Download presentation
Presentation is loading. Please wait.

1
Non-Suicidal Self-Injury: Description, Motivations, and Relationship to Suicide
E. David Klonsky, PhD Associate Professor Department of Psychology University of British Columbia

2
Non-Suicidal Self-Injury
Common in youth and adolescents Can be confused for attempted suicide Has an important relationship to suicide risk

3
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Relationship to Suicide

4
A Preliminary Note What we know (many many studies)
What we think (one or two studies) What we don’t know (no research yet)
 What we don’t know (no research yet)")
5
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Relationship to Suicide

6
What is Self-Injury? Self-inflicted damage to body tissue Intentional
No suicidal intent I think self-harm is a very interesting topic, is poorly understood and is often misunderstood. Important for practice, how to react to patients who self-harm. Important theoretically, why for some people does self-harm feel like a good thing to do? I think self-harm is a fascinating topic, and one that is not well understood and often misunderstood. If you look to DSM-IV, self-harm appears once, as a criterion for borderline personality disorder. Yet in most treatment settings it’s apparent that self-harm can be found in patients with a variety of diagnoses (including those with major depression, eating disorders, bipolar disorders, schizophrenia, and substance disorders). I think this discrepancy is one indication that we don’t yet know what self-harm means when we see it in our patients. We know even less about self-harmers who do not find their way into clinics. How many people in non-clinical populations self-harm? Are they all pathological? Are there some self-harmers who function quite well day to day and don’t need treatment? CASE STUDIES How many people in non-clinical populations self-harm? What are they like? (Are they all pathological?)
. I think this discrepancy is one indication that we don’t yet know what self-harm means when we see it in our patients. We know even less about self-harmers who do not find their way into clinics. How many people in non-clinical populations self-harm Are they all pathological Are there some self-harmers who function quite well day to day and don’t need treatment CASE STUDIES. How many people in non-clinical populations self-harm What are they like (Are they all pathological )")
7
What is Self-Injury? Intentional, direct injuring of one’s body tissue without suicidal intent Also called: non-suicidal self-injury (NSSI), self-mutilation, self-injurious behavior, self-wounding, and deliberate self-harm. Definition gets hazy quickly. 1) What does “deliberate” and “non-accidental” mean different things. Trichitillomania? Deliberate versus non-deliberate overdoses? Banging fist against wall (action deliberate, but harm not)? 2) What kind of damage? Damage to body tissue, vs bleeding, cutting, bruising. 3) without suicidal intent vs without apparent suicidal intent vs without consious suicidal intent
, self-mutilation, self-injurious behavior, self-wounding, and deliberate self-harm. Definition gets hazy quickly. 1) What does deliberate and non-accidental mean different things. Trichitillomania Deliberate versus non-deliberate overdoses Banging fist against wall (action deliberate, but harm not) 2) What kind of damage Damage to body tissue, vs bleeding, cutting, bruising. 3) without suicidal intent vs without apparent suicidal intent vs without consious suicidal intent.")
8
What is Self-Injury? Skin-cutting, burning, scratching, rubbing skin against rough surfaces, interfering with wound healing Does not include overdosing, eating disorder behaviors, alcohol/substance use, body piercings/tattoos* Definition gets hazy quickly. 1) What does “deliberate” and “non-accidental” mean different things. Trichitillomania? Deliberate versus non-deliberate overdoses? Banging fist against wall (action deliberate, but harm not)? 2) What kind of damage? Damage to body tissue, vs bleeding, cutting, bruising. 3) without suicidal intent vs without apparent suicidal intent vs without consious suicidal intent
 What does deliberate and non-accidental mean different things. Trichitillomania Deliberate versus non-deliberate overdoses Banging fist against wall (action deliberate, but harm not) 2) What kind of damage Damage to body tissue, vs bleeding, cutting, bruising. 3) without suicidal intent vs without apparent suicidal intent vs without consious suicidal intent.")
9
Variation in Self-Injury
Frequency Methods Medical Severity Contexts Motivations Desire/Efforts to Stop

10
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Relationship to Suicide

11
Famous Self-Injurers Princess Diana

12
Famous Self-Injurers Angelina Jolie

13
Famous Self-Injurers Christina Ricci

14
Famous Self-Injurers Drew Barrymore

15
Famous Self-Injurers Johnny Depp

16
Famous Self-Injurers Eminem

17
Famous Self-Injurers Marsha Linehan

18
Famous Self-Injurers Harry Potter’s Dobby
Klonsky, E.D. & Laptook, R. (2007). Dobby had to iron his hands, sir! Self-inflicted cuts, burns, and bruises in Harry Potter. In the Psychology of Harry Potter. BenBella Books. “Leaving out cites”
. Dobby had to iron his hands, sir! Self-inflicted cuts, burns, and. bruises in Harry Potter. In the Psychology of Harry Potter. BenBella Books. Leaving out cites")
19
Who Self-Injures? Young Adolescents 8% High-School 14 - 15%
University Students 17% General Adult Population 4-6% Adolescent Inpatients % Klonsky, E.D. & Muehlenkamp, J.J. (2007). Self-injury: A research review for the practitioner. Journal of Clinical Psychology: In Session.
. Self-injury: A research review for the practitioner. Journal of Clinical Psychology: In Session.")
20
Psychological Characteristics
Negative Emotions/Emotion Dysregulation Depression Anxiety Anger Self-Directed Negative Emotion Suicide Ideation and Attempts

