW-SD % H PLATELET /CMM H RDW-CV % H SEGMENT % L LYMPHOCYTE % MONOCYTE % EOSINOPHIL % BASOPHIL %

61
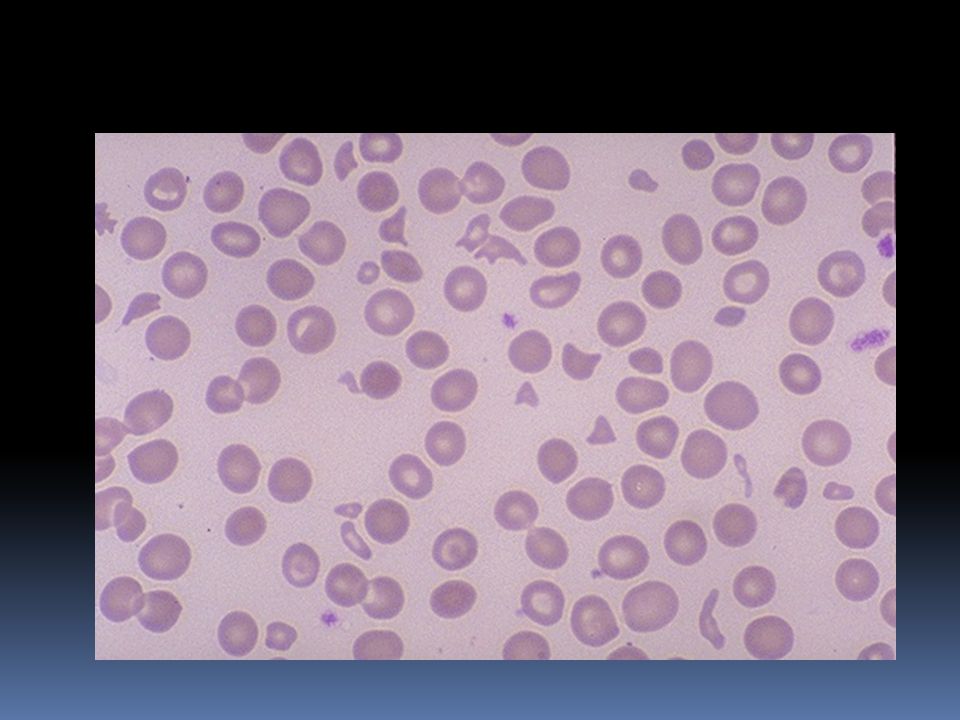
IDA

66
Leukoerythroblastosis
Immature RBC (nucleated RBC) and myeloid cells in peripheral blood Causes Bone morrow disorders: Infiltrative disorders or hematologic malignancy Peripheral disorders: Severe infection, major stress or operation, acute blood loss
 and myeloid cells in peripheral blood. Causes. Bone morrow disorders: Infiltrative disorders or hematologic malignancy. Peripheral disorders: Severe infection, major stress or operation, acute blood loss.")
67
Thrombocytosis Primary: Bone marrow disease Secondary (Reactive)
Myeloproliferative disease Secondary (Reactive) Malignancy Inflammation or infection Connective tissue disorder Blood loss or anemia Splenectomy
 Malignancy. Inflammation or infection. Connective tissue disorder. Blood loss or anemia. Splenectomy.")
68
THANKS

Similar presentations