Download presentation
Presentation is loading. Please wait.

1
LTC Dr. Ahmed Humaid Emergency Physician Consultant MD, CCFP(EM) Zayed Military Hospital
 Zayed Military Hospital")
2
The information presented is solely that of the author and does not represent the official views or policies of the UAE ARMED FORCES. The Presenter has no Financial interest in any systems or devices discussed in this presentation.

3
INTRODUCTION OVERVIEW OF SIMULATION WHY IS MEDICAL SIMULATION ? VALIDITY AND RELIABILITY? CRITICAL CARE SIMULATION APPLICATION CATEGORIES CONCLUSIONS REFERENCES

4
“Necessity is the mother of invention” Definition: “Any training device that duplicates artificially the conditions likely to be encountered in an operation ”

5
WW II Horse Simulator

6
Military Contributions to Simulation Advances? “blue box” flight trainer The military was a major impetus in the transfer of modeling and simulation technology to medicine.

7
Mid-1990s, the gaming industry surpassed the military! Today, military flight simulators are expensive but prove to be cost- effective

9
Introduction of HPS “Human Patient Simulator” toward the end of the 20th century. Delayed acceptance of med simulation. Why? –skepticism, lack of communication, and the burden of proof. Widespread past decade ONLY: –Standardized Patients (SPs). – Virtual Reality (VR) – Mannequins.
. – Virtual Reality (VR) – Mannequins..")
10
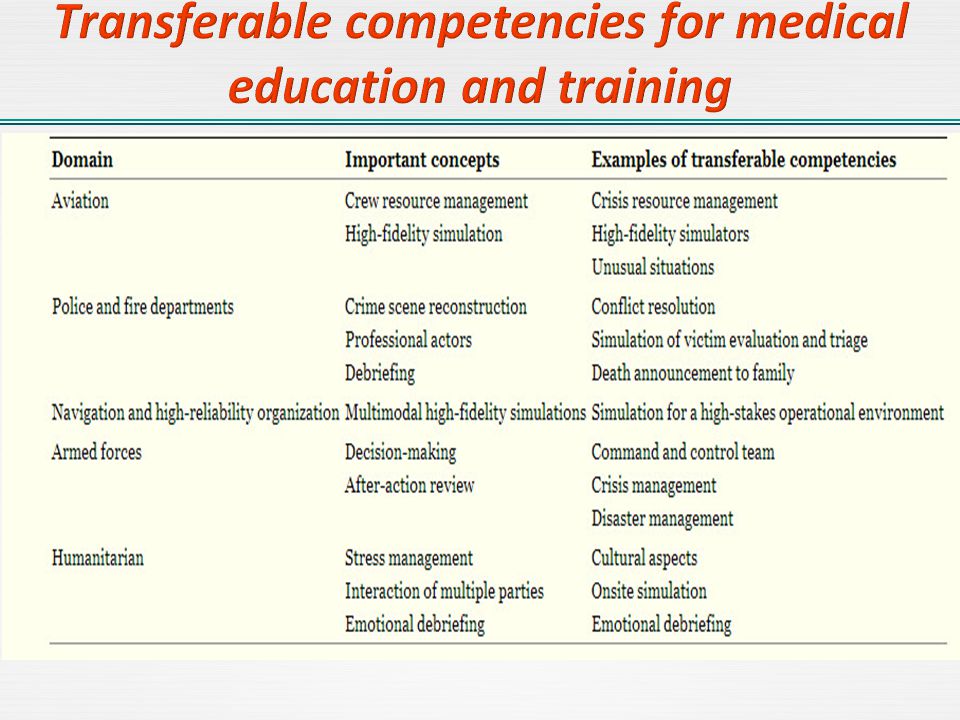
What are the similarities between healthcare and aviation? –Complex industries –Errors can be fatal –Crisis management is important –Errors are preventable –Aviation achieved high level of safety. Healthcare has not.