21
Defining Characteristic
Intense, Self-Directed Negative Emotions?

22
What About Abuse Histories?
“may be reenacting the abuse perpetrated on them” (Noll, 2003) “manifestation of sexual abuse” (Cavanaugh, 2002) Abuse “contributes heavily to the initiation of self-destructive behaviors” (van der Kolk, 1991)
 manifestation of sexual abuse (Cavanaugh, 2002) Abuse contributes heavily to the initiation of self-destructive behaviors (van der Kolk, 1991)")
23
Child Sex Abuse and Self-Injury
Analysis of 44 studies Median phi = 0.23 (small relationship) Klonsky, E.D. & Moyer, A. (2008). Childhood sexual abuse and non-suicidal self-injury: Meta- analysis. British Journal of Psychiatry.
 Klonsky, E.D. & Moyer, A. (2008). Childhood sexual abuse and non-suicidal self-injury: Meta- analysis. British Journal of Psychiatry.")
24
Child Sex Abuse and Self-Injury: Conclusion
Abuse histories can contribute to negative emotions driving NSSI, but … … many who self-injure do not have abuse histories, and many with abuse histories do not self-injure.

25
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Relationship to Suicide

26
Why People Self-Injure: Theories
Theory Description of Theory Anti-Dissociation To end the experience of depersonalization or dissociation Anti-Suicide To replace or compromise with the impulse to commit suicide Emotion Regulation To alleviate intense negative emotions Interpersonal Boundaries To assert one’s identity or a distinction between self and other Interpersonal Influence To seek help from or manipulate others Self Punishment To derogate or express anger towards oneself Sensation Seeking To generate excitement or exhilaration Sexual To control, distract from, or gratify uncomfortable sexual urges

27
Why People Self-Injure: Research
Sources of evidence 1) Reasons/motivations for self-injury 2) Experience of self-injury 3) Laboratory studies of proxies for self-injury Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
 Reasons/motivations for self-injury. 2) Experience of self-injury. 3) Laboratory studies of proxies for self-injury. Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
28
Why People Self-Injure: Research
Theory Evidence For Theory Anti-Dissociation R, R, R, r, r, r, P, p, -p Anti-Suicide R, r, r Emotion Regulation R, R, R, R, R, R, R, R, R, R, R, P, P, P, P, P, P, L, L, L Interpersonal Boundaries r, r Interpersonal Influence R, r, r, r, r, r, r, p, p Self Punishment R, R, R, R, R, R, r, r, r, r, r Sensation Seeking r, r, r, r, r Results of 18 studies of reasons [R, r], self-report of phenomenology [P, p], or laboratory data [L, l].

29
Why People Self-Injure: Research
Primary sources of evidence 1) Reasons/motivations for self-injury 2) Experience of self-injury Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
 Reasons/motivations for self-injury. 2) Experience of self-injury. Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
30
Why People Self-Injure: Research
Primary sources of evidence 1) Reasons/motivations for self-injury 2) Experience of self-injury Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
 Reasons/motivations for self-injury. 2) Experience of self-injury. Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
31
Emotion Regulation 50-95% of self-injurers
“To release emotional pressure that builds up inside me” “To get rid of intolerable emotions” “To control how I am feeling” Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
32
Self-Punishment More than 50% of self-injurers
“To express anger at myself” “To punish myself” Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
33
Anti-Suicide 3rd most common reason
“To avoid the impulse to attempt suicide” “To stop suicidal ideation or attempts” “To stop me from killing myself” Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
34
Anti-Dissociation/Depersonalization
4rd most common reason “To know I am capable of feeling physical pain” “To feel like myself again” “To feel real” Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
35
Interpersonal Influence
5th most common reason “To let others know what I am going through” “To get those around me to understand what I’m going through” “To get reactions out of people” Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
36
Sensation/Excitement Seeking
6th most common reason “To feel exhilarated” “I thought it would be fun” Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
37
Why People Self-Injure: Research
Primary sources of evidence 1) Reasons/motivations for self-injury 2) Experience of self-injury Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
 Reasons/motivations for self-injury. 2) Experience of self-injury. Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
38
Why People Self-Injure: Research
Primary sources of evidence 1) Reasons/motivations for self-injury 2) Experience of self-injury Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.
 Reasons/motivations for self-injury. 2) Experience of self-injury. Klonsky, E.D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review.")
39
Emotions and Self-Injury
Before, During, and After Self-Injury Examples: Angry, Sad, Lonely, Frustrated, Worthless, Guilty Happy, Relieved, Hopeful, Satisfied Bored, Restless, Apathetic Unreal, Mesmerized, In a Trance Klonsky, E.D. (2009). The functions of self-injury in young adults who cut themselves: Clarifying the evidence for affect-regulation. Psychiatry Research.
. The functions of self-injury in young adults who cut themselves: Clarifying the evidence for affect-regulation. Psychiatry Research.")
40
Emotions and Self-Injury
Before Overwhelmed Sad Hurt Emotionally During Angry at Self Hurt Emotionally Isolated After Relieved Angry at Self Calm

