Download presentation
Presentation is loading. Please wait.

1
Liver and Biliary Tract-Tumors
Inga Gurevich, MD, PhD May, 2008

2
Liver - Benign Tumors and Tumor Like Conditions
Focal nodular hyperplasia Liver cell adenoma Hemangioma (most common benign lesion) Mesenchymal hamartoma
 Mesenchymal hamartoma.")
3
Focal nodular hyperplasia (FNH)
Common (#2 liver tumor after hemangioma) Mass lesion of young (median age 38 years); some studies show female predominance Represents 2-10% of pediatric hepatic tumors May be associated with oral contraceptives (66-95% of cases), hepatic cavernous hemangioma (20%), glycogen storage disease type Ia, portal hypertension Tumors associated with oral contraceptives often have hemorrhage, necrosis, infarction Usually an incidental finding; present in 1% of autopsies Xray: mass with central scar, centrifugal hypervascularity by angiography; CT and MRI are important, Treatment: excellent prognosis; discontinue oral contraceptives, if applicable; surgery if symptomatic, complications, compression of adjacent organs or lesion progression
 Mass lesion of young (median age 38 years); some studies show female predominance. Represents 2-10% of pediatric hepatic tumors. May be associated with oral contraceptives (66-95% of cases), hepatic cavernous hemangioma (20%), glycogen storage disease type Ia, portal hypertension. Tumors associated with oral contraceptives often have hemorrhage, necrosis, infarction. Usually an incidental finding; present in 1% of autopsies. Xray: mass with central scar, centrifugal hypervascularity by angiography; CT and MRI are important, Treatment: excellent prognosis; discontinue oral contraceptives, if applicable; surgery if symptomatic, complications, compression of adjacent organs or lesion progression.")
4
Focal nodular hyperplasia
Well-demarcated, subcapsular, light brown to yellow ; bulging nodule, 70-80% solitary, up to 5 -10cm; has central gray-white stellate scar (unless < 1 cm) from which fibrous septa radiate to periphery and create multiple smaller nodules; hemorrhage, necrosis, infarction, bile staining often seen; larger tumors may have multiple scars; adjacent liver is normal
 from which fibrous septa radiate to periphery and create multiple smaller nodules; hemorrhage, necrosis, infarction, bile staining often seen; larger tumors may have multiple scars; adjacent liver is normal.")
5
Focal nodular hyperplasia
Micro: Most tumors (80%) have the 3 classic features of abnormal architecture, bile ductular proliferation and malformed vessels. Non-classic forms lack either abnormal architecture or malformed vessels, and are divided into three types - (a) telangiectatic, (b) mixed hyperplastic and adenomatous or (c) atypia of large cell Positive stains: alpha-1-antitrypsin Negative stains: p53, CD143 (angiotensin I-converting enzyme: reduced expression DD: Osler-Weber-Rendu disease, Budd-Chiari syndrome or cirrhosis (adjacent liver is not normal), fibrolamellar hepatocellular carcinoma (marked atypia of hepatocytes), hepatocellular adenoma (encapsulated, monoclonal)
 have the 3 classic features of abnormal architecture, bile ductular proliferation and malformed vessels. Non-classic forms lack either abnormal architecture or malformed vessels, and are divided into three types - (a) telangiectatic, (b) mixed hyperplastic and adenomatous or (c) atypia of large cell. Positive stains: alpha-1-antitrypsin. Negative stains: p53, CD143 (angiotensin I-converting enzyme: reduced expression. DD: Osler-Weber-Rendu disease, Budd-Chiari syndrome or cirrhosis (adjacent liver is not normal), fibrolamellar hepatocellular carcinoma (marked atypia of hepatocytes), hepatocellular adenoma (encapsulated, monoclonal)")
6
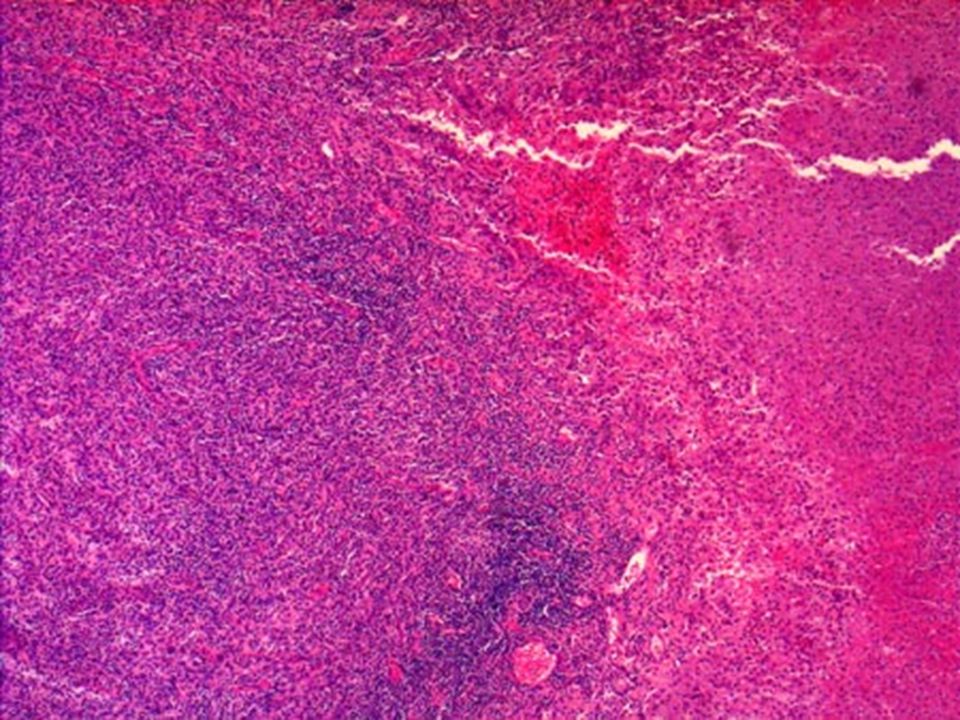
Focal nodular hyperplasia (FNH)
There is a central gray-white, depressed stellate scar with fibrous septa radiating to the periphery. The central scar contains large vessels with fibromuscular hyperplasia +intense lymphocytic infiltrates and bile duct proliferation + normal hepatocytes with regeneration.