11
"To Err is Human...“ –Institute of Medicine Report, 1999 estimated 44,000 to 98,000 deaths annually from adverse events. –Patient Safety is paramount in Medicine Practice. – KPI improvement solutions and innovations.

12
Teamwork Communication Leadership skills Situational awareness Declaring an emergency Human error / Fixation

13
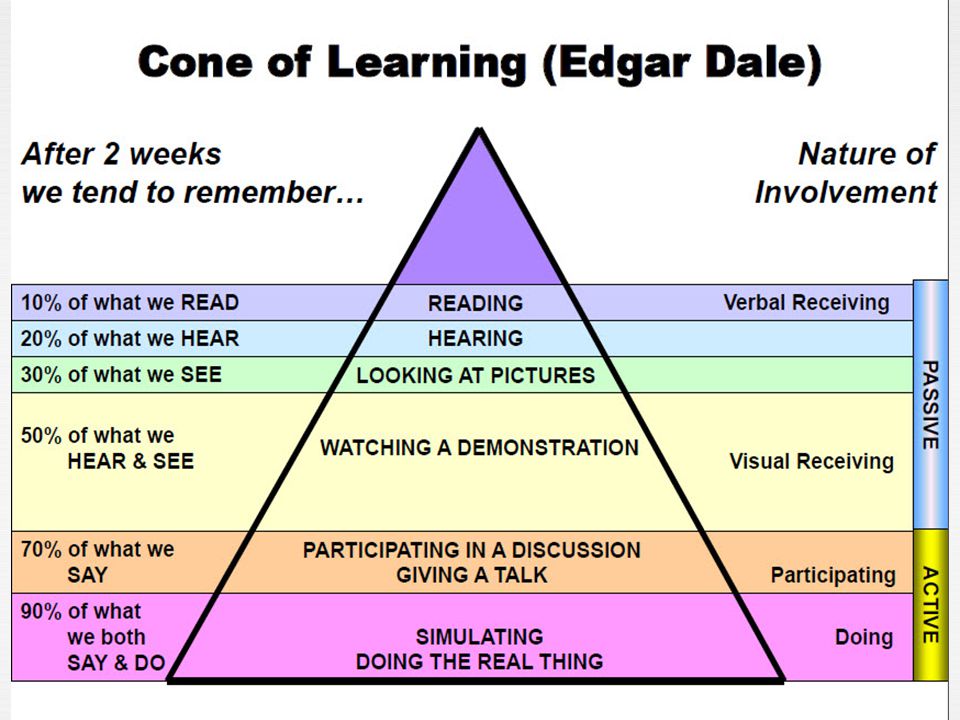
“See one, Do one, Teach one”

15
“See one, PRACTICE MANY, DO one”

16
…“The greatest power of virtual reality is the ability to try and fail without consequence to animal or patient. It is only through failure—and learning the cause of failure—that the true pathway to success lies” This would be best applied to high fidelity simulation technologies that of total immersion in reality.

19
There was a greater than 10-fold increase in the annual prevalence of simulation-related publications this decade compared with the 1990s. Gaba: “No industry in which human lives depend on the skilled performance of responsible operators has waited for the unequivocal proof of the benefit of simulation before embracing it” Validity and reliability data have been partially successful.

21
Feedback 47% Most important feature Feedback 47% Most important feature Repetitive Practice 39% Key Feature Repetitive Practice 39% Key Feature Range of Task Difficulty Level 14% Important variable in SBME Range of Task Difficulty Level 14% Important variable in SBME Multiple Learning Strategies 10% Adaptable Multiple Learning Strategies 10% Adaptable Curriculum integration 25% Essential feature Curriculum integration 25% Essential feature Capture clinical Variation 10% Defined Outcome 9% Controlled Environment 9% Individualized Learn 9% Simulator Validity 3% Effective Learning.