41
Low-Arousal Negative Emotions

42
High-Arousal Negative Emotions

43
Low-Arousal Positive Emotions

44
Big Changes in Negative Arousal
Emotion Cohen’s d Relieved Calm Overwhelmed Anxious

45
Why People Self-Injure: Theories
Theory Description of Theory Anti-Dissociation To end the experience of depersonalization or dissociation Anti-Suicide To replace or compromise with the impulse to commit suicide Emotion Regulation To alleviate intense negative emotions Interpersonal Boundaries To assert one’s identity or a distinction between self and other Interpersonal Influence To seek help from or manipulate others Self Punishment To derogate or express anger towards oneself Sensation Seeking To generate excitement or exhilaration Sexual To control, distract from, or gratify uncomfortable sexual urges

46
Why People Self-Injure: Theories
Theory Description of Theory Anti-Dissociation To end the experience of depersonalization or dissociation Anti-Suicide To replace or compromise with the impulse to commit suicide Emotion Regulation To alleviate intense negative emotions Interpersonal Boundaries To assert one’s identity or a distinction between self and other Interpersonal Influence To seek help from or manipulate others Self Punishment To derogate or express anger towards oneself Sensation Seeking To generate excitement or exhilaration Sexual To control, distract from, or gratify uncomfortable sexual urges

47
Why People Self-Injure: Theories
Theory Description of Theory Anti-Dissociation To end the experience of depersonalization or dissociation Anti-Suicide To replace or compromise with the impulse to commit suicide Emotion Regulation To alleviate intense negative arousal Interpersonal Boundaries To assert one’s identity or a distinction between self and other Interpersonal Influence To seek help from or manipulate others Self Punishment To derogate or express anger towards oneself Sensation Seeking To generate excitement or exhilaration Sexual To control, distract from, or gratify uncomfortable sexual urges

48
Why People Self-Injure: Theories
Theory Description of Theory Anti-Dissociation To end the experience of depersonalization or dissociation Anti-Suicide To replace or compromise with the impulse to commit suicide Emotion Regulation To alleviate intense negative arousal Interpersonal Boundaries To assert one’s identity or a distinction between self and other Interpersonal Influence To seek help from or manipulate others Self Punishment To derogate or express anger towards oneself Sensation Seeking To generate excitement or exhilaration Sexual To control, distract from, or gratify uncomfortable sexual urges

49
Functions of Self-Injury
Organizing conceptual framework Valid and comprehensive assessment

50
Inventory of Statements about Self-injury (ISAS)
Assesses 13 functions of NSSI Three items per function 39-item measure Klonsky, E.D. & Olino. T.O. (2008). Identifying clinically distinct subgroups of self-injurers among young adults: A latent class analysis. Journal of Consulting and Clinical Psychology. Klonsky, E.D. & Glenn, C.R. (2009). Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS). Journal of Psychopathology and Behavioral Assessment.
. Identifying clinically distinct subgroups of self-injurers among. young adults: A latent class analysis. Journal of Consulting and Clinical Psychology. Klonsky, E.D. & Glenn, C.R. (2009). Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS). Journal of. Psychopathology and Behavioral Assessment.")
51
Sample I-SAS items “When I harm myself, I am…
Affect Regulation …calming myself down. Self-Punishment …expressing anger towards myself for being worthless or stupid. Anti-Suicide …putting a stop to suicidal thoughts. Anti-Dissociation …causing pain so I will stop feeling numb. Interpersonal Influence …letting others know the extent of my physical pain. Sensation Seeking …doing something to generate excitement or exhilaration. Peer Bonding …fitting in with others. Self-Care …creating a physical injury that is easier to care for than my emotional distress Marking Distress …creating a physical sign that I feel awful. Interpersonal Boundaries …creating a boundary between myself and others. Toughness …seeing if I can stand the pain. Revenge …getting back at someone. Autonomy …demonstrating I do not need to rely on others for help.

52
Inventory of Statements about Self-injury (ISAS)
235 self-injurers from a college sample 18-19 yrs old, 57% female, 42% Caucasian Hitting self, biting, cutting, pinching, wound-picking