7
Liver Cell Adenoma 95% women, usually child-bearing age (very rare in children), history of 5+ years of oral contraceptives in 85% ; also associated with anabolic steroids (in men), anti-estrogens, Klinefelter’s syndrome Also associated with glycogen storage disease types Ia and III, Fanconi’s anemia, familial adenomatous polyposis, familial diabetes mellitus, Hurler’s disease or tyrosinemia; Spontaneous 2-4% of hepatic tumors in children Subcapsular tumors may rupture, particularly during pregnancy Benign, but may contain hepatocellular carcinoma or cause severe hemorrhage 10% or lower risk of hepatocellular carcinoma if not resected Must sample generously to rule out coexisting hepatocellular carcinoma
, history of 5+ years of oral contraceptives in 85% ; also associated with anabolic steroids (in men), anti-estrogens, Klinefelter’s syndrome. Also associated with glycogen storage disease types Ia and III, Fanconi’s anemia, familial adenomatous polyposis, familial diabetes mellitus, Hurler’s disease or tyrosinemia; Spontaneous. 2-4% of hepatic tumors in children. Subcapsular tumors may rupture, particularly during pregnancy. Benign, but may contain hepatocellular carcinoma or cause severe hemorrhage. 10% or lower risk of hepatocellular carcinoma if not resected. Must sample generously to rule out coexisting hepatocellular carcinoma.")
8
Liver Cell Adenoma Gross: solitary pale, yellow-tan, frequently bile-stained nodules, often subcapsular, cm, sharply demarcated or encapsulated; usually right lobe; usually no fibrous septa or central scar; adjacent liver is non-cirrhotic

9
Liver Cell Adenoma Normal liver tissue with a portal tract is seen on the left. The hepatic adenoma is on the right and is composed of cells that closely resemble normal hepatocytes, but the neoplastic liver tissue has disorganized (portal tracts are absent) hepatocyte cords and does not contain a normal lobular architecture.
 hepatocyte cords and does not contain a normal lobular architecture.")
10
Liver Cell Adenoma Micro: sheets and cords 1-3 cells thick of normal appearing hepatocytes; no/rare mitotic figures; no portal tracts, no central veins ; intact reticulin framework; pseudoglands may be present; but no atypia Positive stains: ER, PR Negative stains: p53 DD: hepatocellular carcinoma (mitotic activity, atypia, trabecular growth, cell plates > 2 cells thick, vascular invasion, infiltrative, often different clinical features), focal nodular hyperplasia (central stellate scar and radiating fibrous septa)
, focal nodular hyperplasia (central stellate scar and radiating fibrous septa)")
11
Hemangioma Most common primary hepatic tumor
Usually an incidental finding More common in adults than children, 75% in women 10% enlarge with follow-up, may be related to pregnancy or oral contraceptives Associated with multiple focal nodular hyperplasia syndrome Giant cavernous hemangiomas (> 4-10 cm) only rarely rupture
 only rarely rupture.")
12
Hemangioma Gross: solitary (70-90%), usually 2-4 cm, although tumors up to 20 cm are overrepresented in studies of excisions; soft, red-purple, well circumscribed; subcapsular or deep; collapse when sectioned as blood oozes out
, usually 2-4 cm, although tumors up to 20 cm are overrepresented in studies of excisions; soft, red-purple, well circumscribed; subcapsular or deep; collapse when sectioned as blood oozes out.")
13
Hemangioma Micro: variably sized vascular spaces lined by flat endothelial cells and myxoid or fibrous stroma; large fibrous septa may trap bile ducts; variable thrombosis, calcification, increased fibrosis with age of lesion may obliterate lumen

14
Mesenchymal Hamartoma
Formerly called cavernous lymphangioadenomatoid tumor, cystic hamartoma, benign mesenchymoma 75% are age 1 year or less (rarely adults), 60-70% male 8% of pediatric liver tumors Usually asymptomatic Serum AFP is usually normal or mildly elevated Rarely associated with undifferentiated sarcoma Adult cases are usually women with abdominal pain, more prominent fibrosis and a lesser myxoid component than childhood cases, usually no extramedullary hematopoiesis Treatment: excision, liver transplantation may be necessary
, 60-70% male. 8% of pediatric liver tumors. Usually asymptomatic. Serum AFP is usually normal or mildly elevated. Rarely associated with undifferentiated sarcoma. Adult cases are usually women with abdominal pain, more prominent fibrosis and a lesser myxoid component than childhood cases, usually no extramedullary hematopoiesis. Treatment: excision, liver transplantation may be necessary.")
15
Mesenchymal Hamartoma
Gross: well circumscribed, solitary, 5-23 cm, 20% pedunculated, myxoid mass with fluid filled cysts; usually no necrosis, hemorrhage or calcification; interstitial deletion near 19q13.4

16
Mesenchymal Hamartoma
Micro: branching bile ducts without atypia in a loose, myxoid stroma with myofibroblast-like cells dilated vessels and lymphatics; also normal appearing hepatocytes, thick walled veins, variable collagen bile ducts may have mesenchymal collars and are often cystically dilated

