Download presentation
Presentation is loading. Please wait.

1
Cardiosurgery - Skopje Differential diagnosis and treatment of acute coronary disease Special Hospital for Surgical Diseases “Filip II” - Skopje, Macedonia Milev Ivan MD June, 2009

2
Cardiosurgery - Skopje

3
Acute coronary syndrome defininiton Chest pain is a major symptom of acute coronary disease or syndrome (ACS). ACS includes non stabile angina (NA), myocardial infarction (MI) without ST elevation (NSTEMI) and MI with ST elevation (STEMI). Erosion or rupture of unstable atherosclerotic plaque, and creation of thrombus formation The limitation of flow, oxygenation of myocardium and collateral circulation are major determinants of clinical signs.
, myocardial infarction (MI) without ST elevation (NSTEMI) and MI with ST elevation (STEMI). Erosion or rupture of unstable atherosclerotic plaque, and creation of thrombus formation The limitation of flow, oxygenation of myocardium and collateral circulation are major determinants of clinical signs..")
4
Cardiosurgery - Skopje Development of Atherosclerotic Plaques Normal Fatty streak Foam cells Lipid-rich plaque Lipid core Fibrous cap Thrombus

5
Cardiosurgery - Skopje Lumen Fibrous Cap Lipid Core Fibrous Cap Lumen Vulnerable Plaque Stable Plaque Thick fibrous cap Smooth muscle cells: more extracellular matrix Lipid-poor plaque Thin fibrous cap Inflammatory cell infiltrates: proteolytic activity Lipid-rich plaque Libby P. Circulation. 1995;91:2844-2850. Vulnerable vs Stable Atherosclerotic Plaques

6
Cardiosurgery - Skopje Thrombosis Influences the Severity of a Cardiovascular Event Nonocclusive thrombusOcclusive thrombus Unstable angina Non—Q-wave MI Q-wave MI Sudden death Minor plaque disruption High flow Low thrombotic tendency Major plaque disruption Low flow or vasospasm Thrombotic tendency Kullo IJ, et al. Ann Intern Med. 1998;129:1050-1060. Factors favoring thromb.Factors limiting thromb.:

7
Cardiosurgery - Skopje Other reasons for NA and NSTEMI Non-oclusive thrombus Dynamic obstruction (coronary spasms) Infection -inflammation with increase markers (CRP) -infection with Chlamidia pneumonie, Helicobacter pylori, cytomegalovirusi, herpes simplex virus
 Infection -inflammation with increase markers (CRP) -infection with Chlamidia pneumonie, Helicobacter pylori, cytomegalovirusi, herpes simplex virus")
8
Cardiosurgery - Skopje ECG changes vs risqué of death or MI- epidemiology death or IM 30-days6- months1-year ST elevation9,4%12,3%16,1% ST depression10,5%15,45%18,1% ST elevacija and depression 12,4% 15,7%25,6% T wave inversion5,5%8,1%13,6%

9
Cardiosurgery - Skopje Chest pain - origin acute aortic dissection (AAD) pulmonary embolism pericarditis mitral valve prolaps chest pain in obstructive cardiomiopathy primary pulmonary hypertension *consider non-cardiac disesases of pleura, mediastinum and abdomen
 pulmonary embolism pericarditis mitral valve prolaps chest pain in obstructive cardiomiopathy primary pulmonary hypertension *consider non-cardiac disesases of pleura, mediastinum and abdomen")
10
Cardiosurgery - Skopje Chest pain-origin

11
Cardiosurgery - Skopje

13
Acute coronary syndrome - the importance Urgent presentation Needs high level of health organization Great morbidity and mortality rate Increasing of percentage of pts with unstable angina and NSTEMI in recent years

14
Cardiosurgery - Skopje ACSy - triggers hypertension, tachycardia, hard work –the intracoronary changes in hemodynamic state. Peak - early in the morning (sympaticus) Factors inside the plaque Emotional stress
 Factors inside the plaque Emotional stress.")
15
Cardiosurgery - Skopje Diagnostic of coronary disease Diagnostic of coronary disease

16
Cardiosurgery - Skopje ECG Standard 12-lead ECG is the best test Additional leads V4R-V6R (inferior IM) for RV assessment. V7-V9 posterior leads Continious recording every 20 sec. New LBBB, ST depression 1 mm V1 - V3, ST elevation > od 2 mm suggest IM

17
Cardiosurgery - Skopje Laboratory markers Two folds increasing of CK after 6 h, peak 24 h. CK-MB sensitivity 90%, increase 6 h. Troponin I /T is more specific. Activity rise after 6 h, peak 12-24 h, and high level in serum up to 7-10 days.

18
Cardiosurgery - Skopje Echocardiography Assessment of wall motion Sensitivity of acute IM is 93%, specificity 53% Can not distinguish acute from previous IM