53
Intrapersonal Functions
ISAS Factor loadings (Exploratory Factor Analysis with Promax Rotation) Function Mean (SD) Social Functions Intrapersonal Functions Affect Regulation Anti-Dissociation Anti-Suicide Marking Distress Self-Punishment Autonomy Interpersonal Boundaries Interpersonal Influence Peer Bonding Revenge Self-Care Sensation Seeking Toughness 3.0 (2.1) 1.0 (1.6) 0.8 (1.5) 1.5 (1.8) 2.0 (2.1) 0.6 (1.3) 0.8 (1.4) 0.5 (1.3) 0.6 (1.4) 0.7 (1.3) 1.0 (1.4) -.14 .21 . 35 .04 .64 .52 .54 .98 .53 .41 .87 .65 .69 .50 .42 .82 .84 .11 .26 .23 -.26 .16 .33 -.18 .02
 Function. Mean (SD) Social Functions. Intrapersonal Functions. Affect Regulation. Anti-Dissociation. Anti-Suicide. Marking Distress. Self-Punishment. Autonomy. Interpersonal Boundaries. Interpersonal Influence. Peer Bonding. Revenge. Self-Care. Sensation Seeking. Toughness. 3.0 (2.1) 1.0 (1.6) 0.8 (1.5) 1.5 (1.8) 2.0 (2.1) 0.6 (1.3) 0.8 (1.4) 0.5 (1.3) 0.6 (1.4) 0.7 (1.3) 1.0 (1.4)")
54
Intrapersonal Functions
ISAS Factor loadings (Exploratory Factor Analysis with Promax Rotation) Function Mean (SD) Social Functions Intrapersonal Functions Affect Regulation Anti-Dissociation Anti-Suicide Marking Distress Self-Punishment Autonomy Interpersonal Boundaries Interpersonal Influence Peer Bonding Revenge Self-Care Sensation Seeking Toughness 3.0 (2.1) 1.0 (1.6) 0.8 (1.5) 1.5 (1.8) 2.0 (2.1) 0.6 (1.3) 0.8 (1.4) 0.5 (1.3) 0.6 (1.4) 0.7 (1.3) 1.0 (1.4) -.14 .21 . 35 .04 .64 .52 .54 .98 .53 .41 .87 .65 .69 .50 .42 .82 .84 .11 .26 .23 -.26 .16 .33 -.18 .02
 Function. Mean (SD) Social Functions. Intrapersonal Functions. Affect Regulation. Anti-Dissociation. Anti-Suicide. Marking Distress. Self-Punishment. Autonomy. Interpersonal Boundaries. Interpersonal Influence. Peer Bonding. Revenge. Self-Care. Sensation Seeking. Toughness. 3.0 (2.1) 1.0 (1.6) 0.8 (1.5) 1.5 (1.8) 2.0 (2.1) 0.6 (1.3) 0.8 (1.4) 0.5 (1.3) 0.6 (1.4) 0.7 (1.3) 1.0 (1.4)")
55
Relationship of Functions to NSSI Frequency
NSSI Behavior Social Functions α = .87 Intrapersonal Functions α = .80 Cutting Needle sticking Carving Banging/Hitting self .19 .30 .18 .13 Note. All correlations are statistically significant at an alpha of .03.

56
Relationship of Functions to Cutting
Correlation with Cutting Affect Regulation Anti-Dissociation Anti-Suicide Marking Distress Self-Punishment Autonomy Interpersonal Boundaries Interpersonal Influence Peer Bonding Revenge Self-Care Sensation Seeking Toughness .21 .24 .23 .22 .04 .15 -.01 .09 .06 .11 Note. Correlations above .20 are statistically significant at an alpha of .001.

57
Relationship of Functions to Clinical Variables
Social Functions α = .87 Intrapersonal Functions α = .80 Depression Anxiety Borderline Personality Disorder .24 .33 .14 .42* .36 .43* Note. Correlations above .16 are statistically significant an at alpha level of .01. * Indicates correlations are significantly different at an alpha of .01.

58
Relationship of Functions to Clinical and Contextual Variables
Clinical/Contextual Variable Social Functions α = .87 Intrapersonal Functions α = .80 Suicidal Ideation Suicide Plans Attempted Suicide .10 .14 .12 .32* .33* .29* Note. Correlations above .16 are statistically significant an at alpha level of .01. * Indicates correlations are significantly different at an alpha of .01.

59
ISAS in Alexian Brothers Hospital
108 psychiatric patients Ages 11 – 62, mean=19 90% female 72% Caucasian

60
Function Social Intrapersonal .77 .62 .50 .75 .67 .55 .44 .51 .95 .47
Affect Regulation .77 Anti-Dissociation .62 Anti-Suicide .50 Marking Distress .75 Self-Punishment .67 Autonomy .55 Interpersonal Boundaries .44 Interpersonal Influence .51 Peer Bonding .95 Revenge .47 Self-Care .39 .41 Sensation Seeking .71 Toughness .37 .43

61
ISAS in an Adolescent Psychiatric Sample
80 psychiatric patients with NSSI from South Oaks Hospital in Long Island, NY Mean age = 15 ( ) 70% female 61% Caucasian
 70% female. 61% Caucasian.")
62
Function Social Intrapersonal .87 .83 .66 .63 .77 .79 .69 .54 .70 .36
Affect Regulation .87 Anti-Dissociation .83 Anti-Suicide .66 Marking Distress .63 Self-Punishment .77 Autonomy .79 Interpersonal Boundaries .69 Interpersonal Influence .54 Peer Bonding Revenge .70 Self-Care .36 .37 Sensation Seeking .73 Toughness .72