17
Mesenchymal Hamartoma
Positive stains: CK7, vimentin, smooth muscle actin, desmin, actin Negative stains: CK20 Molecular: interstitial deletion near 19q13.4 DD: bile duct adenoma (no hepatocyte islands) or cystadenoma (adults), bile duct hamartoma (usually multiple with fibrous background), infantile hemangioendothelioma (more vascular), embryonal sarcoma (marked cellularity and atypical cells)
 or cystadenoma (adults), bile duct hamartoma (usually multiple with fibrous background), infantile hemangioendothelioma (more vascular), embryonal sarcoma (marked cellularity and atypical cells)")
18
Liver Cell Tumors - Malignant
Hepatocellular carcinoma Hepatoblastoma Epithelioid hemangioendothelioma Angiosarcoma Undifferentiated (embryonal) sarcoma Squamous Cell Carcinoma Carcinoid Tumor Lymphoma/leukemia
 sarcoma. Squamous Cell Carcinoma. Carcinoid Tumor. Lymphoma/leukemia.")
19
Hepatocellular carcinoma
85% of hepatic malignancies (30% in children); major cause of cancer death worldwide (20-40% in China, Japan, sub-Saharan African) Primary carcinomas are rare in North America, but more common in countries bordering Mediterranean Sea endemic for viral hepatitis; highest rates in Korea, Taiwan, southeast China, Mozambique; Higher rates in blacks vs. whites (4:1) Most are age 60+ years with cirrhosis or ages years without cirrhosis, occasionally are second tumors in Wilm’s tumor patients Risk factors/causes: hepatitis B virus (HBV), cirrhosis (85% in West with HCC have cirrhosis, 3% with cirrhosis develop HCC annually), hepatitis C virus (HCV), alcohol abuse, aflatoxins, Thorotrast exposure, androgenic steroids, tyrosinemia
; major cause of cancer death worldwide (20-40% in China, Japan, sub-Saharan African) Primary carcinomas are rare in North America, but more common in countries bordering Mediterranean Sea endemic for viral hepatitis; highest rates in Korea, Taiwan, southeast China, Mozambique; Higher rates in blacks vs. whites (4:1) Most are age 60+ years with cirrhosis or ages years without cirrhosis, occasionally are second tumors in Wilm’s tumor patients. Risk factors/causes: hepatitis B virus (HBV), cirrhosis (85% in West with HCC have cirrhosis, 3% with cirrhosis develop HCC annually), hepatitis C virus (HCV), alcohol abuse, aflatoxins, Thorotrast exposure, androgenic steroids, tyrosinemia.")
20
Hepatocellular carcinoma
Symptoms: abdominal pain, ascites, hepatomegaly, obstructive jaundice; also systemic manifestations Laboratory: elevated serum AFP (70% sensitive), tumors arising in noncirrhotic liver (33%), tumors 2 cm or less (25%) Screening: recommended to use ultrasound and serum AFP in patients with chronic liver disease; leads to diagnosis of tumors 2 cm or less Other causes of elevated serum AFP: yolk sac tumors of gonads, cirrhosis, massive liver necrosis, chronic hepatitis, normal pregnancy, fetal neural tube defects, hepatoblastoma 5 year survival: 10% normally to 50% in tumors 5 cm or less with resection; death usually within 1 year from cachexia, GI bleed, liver failure, rupture of tumor (10%) Metastases: initially within liver, distant metastases late to lungs, bone, adrenal gland or porta hepatis lymph nodes
, tumors arising in noncirrhotic liver (33%), tumors 2 cm or less (25%) Screening: recommended to use ultrasound and serum AFP in patients with chronic liver disease; leads to diagnosis of tumors 2 cm or less. Other causes of elevated serum AFP: yolk sac tumors of gonads, cirrhosis, massive liver necrosis, chronic hepatitis, normal pregnancy, fetal neural tube defects, hepatoblastoma. 5 year survival: 10% normally to 50% in tumors 5 cm or less with resection; death usually within 1 year from cachexia, GI bleed, liver failure, rupture of tumor (10%) Metastases: initially within liver, distant metastases late to lungs, bone, adrenal gland or porta hepatis lymph nodes.")
21
Hepatocellular carcinoma
Favorable prognosis factors: low stage, encapsulation, single lesion, tumor size < 5 cm, fibrolamellar variant, no cirrhosis (independent of fibrolamellar subtype), no vascular invasion, negative surgical margins Poor prognostic factors: microscopic vascular invasion, high nuclear grade (grade 3 of 3) Factors that are not prognostic: age, gender, HBV status Classification: small (< 2 cm) or advanced (2 cm or more) Treatment: resection, transplantation
, no vascular invasion, negative surgical margins. Poor prognostic factors: microscopic vascular invasion, high nuclear grade (grade 3 of 3) Factors that are not prognostic: age, gender, HBV status. Classification: small (< 2 cm) or advanced (2 cm or more) Treatment: resection, transplantation.")
22
Hepatocellular carcinoma
Gross: unifocal, multifocal or diffusely infiltrative soft tumor, paler than normal tissue, may be green due to bile; extensive intrahepatic metastases are common; snakelike masses of tumor may involve the portal vein (35-80%), hepatic vein (20%) or inferior vena cava); hemorrhage and necrosis are common; liver usually cirrhotic, often enlarged
, hepatic vein (20%) or inferior vena cava); hemorrhage and necrosis are common; liver usually cirrhotic, often enlarged.")
23
Hepatocellular carcinoma
Micro patterns are trabecular (most common) with 4+ cells surrounded by layer of flattened endothelial cells solid (compact) pseudoglandular (acinar with proteinaceous material or bile in lumina, may resemble thyroid follicles) pelioid, giant cell sarcomatoid clear cell pattern
 with 4+ cells surrounded by layer of flattened endothelial cells. solid (compact) pseudoglandular (acinar with proteinaceous material or bile in lumina, may resemble thyroid follicles) pelioid, giant cell. sarcomatoid. clear cell pattern.")
24
Hepatocellular carcinoma
Well differentiated: thin plates (1-3 hepatocytes thick), cells smaller than normal, abnormal reticulin network; minimal nuclear atypia, nuclear density 2x normal liver; commonly fatty change and pseudoglands; may resemble hepatocyte adenoma; common pattern for small hepatocellular carcinoma Moderately differentiated: trabecular pattern with 4+ cells thick; larger tumor cells than well differentiated HCC with more eosinophilic cytoplasm, distinct nucleoli, pseudoglands, bile, tumor giant cells; most common pattern in advanced HCC Poorly differentiated: Large tumor cells with hyperchromatic nuclei in compact growth pattern with rare trabeculae or bile; prominent pleomorphism, may have spindle cell or small cell areas; may not appear to be hepatocellular
, cells smaller than normal, abnormal reticulin network; minimal nuclear atypia, nuclear density 2x normal liver; commonly fatty change and pseudoglands; may resemble hepatocyte adenoma; common pattern for small hepatocellular carcinoma. Moderately differentiated: trabecular pattern with 4+ cells thick; larger tumor cells than well differentiated HCC with more eosinophilic cytoplasm, distinct nucleoli, pseudoglands, bile, tumor giant cells; most common pattern in advanced HCC. Poorly differentiated: Large tumor cells with hyperchromatic nuclei in compact growth pattern with rare trabeculae or bile; prominent pleomorphism, may have spindle cell or small cell areas; may not appear to be hepatocellular.")
25
Hepatocellular carcinoma
Note that this hepatocellular carcinoma is composed of liver cords that are much wider than the normal liver plate that is two cells thick. There is no discernable normal lobular architecture, though vascular structures are present.