19
Cardiosurgery - Skopje

20
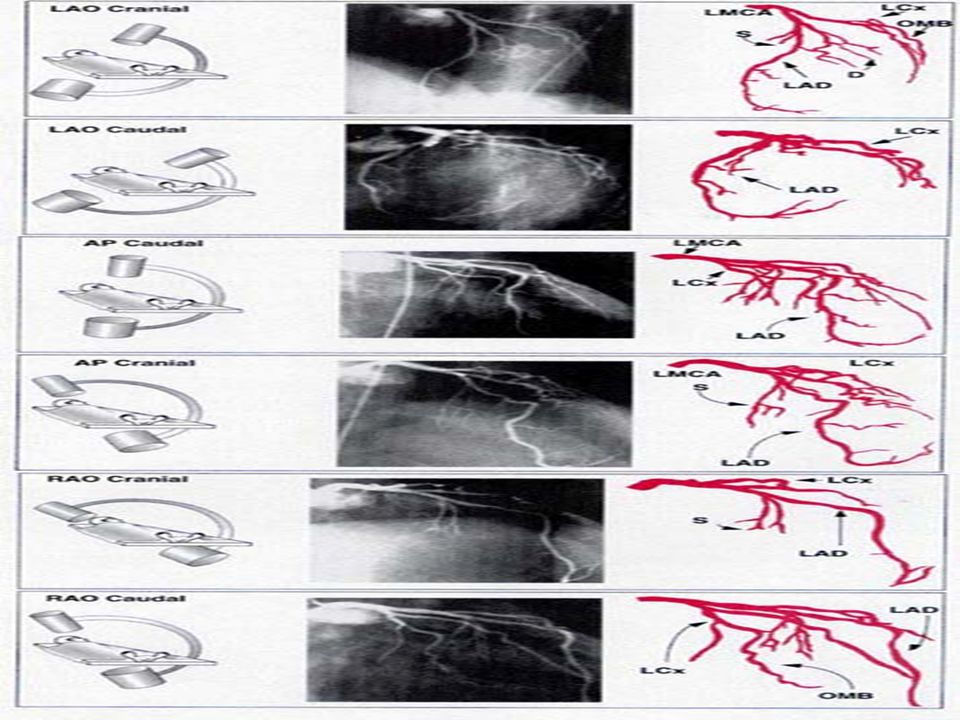
Coronarography

23
Action- time is short, move swiftly & decide... Door (events prior to arrival) Data – actual (obtain ECG, Lab) Decision (AMI & decide Th) Drug (Fibrinolytic or passing Angioplasty Cath) Triage ID AMI, Immediate Cardio consult
 Data – actual (obtain ECG, Lab) Decision (AMI & decide Th) Drug (Fibrinolytic or passing Angioplasty Cath) Triage ID AMI, Immediate Cardio consult.")
24
Cardiosurgery - Skopje EKG fibrinolytic Therapy eligibility ST elevation 1mm+ in 2 or more limb leads & 2mm+ in 2 or more contiguous precordial leads, 2-6 hours before OR new or presumed new LBBB No benefit in ischemic pt who lack above EKG findings LBBB + AMI = poorer outcome due to likely proximal LAD occlusion, putting signif. portion LV in ischemic jeopardy DO NOT USE in ST-depression... signif. poorer outcomes!!! Remember age is NO longer excluder, but age > 75 ICH

25
Cardiosurgery - Skopje When TO & When NOT TO Active Diabetic Retinopathy... strong relative C/I risk blindness DM pts + AMI 2X more likely to DIE CPR > 10 minutes long or extensive chest trauma from CPR Hemithorax/cardiac tamponade IM > 12 hours before Prior Stroke/TIA, major risk for ICH, relative C/I, prior Hemorrhagic stroke ABSOLUTE C/I Prior MI in setting AMI; 26% mortality even if prior fibrinolytics th

26
Cardiosurgery - Skopje When TO & When NOT TO Recent Surgery/Trauma/GI Bleed w/in 10 days is absolute C/I Women menses w/ AMI consider use; excessVag bleeding after Fibrinolytics CTRL w/ Vag packing compressible site of bleeding GI bleed in 10 days Absolute C/I HTA; SystBP > 180 or Diast.BP 110 Significant liver dysfunction

27
Cardiosurgery - Skopje Our results (2005-2009,n=115) Differential diagnosis was confirmed with clinical signs, repeated ECG, serum level of cardiac markers (troponin I,T), echocardiography and finaly with coronarography.
 Differential diagnosis was confirmed with clinical signs, repeated ECG, serum level of cardiac markers (troponin I,T), echocardiography and finaly with coronarography.")
28
Cardiosurgery - Skopje Results (2005-2009)
")
29
Cardiosurgery - Skopje Results (2005-2009)
")
30
Cardiosurgery - Skopje Case report (2005-2009)
")
31
Cardiosurgery - Skopje Case report(2005-2009)
")
32
Cardiosurgery - Skopje Case report (2005-2009)
")
33
Cardiosurgery - Skopje Catheterisation laboratory – Filip II 2000-2009 Ma y 2005 - May 2009: -802 intervention -Coronary intervention: 690 pat. -Intervent. of congenital anomalies: 104 pat. -Carotid stenting: 5 pat -Peripheral stenting: 3 pat.

34
Cardiosurgery - Skopje Coronary intervention May 2005-May 2009 690 PCI -treatment : -Out patients treatment: 651(94.3%) patients -Hospital treatment (more than 24h): 39(5.9%) patients
 patients -Hospital treatment (more than 24h): 39(5.9%) patients")
35
Cardiosurgery - Skopje Coronary intervention May 2005-May 2009 690 PCI - approach : -TRA: 673 (97.5%) pat. -TUA: 11 (1.5%) pat. -TFA: 3 (0.6%) pat. -TBA: 2 (0.4 %) pat.
 pat. -TFA: 3 (0.6%) pat. -TBA: 2 (0.4 %) pat..")
36
Cardiosurgery - Skopje Conclusion Time from begining of chest pain to reperfusion / D2B is a major factor in treatment of pts with ACS. Early diagnosis, urgent transport to PCI centar, early begining of fybrinolitic therapy and early differential diagnosis is essential in treatment of ACS pts and decreasing of mortality.

Similar presentations