63
FASM in Alexian Brothers Sample
Item Social Intrapersonal Receive more attention (S-P) .83 Get a reaction (S-P) .75 Feel more a part of a group (S-P) .74 Get parents to notice (S-P) .72 Get attention (S-P) .64 Avoid something unpleasant (S-N) .63 Avoid school/work/activities (S-N) .55 Stop bad feelings (I-N) .68 Feel something (I-P) Relive feeling numb/empty (I-N) Punish self (I-P) .58 Feel relaxed (I-P) .54 First letter social or intrapersonal, second letter positive or negative
 .83. Get a reaction (S-P) .75. Feel more a part of a group (S-P) .74. Get parents to notice (S-P) .72. Get attention (S-P) .64. Avoid something unpleasant (S-N) .63. Avoid school/work/activities (S-N) .55. Stop bad feelings (I-N) .68. Feel something (I-P) Relive feeling numb/empty (I-N) Punish self (I-P) .58. Feel relaxed (I-P) .54. First letter social or intrapersonal, second letter positive or negative.")
64
Two Motivational Dimensions
1. Self-Focused 2. Other-Focused

65
Two Motivational Dimensions
1. Self-Focused 2. Other-Focused Affect Regulation Anti-Dissociation Anti-Suicide Marking Distress Self-Punishment

66
Two Motivational Dimensions
1. Self-Focused 2. Other-Focused Affect Regulation Interpersonal Influence Anti-Dissociation Peer Bonding Anti-Suicide Revenge Marking Distress Excitement Seeking Self-Punishment Toughness

67
Two Motivational Dimensions
1. Self-Focused 2. Other-Focused More Self-Injury More Psychopathology More Suicidality

68
NSSI Motivations: Summary
Most common motivations are emotion regulation and self-punishment NSSI motivations fall into two super-ordinate dimensions: 1) self-focused and 2) other-focused Self-focused motivations are associated with greatest clinical severity Informs treatment
 self-focused and 2) other-focused. Self-focused motivations are associated with greatest clinical severity. Informs treatment.")
69
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Relationship to Suicide

70
NSSI vs. Attempted Suicide
Differ in terms of intent and medical severity Commonly co-occur Avoid oversimplified conclusions! Complex relationship needs careful study Involuntary Hospitalization, Breaking Confidentiality and Trust, mobilizing emergency services when not necessary, perhaps missing someone truly suicidal because increased attention is paid to the salient wound resulting from non-suicidal self-injury

71
NSSI vs. Attempted Suicide
NSSI sometimes mistaken for attempted suicide Unnecessary hospitalizations Harms case conceptualization Misallocates valuable resources NSSI conveys valuable information regarding suicide risk Results from 4 Studies: Does NSSI predict attempted suicide? Involuntary Hospitalization, Breaking Confidentiality and Trust, mobilizing emergency services when not necessary, perhaps missing someone truly suicidal because increased attention is paid to the salient wound resulting from non-suicidal self-injury

72
Predictors of Attempted Suicide 139 Adolescent Psychiatric Inpatients
Suicide Ideation NSSI Borderline Personality Disorder .37 Depression Anxiety Impulsivity

73
Predictors of Attempted Suicide 426 High-School Students
Suicide Ideation NSSI Borderline Personality Disorder .29 Depression Anxiety Impulsivity

74
Predictors of Attempted Suicide 1,351 Undergraduates
Suicide Ideation NSSI Borderline Personality Disorder .22 Depression Anxiety Impulsivity

75
Predictors of Attempted Suicide 438 United States Adults
Suicide Ideation NSSI

76
Summary of Results From Four Studies
NSSI relates to attempted suicide NSSI relates to attempted suicide more strongly than other risk-factors NSSI is similar to suicide ideation in conferring risk for suicide Yet, like suicide ideation, many/most who engage in NSSI have not attempted suicide

77
?? Why does NSSI have such a strong relationship to attempted suicide?
Thomas Joiner’s Interpersonal-Psychological Theory Desire + Capability Suicide

78
?? Most risk factors only confer desire Others only confer capability
Depression Hopelessness Suicidal ideation Others only confer capability Access to lethal means Combat exposure in military

79
?? NSSI confers both desire and capability
Desire (intense negative emotions) Capability (habituation to self-inflicted violence) (Nock et al., 2006) NSSI is relatively unique among risk-factors in that it represents double-trouble!
 Capability (habituation to self-inflicted violence) (Nock et al., 2006) NSSI is relatively unique among risk-factors in that it represents double-trouble!")
80
So what have we learned? Is NSSI a form of suicidal behavior? No!
Is NSSI unrelated to attempted suicide? NSSI is different from attempted suicide, but confers strong suicide risk because it represents double-trouble (both desire + capability)
")
81
Suicide: Take-Home Message
NSSI is not attempted suicide, but… … People who self-injure are at greater risk for suicidal ideation … People who self-injure are more capable of acting on suicidal thoughts

82
For more information… Published 2011
User-friendly information for health professionals

83
Thank you Graduate Students Funding Sources Catherine Glenn Alexis May
Sarah Victor Anita Hibbert Funding Sources National Institute of Mental Health American Foundation for Suicide Prevention Stony Brook University Center for Survey Research

84
Questions, Comments, Discussion??
Thank you!! Questions, Comments, Discussion??

85
Extra Slides

86
NSSI and BPD DSM-IV: NSSI is part of a BPD criterion
DSM-5: NSSI proposed as own diagnostic entity What exactly is the relationship of NSSI to BPD?