26
Hepatocellular carcinoma
A, hepatocellular carcinoma, pseudoalveolar pattern B,cholangiocarcinoma

27
Hepatocellular carcinoma
Positive stains: HepPar1 (80-90%, cytoplasmic and granular), polyclonal CEA in canalicular pattern (50-90%, in better differentiated tumors), AFP (15-70%, not in small tumors), alpha-1-antitrypsin (55-93%), CEA-Gold 5 (76%), albumin mRNA ISH, CD10 (52%), transferrin, copper (7-41%), CAM 5.2 (CK 8/18), Fas, Fas ligand Note: polyclonal CEA in canalicular pattern is specific for hepatocellular carcinoma ; monoclonal CEA is usually negative Negative stains: AE1-AE3, CK7 (80%), CK13, CK19 (>90%), CK20, keratin 903 (>90%), EMA, monoclonal CEA (present in 0-10%), CD15, mucin (mucicarmine), MOC31, BerEP4 Recommended panel: p-CEA or CEA-Gold 5 or (less recommended) CD10, HepPar-1, mucicarmine or MOC31 Molecular: 50-92% hyperploid or aneuploid
, polyclonal CEA in canalicular pattern (50-90%, in better differentiated tumors), AFP (15-70%, not in small tumors), alpha-1-antitrypsin (55-93%), CEA-Gold 5 (76%), albumin mRNA ISH, CD10 (52%), transferrin, copper (7-41%), CAM 5.2 (CK 8/18), Fas, Fas ligand. Note: polyclonal CEA in canalicular pattern is specific for hepatocellular carcinoma ; monoclonal CEA is usually negative. Negative stains: AE1-AE3, CK7 (80%), CK13, CK19 (>90%), CK20, keratin 903 (>90%), EMA, monoclonal CEA (present in 0-10%), CD15, mucin (mucicarmine), MOC31, BerEP4. Recommended panel: p-CEA or CEA-Gold 5 or (less recommended) CD10, HepPar-1, mucicarmine or MOC31. Molecular: 50-92% hyperploid or aneuploid.")
28
Hepatocellular carcinoma
DD: metastatic hepatoid adenocarcinoma from stomach or lung (CK19+, CK20+, CK7-, HepPar1 negative, no cirrhosis) neuroendocrine tumors from pancreas or small bowel (similar trabecular pattern but smaller cells, inconspicuous nucleoli, stippled chromatin, no cirrhosis) poorly differentiated metastatic adenocarcinoma or cholangiocarcinoma (desmoplastic stroma, mucin+) renal cell carcinoma (RCC+, HepPar1-, biopsy may be from renal mass) Melanoma, angiosarcoma, epithelioid angiomyolipoma (spindle cell component, thick walled vessels, HMB45+, actin+, CK-) adenoma or macroregenerative nodule (no trabecular growth pattern, different clinical history, minimal atypia
 neuroendocrine tumors from pancreas or small bowel (similar trabecular pattern but smaller cells, inconspicuous nucleoli, stippled chromatin, no cirrhosis) poorly differentiated metastatic adenocarcinoma or cholangiocarcinoma (desmoplastic stroma, mucin+) renal cell carcinoma (RCC+, HepPar1-, biopsy may be from renal mass) Melanoma, angiosarcoma, epithelioid angiomyolipoma (spindle cell component, thick walled vessels, HMB45+, actin+, CK-) adenoma or macroregenerative nodule (no trabecular growth pattern, different clinical history, minimal atypia.")
29
Hepatocellular carcinoma
Hepatocellular carcinoma. A, hematoxylin and eosin stained section. B, cytoplasmic staining with Hepatocyte (40).
.")
30
Hepatocellular carcinoma
Hepatocellular carcinoma stained with pCEA. A, canalicular pattern of staining. B, canalicular-membranous pattern of immunoreactivity (40 ).
.")
31
Hepatocellular carcinoma
Hepatocellular carcinoma, focal positive staining with ά-fetoprotein

32
Hepatocellular carcinoma
A, hepatocellular carcinoma, negative staining with MOC31 B, cholangiocarcinoma, positive staining with MOC31