87
What BPD and NSSI Share Frequently co-occur
Both have emotion dysregulation as a core feature Both associated with shame

88
Can NSSI be Distinct from BPD?
198 Adolescent Psychiatric Inpatients Average of 3.3 Axis-I diagnoses Two Key Questions: Does BPD overlap with NSSI more than with other disorders? Does NSSI overlap with BPD more than with other disorders?

89
Of those with BPD… … 78% NSSI … 84% Anxiety Disorder
… 84% Disruptive Behavior Disorder (ODD or Conduct) … 78% Mood Disorder
 … 78% Mood Disorder.")
90
Of those with NSSI… … 52% BPD … 74% Anxiety Disorder … 73% ADHD
… 66% Mood Disorder

91
NSSI and BPD: Conclusions
NSSI and BPD are correlated, but … Many who have BPD do not self-injure Many who self-injure do not have BPD

92
Clinical Take-Home Message
Diagnosis of BPD is not implied by presence of NSSI, but made through careful assessment on a case-by-case basis. Think of BPD and NSSI as you do Depression and Suicidality… … they often co-occur and even contribute to one another, yet are best view as distinct phenomena

93
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Key Clinical Issues: Borderline Personality Disorder DSM-5 Suicide

94
A Distinct NSSI Diagnosis?
A symptom of a personality disorder in DSM-IV Proposed as a Behavioral Disorder for DSM-V

95
The Process Group of Experts Lots of phone and email discussions
Members from Mood Disorders and Child/Adolescent Disorders Workgroups Advisors with particular expertise in NSSI Lots of phone and discussions Separateness Independent Clinical Significance Threshold Defining Characteristics Differentiation from other Behaviors/Disorders

96
And the proposed NSSI diagnosis is ………..
…not going to take effect in DSM-5 … but will appear in DSM-5 appendix as a research diagnosis

97
A. In the last year, the individual has, on 5 or more days, engaged in intentional self-inflicted damage to the surface of his or her body, of a sort likely to induce bleeding or bruising or pain (e.g., cutting, burning, stabbing, hitting, excessive rubbing), for purposes not socially sanctioned (e.g., body piercing, tattooing, etc.), but performed with the expectation that the injury will lead to only minor or moderate physical harm. The absence of suicidal intent is either reported by the patient or can be inferred by frequent use of methods that the patient knows, by experience, not to have lethal potential. (When uncertain, code with NOS 2.) The behavior is not of a common and trivial nature, such as picking at a wound or nail biting. B. The intentional injury is associated with at least 2 of the following: 1. Negative feelings or thoughts, such as depression, anxiety, tension, anger, generalized distress, or self-criticism, occurring in the period immediately prior to the self-injurious act. 2. Prior to engaging in the act, a period of preoccupation with the intended behavior that is difficult to resist. 3. The urge to engage in self-injury occurs frequently, although it might not be acted upon. 4. The activity is engaged in with a purpose; this might be relief from a negative feeling/cognitive state or interpersonal difficulty or induction of a positive feeling state. The patient anticipates these will occur either during or immediately following the self-injury.
, for purposes not socially sanctioned (e.g., body piercing, tattooing, etc.), but performed with the expectation that the injury will lead to only minor or moderate physical harm. The absence of suicidal intent is either reported by the patient or can be inferred by frequent use of methods that the patient knows, by experience, not to have lethal potential. (When uncertain, code with NOS 2.) The behavior is not of a common and trivial nature, such as picking at a wound or nail biting. B. The intentional injury is associated with at least 2 of the following: 1. Negative feelings or thoughts, such as depression, anxiety, tension, anger, generalized distress, or self-criticism, occurring in the period immediately prior to the self-injurious act. 2. Prior to engaging in the act, a period of preoccupation with the intended behavior that is difficult to resist. 3. The urge to engage in self-injury occurs frequently, although it might not be acted upon. 4. The activity is engaged in with a purpose; this might be relief from a negative feeling/cognitive state or interpersonal difficulty or induction of a positive feeling state. The patient anticipates these will occur either during or immediately following the self-injury.")
98
Agenda What is Self-Injury Who Self-Injures Why People Self-Injure
Key Clinical Issues: Borderline Personality Disorder DSM-5 Suicide

99
Some Overall Clinical Conclusions
Treatment should emphasize Functions (functional assessment) Negative Emotions (emotion regulation skills) Self-criticism (cognitive techniques) Arousal regulation (exercise?) Careful Diagnosis Suicidality should be carefully monitored
 Negative Emotions (emotion regulation skills) Self-criticism (cognitive techniques) Arousal regulation (exercise ) Careful Diagnosis. Suicidality should be carefully monitored.")
100
Choose your own adventure
Why do people choose NSSI and not something else? (role of self-derogation/criticism) Physiologically speaking, how does NSSI work? Is NSSI an ‘addictive’ behavior? Why is physical pain reduced in NSSI?
 Physiologically speaking, how does NSSI work Is NSSI an ‘addictive’ behavior Why is physical pain reduced in NSSI")
101
Many ways to cope with negative emotions …
why self-injury?