33
Hepatocellular carcinoma
A, hepatocellular carcinoma, negative staining with MOC31 B,cholangiocarcinoma, positive staining with MOC31

34
Hepatocellular carcinoma
A, hepatocellular carcinoma, canalicular pattern of staining with polyclonal carcinoembryonic antigen (pCEA) B, cholangiocarcinoma, positive cytoplasmic staining with pCEA C, cholangiocarcinoma, difficult pattern of pCEA to interpret with focal pattern resembling canalicular staining D, hepatocellular carcinoma, luminal pattern of staining with pCEA
 B, cholangiocarcinoma, positive cytoplasmic staining with pCEA. C, cholangiocarcinoma, difficult pattern of pCEA to interpret with focal pattern resembling canalicular staining. D, hepatocellular carcinoma, luminal pattern of staining with pCEA.")
35
Hepatocellular carcinoma
Cytology: highly cellular, polygonal tumor cells with abundant eosinophilic cytoplasm, central hyperchromatic nuclei or variable prominent nucleoli; increased nuclear to cytoplasmic ratio; often naked tumor cell nuclei;

36
Clear cell variant of hepatocellular carcinoma
Hepatocellular clear cell carcinoma. A, low-power view of tumor, capsule, and normal nontumor parenchyma. B, medium-power view, macrotrabeculae. C, high-power view, sheets of tumor cells. D and E, high-power views, macrotrabeculae, sinusoids.

37
Fibrolamellar Variant of Hepatocellular Carcinoma
Young adults years, but 30-40% in patients are less than 20 years old, no gender preference 1-5% of all hepatocellular carcinoma Not associated with hepatitis B virus, cirrhosis or metabolic abnormalities; pathogenesis unknown Better prognosis than classic HCC; 5 years survival is 60% Metastasizes to abdominal lymph nodes, peritoneum, lung Xray: central scar (similar to focal nodular hyperplasia); often calcified (uncommon with FNH) Laboratory: serum alpha fetoprotein elevated in only 10% vs. 60% of classic HCC Gross: single (75%), large (mean 13 cm), hard, scirrhous, well-circumscribed, bulging, white-brown tumor with fibrous bands throughout and central stellate scar; most cases involve left lobe, but may involve both lobes; variable bile staining, hemorrhage and necrosis
; often calcified (uncommon with FNH) Laboratory: serum alpha fetoprotein elevated in only 10% vs. 60% of classic HCC. Gross: single (75%), large (mean 13 cm), hard, scirrhous, well-circumscribed, bulging, white-brown tumor with fibrous bands throughout and central stellate scar; most cases involve left lobe, but may involve both lobes; variable bile staining, hemorrhage and necrosis.")
38
Fibrolamellar Variant of Hepatocellular Carcinoma
This neoplasm is composed of big pink cells that form trabeculae. These trabeculae are separated by fibrous stroma