102
Self-Derogation Self-injurers consistently score high on measures of self- derogation, self-criticism, and low self-esteem Klonsky, Oltmanns, & Turkheimer, 2003, American Journal of Psychiatry; Klonsky & Muehlenkamp, 2007, Journal of Clinical Psychology/In Session; Glassman et al., 2007, Behaviour Research and Therapy) Self-punishment/self-directed anger is the second most common motivation for self-injury (Klonsky, 2007, Clinical Psychology Review) “To express anger at myself” (Klonsky, 2009, Psychiatry Research)
 Self-punishment/self-directed anger is the second most. common motivation for self-injury (Klonsky, 2007, Clinical Psychology Review) To express anger at myself (Klonsky, 2009, Psychiatry Research)")
103
NESD Theory For those high in negative emotionality (NE) and
self-derogation (SD) … … Self-injury is an ego-syntonic regulation method … Self-injury uniquely fulfills a self punishment function
 … … Self-injury is an ego-syntonic regulation method. … Self-injury uniquely fulfills a self punishment function.")
104
NESD Model Temperament Self-injury Intense self-derogation
Intense, negative emotions Normative/Low Environment self-derogation Other healthy & unhealthy coping

105
NESD Theory Hypothesis: Those high in both negative
emotionality (NE) and self-derogation (SD) are most likely to self-injure Predicts a statistical interaction between NE and SD in identifying self-injurers
 and self-derogation (SD) are. most likely to self-injure. Predicts a statistical interaction between NE and. SD in identifying self-injurers.")
106
Sample 1: Young Adults 2,011 Air Force recruits in basic training
Thomas, Turkheimer, & Oltmanns. (2003). Factorial structure of pathological personality traits as evaluated by peers. Journal of Abnormal Psychology. Mean age 20 (SD=5), 62% Male, 65% Caucasian, 17% African American Administered the Schedule for Nonadaptive and Adaptive Personality (SNAP; Clark, 1996)
. Factorial structure of pathological personality traits as evaluated by. peers. Journal of Abnormal Psychology. Mean age 20 (SD=5), 62% Male, 65% Caucasian, 17% African American. Administered the Schedule for Nonadaptive and Adaptive. Personality (SNAP; Clark, 1996)")
107
Self-Injury “When I get very tense, hurting myself physically somehow calms me down” “I have hurt myself on purpose several times” 1% endorsed both of these items

108
Negative Emotionality
SNAP Negative Temperament Scale 28 items: “I often have strong feelings such as anxiety or anger..” True-False format

109
Self-Derogation SNAP Self-Derogation/Low Self-Esteem scale
7 items: “I’ve really made a mess of my life” True-False format

110
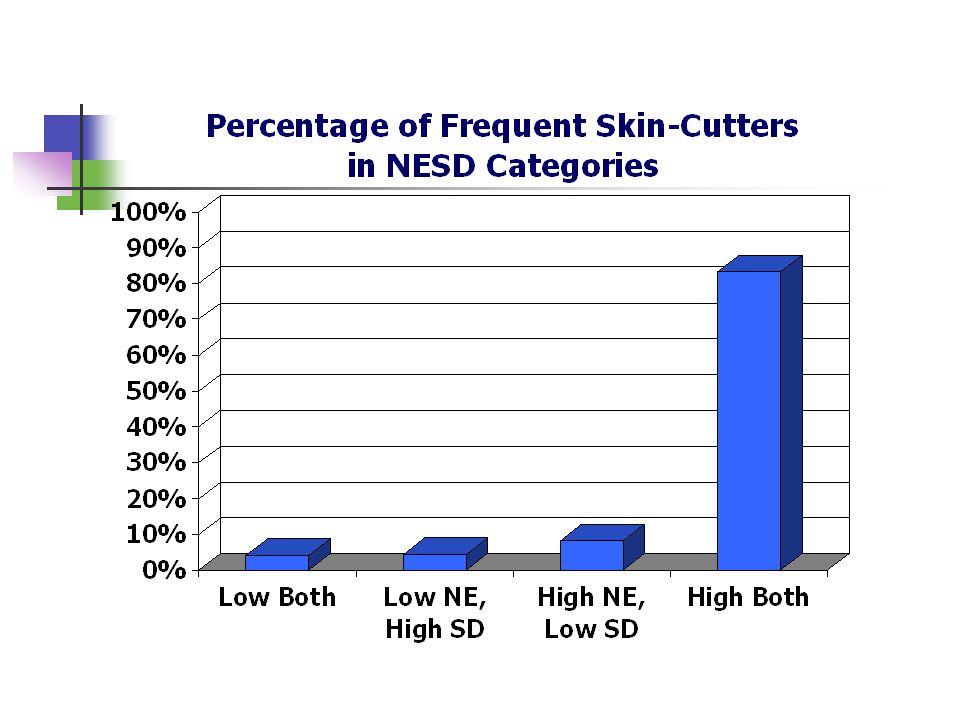
Results Negative Emotionality (NE) 1.29 -.01
Frequent Injurers Control Negative Emotionality (NE) Self-Derogation (SD) NE and SD interact to distinguish frequent cutters from controls (Binary Logistic Regression: Wald’s X2(1)=3.24, p=.07)
 Self-Derogation (SD) NE and SD interact to distinguish frequent cutters from. controls (Binary Logistic Regression: Wald’s X2(1)=3.24, p=.07)")
112
Sample 2: Adolescents 432 high-school students Ages 13-17, 61% Female
53% Caucasian, 19% Hispanic, 15% Asian, 11% African American

113
Self-Injury Section I of the Inventory of Statements About Self-injury
(ISAS; Klonsky & Olino, 2008; Klonsky & Glenn, in press) Self-injurious behaviors done “intentionally” and “without suicidal intent” 12 different behaviors: “cutting,” “scratching,” “needle- sticking” 6.5% Cut 3 or more times
 Self-injurious behaviors done intentionally and without. suicidal intent 12 different behaviors: cutting, scratching, needle- sticking 6.5% Cut 3 or more times.")
114
Negative Emotionality
Composite of two measures Positive and Negative Affect Scale (PANAS; Watson & Clark, 1994) 10-items: “Upset,” “Ashamed,” “Irritable” [just NA scale] Difficulties in Emotion Regulation Scale (DERS; Gratz, 2004) 36-items: “When I’m upset, my emotions feel overwhelming” PANAS NA scale and DERS correlated r=.68
 10-items: Upset, Ashamed, Irritable [just NA scale] Difficulties in Emotion Regulation Scale (DERS; Gratz, 2004) 36-items: When I’m upset, my emotions feel overwhelming PANAS NA scale and DERS correlated r=.68.")
115
Self-Derogation Composite of three measures
Self-Derogation scale from the Schedule for Nonadaptive and Adaptive Personality (SNAP; Clark, 1996) 7-items: “I’ve really made a mess of my life” Self-Perception Profile for Adolescents-Revised (SPPA; Harter, 1988; Wichstrom, 1995) Global Self-Worth 5-items: “often disappointed with [yourself]” Physical Appearance 5-items: “not happy with the way [you] look”
 7-items: I’ve really made a mess of my life Self-Perception Profile for Adolescents-Revised (SPPA; Harter, 1988; Wichstrom, 1995) Global Self-Worth 5-items: often disappointed with [yourself] Physical Appearance 5-items: not happy with the way [you] look")
116
Results Negative Emotionality (NE) 1.01 -.07
Frequent Cutters Control Negative Emotionality (NE) Self-Derogation (SD) NE and SD interact to distinguish frequent cutters from controls (Binary Logistic Regression: Wald’s X2(1)=3.86, p<.05)
 Self-Derogation (SD) NE and SD interact to distinguish frequent cutters from. controls (Binary Logistic Regression: Wald’s X2(1)=3.86, p<.05)")
118
NESD Theory: Next Steps
Preliminary evidence supports NESD theory Examine large group of severe self-injurers Consider functions of self-injury (e.g., Klonsky & Olino, 2008)
")
119
Parasympathetic Rebound Theory
How Does NSSI Work? Parasympathetic Rebound Theory Informs treatment

120
Parasympathetic Rebound Theory
Sympathetic nervous system – “fight or flight” Intense emotion: Fear, rage, panic Increases heart rate Increases blood flow to major muscle gruops Parasympathetic nervous system – “rest and digest” Limits effects of sympathetic system Slows heart rate Facilitates sustained engagement and attention Informs treatment

121
Parasympathetic Impairment
Inability to restrain sympathetic responses and emotions (panic, anger) Impaired parasympathetic activity observed in self-injury and Borderline Personality Disorder (Austin et al, 2007; Crowell et al., 2005; Weinberg, Hajcak, Klonsky, 2009)
 Impaired parasympathetic activity observed in self-injury and Borderline Personality Disorder (Austin et al, 2007; Crowell et al., 2005; Weinberg, Hajcak, Klonsky, 2009)")
122
Parasympathetic Rebound
Surges in sympathetic activity are followed by increases in parasympathetic activity What if surges are too strong or too weak? Too strong: fainting Too weak: emotional dysregulation observed in BPD and self-injurers Perhaps self-injury causes a surge in sympathetic activity which in turn triggers a strong parasympathetic rebound?

123
Parasympathetic Rebound
Some self-injurers report that seeing the blood is important for achieving calming influence of self-injury (Glenn & Klonsky, 2010) Interestingly, the fainting response observed in blood phobics is often attributed to parasympathetic rebound The pain and blood caused by self-injury may both trigger a parasympathetic rebound
 Interestingly, the fainting response observed in blood phobics is often attributed to parasympathetic rebound. The pain and blood caused by self-injury may both trigger a parasympathetic rebound.")
124
Parasympathetic Activity Pre- and Post- Self-Injury
Mean RSA Minutes NSSI Data from Matthew Nock, shown with permission (Nock & Mendes, in preparation)
")
Similar presentations



 February 28, 2014 PSYC 2340: Abnormal Psychology Brett Deacon, Ph.D.>")



 A pervasive pattern of instability of interpersonal relationships, self-image.>")


 Lethality Repetition Tissue Damage Scratch, burn, cut.>")