39
Fibrolamellar Variant of Hepatocellular Carcinoma
Positive stains: fibrinogen (pale bodies), copper, copper-binding protein, bile, alpha-1-antitrypsin, polyclonal CEA, CAM 5.2 (CK 8/18), CK7 Negative stains: mucin (if present, call combined hepatocellular carcinoma-cholangiocarcinoma), alpha fetoprotein DD: focal nodular hyperplasia (usually 5 cm or less, fibrous stroma contain bile ductules and inflammatory cells, no bile staining grossly, no hepatocyte atypia), sclerosing variant of hepatocellular carcinoma (no oncocytes, smaller tumor cells, pseudoglandular pattern common), cholangiocarcinoma, adenosquamous carcinoma with sclerosis, metastatic carcinoma with sclerotic stroma, neuroendocrine tumors
, copper, copper-binding protein, bile, alpha-1-antitrypsin, polyclonal CEA, CAM 5.2 (CK 8/18), CK7. Negative stains: mucin (if present, call combined hepatocellular carcinoma-cholangiocarcinoma), alpha fetoprotein. DD: focal nodular hyperplasia (usually 5 cm or less, fibrous stroma contain bile ductules and inflammatory cells, no bile staining grossly, no hepatocyte atypia), sclerosing variant of hepatocellular carcinoma (no oncocytes, smaller tumor cells, pseudoglandular pattern common), cholangiocarcinoma, adenosquamous carcinoma with sclerosis, metastatic carcinoma with sclerotic stroma, neuroendocrine tumors.")
40
Hepatoblastoma Most common primary liver tumor in children (50% of liver malignancies in children) 90% occur by age 5 years, 70% by age 2 years 2/3 male Associated with hemihypertrophy (Beckwith-Wiedemann syndrome), Wilm’s tumor, glycogen storage disease, familial colonic polyposis); not associated with cirrhosis Symptoms: variable virilization due to hCG production by multinucleated giant cells Laboratory: elevated serum AFP in 75% Metastases to regional lymph nodes, lung, brain, adrenal glands, bone marrow Treatment: preoperative chemotherapy and surgery; resect lung metastases; liver transplant if unresectable Long term survival now 60-70% Prognostic factors: stage, age, sex; increase mitotic activity may confer poorer prognosis; presence of osteoid may confer favorable prognosis
, Wilm’s tumor, glycogen storage disease, familial colonic polyposis); not associated with cirrhosis. Symptoms: variable virilization due to hCG production by multinucleated giant cells. Laboratory: elevated serum AFP in 75% Metastases to regional lymph nodes, lung, brain, adrenal glands, bone marrow. Treatment: preoperative chemotherapy and surgery; resect lung metastases; liver transplant if unresectable. Long term survival now 60-70% Prognostic factors: stage, age, sex; increase mitotic activity may confer poorer prognosis; presence of osteoid may confer favorable prognosis.")
41
Hepatoblastoma Gross: tan-green, 70% solitary, well circumscribed, variable hemorrhage and cysts; mean 10 cm (range 3-20 cm), often partially encapsulated; may be calcified in prominent mesenchymal component
, often partially encapsulated; may be calcified in prominent mesenchymal component.")
42
Hepatoblastoma This neoplasm is composed of a mixture of two cell types. Some neoplastic hepatocytes are arranged in irregular laminae (fetal) while others grow in a more embryonal pattern.
 while others grow in a more embryonal pattern.")
43
Hepatoblastoma Epithelial type (56%) Fetal pattern (31%): tumor cells in trabeculae 2-3 cells thick (resembling fetal liver), separated by sinusoids lined by CD34+ endothelial cells; tumor cells are same size or smaller than in non-neoplastic liver; distinct cell membranes, uniform, polyhedral, slightly higher nuclear/cytoplasmic ratio, inconspicuous nucleoli, may contain bile; minimal pleomorphism, no/rare mitotic figures;; no portal tracts, bile ducts or ductules; reduced reticulin Embryonal pattern (19%): sheets, ribbons, rosettes, papillary patterns or trabeculae of variable thickness with immature appearance, discohesive small cells with poorly defined cell borders, basophilic cytoplasm, high N/C ratio, prominent nucleoli, coarse chromatin, increased mitotic figures; extramedullary hematopoiesis, necrosis and vascular lakes are common; no fat, glycogen or bile Macrotrabecular pattern (3%): frequent trabeculae > 10 cells thick throughout the tumor, variable cytologic features Small cell undifferentiated pattern (3%): discohesive sheets of small uniform cells with minimal cytoplasm, indistinct cell borders, oval hyperchromatic nuclei, variable prominent nucleoli and increased mitotic figures; resembles small cell carcinoma at other sites; may have mucoid stroma, hyalinized septae; tumor cells are keratin+, bile- Mixed epithelial and mesenchymal type (44%) mixture of fetal/epithelial and mesenchymal cell types; teratoid (34%) or not (10%); mesenchymal component has spindle-oval cells with minimal cytoplasm, frequent osteoid, fibrous septa, myxoid zones, hemorrhage and necrosis; teratoid features are keratinized squamous epithelium, intestinal epithelial, skeletal muscle, mature bone and cartilage, melanin and neuroectodermal structures
: tumor cells in trabeculae 2-3 cells thick (resembling fetal liver), separated by sinusoids lined by CD34+ endothelial cells; tumor cells are same size or smaller than in non-neoplastic liver; distinct cell membranes, uniform, polyhedral, slightly higher nuclear/cytoplasmic ratio, inconspicuous nucleoli, may contain bile; minimal pleomorphism, no/rare mitotic figures;; no portal tracts, bile ducts or ductules; reduced reticulin. Embryonal pattern (19%): sheets, ribbons, rosettes, papillary patterns or trabeculae of variable thickness with immature appearance, discohesive small cells with poorly defined cell borders, basophilic cytoplasm, high N/C ratio, prominent nucleoli, coarse chromatin, increased mitotic figures; extramedullary hematopoiesis, necrosis and vascular lakes are common; no fat, glycogen or bile. Macrotrabecular pattern (3%): frequent trabeculae > 10 cells thick throughout the tumor, variable cytologic features. Small cell undifferentiated pattern (3%): discohesive sheets of small uniform cells with minimal cytoplasm, indistinct cell borders, oval hyperchromatic nuclei, variable prominent nucleoli and increased mitotic figures; resembles small cell carcinoma at other sites; may have mucoid stroma, hyalinized septae; tumor cells are keratin+, bile- Mixed epithelial and mesenchymal type (44%) mixture of fetal/epithelial and mesenchymal cell types; teratoid (34%) or not (10%); mesenchymal component has spindle-oval cells with minimal cytoplasm, frequent osteoid, fibrous septa, myxoid zones, hemorrhage and necrosis; teratoid features are keratinized squamous epithelium, intestinal epithelial, skeletal muscle, mature bone and cartilage, melanin and neuroectodermal structures")
44
Epithelioid Hemangioendothelioma
Malignant endothelium derived neoplasm with intermediate clinical course between hemangioma and angiosarcoma Hepatic EH is considered a neoplasm of unpredictable malignant potential: the metastatic rate of hepatic EH was 27%, and 43% of the patients ultimately died of their disease. Mean age 47 years, but occurs at any age, 60% women No predisposing factors FNA not recommended as even small biopsies can be misleading

45
Epithelioid Hemangioendothelioma
Most of the lobe is occupied by a ill-defined, mottled tumorous mass (arrowheads) corresponding to EH. Note a cavernous hemangioma (arrow).
 corresponding to EH. Note a cavernous hemangioma (arrow).")
46
Epithelioid Hemangioendothelioma
The tumor forms a relatively circumscribed mass with a prominent fibrous stoma with myxohyaline areas. In some areas, the tumor grows as strands and cords of cells. Here the tumor cells are rounded to slightly spindled. Some of the cells contain prominent intracytoplasmic vacuoles. In other areas the tumor cells line open channels filled with erythrocytes. Here the tumor cells are flat and lack tufting or pleomorphism.

47
Epithelioid Hemangioendothelioma
Positive stains: factor VIII related antigen and CD34 for vacuoles, CD31, trichrome and elastic stains accentuate obliteration of hepatic venules and hepatic vein branches, NSE EM: Weibel-Palade bodies, intermediate filaments DD: signet ring adenocarcinoma, scirrhous cholangiocarcinoma, sclerotic hepatocellular carcinoma, sclerosed hemangioma (well circumscribed, no venous invasion, no atypia), leiomyosarcoma, chondrosarcoma, metastatic tumor from lung or elsewhere, angiosarcoma (different stroma, more atypia)
, leiomyosarcoma, chondrosarcoma, metastatic tumor from lung or elsewhere, angiosarcoma (different stroma, more atypia)")
48
Angiosarcoma Rare (10-30 annual cases in US), but most common hepatic primary sarcoma in adults (2% of all primary liver tumors) 75% men, usually age 50+ years; rare in children Causes: 25-42% associated with exposure to vinyl chloride, arsenic, Thorotrast (thorium dioxide) or androgen steroids; rarely associated with copper sulfate, estrogenic steroids, phenelzine, radiotherapy, chemotherapy, hereditary hemochromatosis Patients with exposure to vinyl chloride or Thorotrast may have synchronous cholangiocarcinoma or hepatocellular carcinoma Most patients die within 6 months from hepatic failure, intraabdominal bleeding; metastasizes widely, often to lung
 or androgen steroids; rarely associated with copper sulfate, estrogenic steroids, phenelzine, radiotherapy, chemotherapy, hereditary hemochromatosis. Patients with exposure to vinyl chloride or Thorotrast may have synchronous cholangiocarcinoma or hepatocellular carcinoma. Most patients die within 6 months from hepatic failure, intraabdominal bleeding; metastasizes widely, often to lung.")
49
Angiosarcoma Gross: multicentric, diffusely infiltrative, hemorrhagic and gray-white solid nodules with blood filled cavities Micro: tumor composed of infiltrative, freely anastomosing vascular channels; tumor cells grow along sinusoids adjacent to hepatic cords; frequent mitotic activity; also epithelioid cells with abundant cytoplasm and prominent nucleoli Positive stains: CD34, CD31, factor VIII related antigen DD: reactive disorders, hepatocellular carcinoma, Kaposi’s sarcoma , peliosis hepatis, epithelioid hemangioendothelioma

50
Angiosarcoma Figure 1. FNA specimen showing spindle cells with fine cytoplasmic processes and vascular lumen (microacinar) formation Figure 2. FNA specimen showing focally prominent intracytoplasmic vacuoles Figure 3. FNA specimen demonstrating an intracytoplasmic lumen containing fragmented red blood cell by-products, which stained densely basophilic) Figure 4. Discohesive anastomosing vascular channels lined by plump malignant spindle cells.
 Figure 4. Discohesive anastomosing vascular channels lined by plump malignant spindle cells.")
51
Undifferentiated Sarcoma
Also called embryonal sarcoma, malignant mesenchymoma, mesenchymal sarcoma Usually ages 6-10 years, rare in adults, 10% of pediatric hepatic tumors (#3 after hepatoblastoma and hepatocellular carcinoma) Often aneuploid Appears to be a primitive mesenchymal neoplasm with possible foci of differentiated sarcoma Presents with abdominal mass, fever, pain, normal serum AFP Most patients die within 2 years due to direct extension; often metastasizes to lung, pleura, peritoneum Treatment: complete resection
 Often aneuploid. Appears to be a primitive mesenchymal neoplasm with possible foci of differentiated sarcoma. Presents with abdominal mass, fever, pain, normal serum AFP. Most patients die within 2 years due to direct extension; often metastasizes to lung, pleura, peritoneum. Treatment: complete resection.")
52
Undifferentiated sarcoma
Gross: cm, solitary, well-demarcated, soft tumor with cystic, gelatinous, hemorrhagic and necrotic foci Micro: variably cellular tumor with anaplastic, spindled / oval cells with hyaline globules and ill-defined borders within pseudocapsule; nuclei have stippled chromatin, inconspicuous nucleoli; variably myxoid stroma with numerous thin-walled veins

53
Bile Duct Tumors Bile Duct Adenoma Biliary Cystadenoma
Biliary Cystadenocarcinoma Cholangiocarcinoma (intrahepatic)
")
54
Bile Duct Adenoma Incidental finding, although often confused with adenocarcinoma Usually adults > 40 years old, no gender preference Benign Gross: well-circumscribed but unencapsulated, firm, gray-white, tan, subcapsular nodules Micro: simple tubular ducts with small or indistinct lumina; epithelium has abundant cytoplasm and pale nuclei compared to interlobular bile ducts in adjacent liver; variable fibrous stroma, granulomas, calcification, inflammatory cells; usually no cystic change, no cytoplasmic or intraluminal bile, no atypia, no mitotic figures, no angiolymphatic invasion Positive stains: mucin (intracytoplasmic), CEA, EMA, keratin, PAS highlights basement membrane DD: cholangiocarcioma, adenocarcinoma
, CEA, EMA, keratin, PAS highlights basement membrane. DD: cholangiocarcioma, adenocarcinoma.")
55
Biliary Cystadenoma 5% of all hepatic solitary cysts
95% occur in women, mean age 45 years 84% are intrahepatic, Associated with polycystic liver disease, abnormal hepatobiliary anatomy Usually slow growing with good prognosis after surgical excision, although 25% have coexisting malignancy Complications: intracystic hemorrhage, bacterial infection, rupture Also associated with borderline or malignant lesions Laboratory: elevated CA 19-9 (in cases with ovarian type stroma) and CEA in cyst fluid and serum Xray: calcification in 20% (resemble echinococcal cyst)
 and CEA in cyst fluid and serum. Xray: calcification in 20% (resemble echinococcal cyst)")
56
Biliary Cystadenoma Gross: encapsulated, solitary, mean 15 cm), usually mucinous, multilocular by definition); contains up to several liters of fluid; smooth inner surface Micro: mucinous - lined by single layer of columnar-cuboidal mucinous epithelium with basal nuclei and apical mucin; serous - lined by bland, flat to cuboidal cells with clear, glycogen-rich cytoplasm, no spindle cell stroma
, usually mucinous, multilocular by definition); contains up to several liters of fluid; smooth inner surface. Micro: mucinous - lined by single layer of columnar-cuboidal mucinous epithelium with basal nuclei and apical mucin; serous - lined by bland, flat to cuboidal cells with clear, glycogen-rich cytoplasm, no spindle cell stroma.")
57
Biliary Cystadenocarcinoma
<100 cases reported Usually ages 50+ years; equal gender frequency Usually mucinous, often associated with cystadenoma Tumors more indolent in women with ovarian-like stroma, more aggressive in men May have intraabdominal dissemination as terminal event Cysts represent dilated intrahepatic bile ducts invaded by tumor cells Survival: 50% at 4 years, better prognosis if spindle-cell stroma

58
Biliary Cystadenocarcinoma
Left hepatic lobe (lateral segment) is replaced by multiple cystic lesions (large arrows) and a solid lesion (arrow heads). The largest cyst is 4 cm in diameter. The cysts are mucinous. Intrahepatic biliary tree of the right lobe also shows significant dilatation (small arrows).
 is replaced by multiple cystic lesions (large arrows) and a solid lesion (arrow heads). The largest cyst is 4 cm in diameter. The cysts are mucinous. Intrahepatic biliary tree of the right lobe also shows significant dilatation (small arrows).")
59
Biliary Cystadenocarcinoma
Micro: papillary or tubulopapillary neoplasm of malignant cells lining fibrovascular cores that project into cystic cavities malignant diagnosis is based on stromal invasion

60
Cholangiocarcinoma (intrahepatic)
Also called bile duct carcinoma 10% of primary liver cancers High prevalence in southeast and eastern Asia 10-20% are associated with cholangitis due to autosomal dominant polycystic disease, congenitally dilated hepatic ducts (Caroli’s disease), congenital hepatic fibrosis, infection by liver flukes, Thorotrast, anabolic steroids, intrahepatic lithiasis (5-10% of these patients), primary sclerosing cholangitis (7-42% of these patients) Diagnosis of exclusion (must rule out metastatic adenocarcinoma) Usually age 60+ years; no gender preference Laboratory: normal AFP Poor prognosis; death usually within 6 months 50-75% metastasize to regional lymph nodes, lungs, vertebrae, adrenals, brain, elsewhere at autopsy
, congenital hepatic fibrosis, infection by liver flukes, Thorotrast, anabolic steroids, intrahepatic lithiasis (5-10% of these patients), primary sclerosing cholangitis (7-42% of these patients) Diagnosis of exclusion (must rule out metastatic adenocarcinoma) Usually age 60+ years; no gender preference. Laboratory: normal AFP. Poor prognosis; death usually within 6 months % metastasize to regional lymph nodes, lungs, vertebrae, adrenals, brain, elsewhere at autopsy.")
61
Cholangiocarcinoma (intrahepatic)
Gross: solitary, 7-10 cm, multinodular or diffuse small nodules < 1 cm; gray-white and firm; often hepatomegaly and satellite nodules; rarely cirrhosis; rarely bile stained; may invade portal vein

62
Cholangiocarcinoma (intrahepatic)
Patterns signet ring adenosquamous osteoclast giant cell sarcomatous colloid, mucoepidermoid, rhabdoid, clear cell, lymphoepithelioma-like

63
Cholangiocarcinoma (intrahepatic)
The carcinoma has a glandular appearance that is most consistent with cholangiocarcinoma. Cholangiocarcinomas do not make bile, but the cells do make mucin, and they can be almost impossible to distinguish from metastatic adenocarcinoma on biopsy or fine needle aspirate.

64
Cholangiocarcinoma (intrahepatic)
54-year-old woman, history of common duct stricture. Adenocarcinoma (x200). Note marked nuclear crowding, nucleomegaly, anisonucleosis, hyperchromasia and prominent nucleoli.
. Note marked nuclear crowding, nucleomegaly, anisonucleosis, hyperchromasia and prominent nucleoli.")
65
Cholangiocarcinoma (intrahepatic)
Positive stains: mucin (almost always), CEA (cytoplasmic and luminal, not canalicular), keratin 903 (74%), CK7 (90-96%), CK19 (84%), CK20 (30-70%) Negative stains: AFP Molecular: Kras mutations DD: metastatic adenocarcinoma from pancreas, extrahepatic biliary tree, breast, colon (CK7-/CK20+ [strong]) or gallbladder (must exclude based on clinical and radiographic findings); hepatocellular carcinoma with ductular differentiation, epithelioid hemangioendothelioma (vascular markers+, mucin-), benign bile duct proliferations (smaller, no atypia, incidental)
, CEA (cytoplasmic and luminal, not canalicular), keratin 903 (74%), CK7 (90-96%), CK19 (84%), CK20 (30-70%) Negative stains: AFP. Molecular: Kras mutations. DD: metastatic adenocarcinoma from pancreas, extrahepatic biliary tree, breast, colon (CK7-/CK20+ [strong]) or gallbladder (must exclude based on clinical and radiographic findings); hepatocellular carcinoma with ductular differentiation, epithelioid hemangioendothelioma (vascular markers+, mucin-), benign bile duct proliferations (smaller, no atypia, incidental)")
66
Cholangiocarcinoma (intrahepatic)
Immunostains demonstrate that the tumor cells are diffusely CK7 positive, partially CK20 positive; and PSA, as well as Heppar-1 negative in support of a pancreato-biliary origin. Mucin stain is focally positive.

67
Case 1

68
GIST

69
Case 2

70
Neuroendocrine Carcinoma

71
Case 3 This is a 77 year-old male with a liver mass.

72
Metastatic MM

73
Case 4: 74 yo Asian female with liver mass

79
Follicular dendritic cell sarcoma

Similar presentations






>")














>")