23
PC-based Interactive Virtual Reality and Multimedia ex. ORCA System and TC3 games. Digitally Enhanced Mannequins. Ex. Combat HAL, CAESER.

24
Virtual Workbenches for task trainers activities ex. Surgical Cut Suits. Total Immersion Virtual Reality “TIVR” for hybrid activities in the battlefield ex. Hybrid Simulation, Haptic Simulation and Avatar.

26
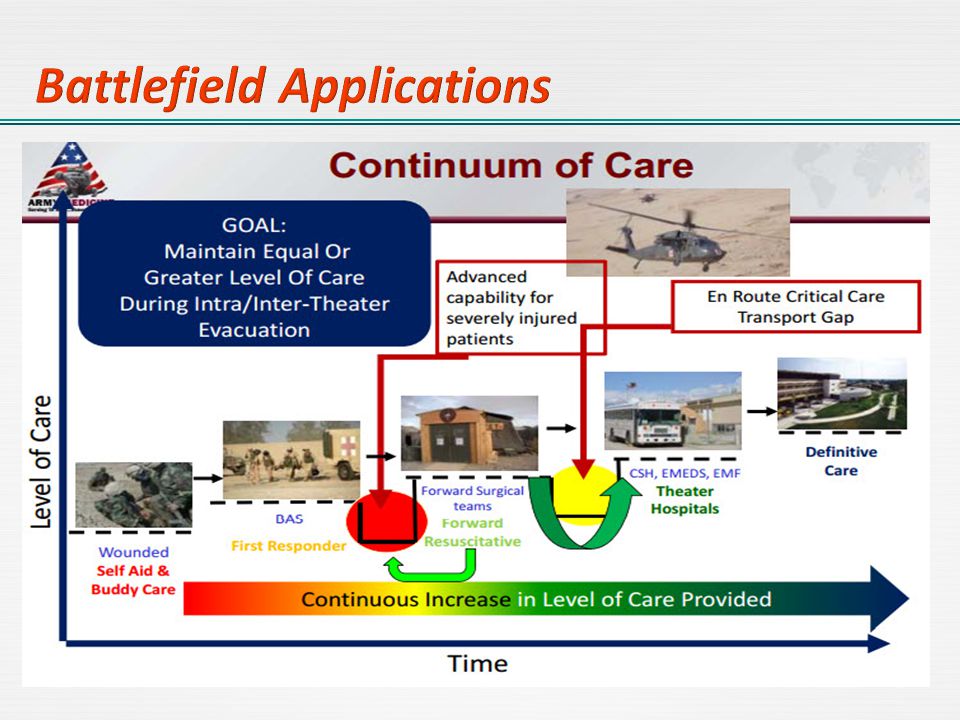
CSH “Combat Support Hospital” CCP “Casualty Collection Point” BAS “Battalion Aid Station” POI “Point Of Injury” Wartime Zone FST “Forward Surgical Team” HFS Battlefield Applications.

28
Simulated Clinical Experiences (SCEs) ‐ for tactical medicine, emergency medicine and disaster management Simulated Wound Kit ‐ Wound Effects and Moulages. Dehydrated sniperMultiple GSW

29
Simulation Debriefing and performance assessment Monitoring and case management

30
Cubic’s virtual P5CTS virtual fighter jet trainer.

31
Battlefield Military Medical Simulation is cost-effective for improving knowledge, skills and behaviors among different level of learners. If applied with right conditions. The cost of these breakthrough innovations should be weighed against the outcome, the impact of it’s application and transferable competencies. learning space is important to manage, monitor, feedback, schedule courses and maintain resources.

32
Importance of “Deliberate Practice” concept implementation. Battlefield Military Medical Education Based Simulation is a truth that can mitigate errors and improve performance in real scenarios. Medical Simulation and Modeling researches are still advancing to address it’s values, validity and reliability. Future are promising to advance the innovations in Military Medical Simulation especially in Battlefield.

33
Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systemic review. Med Teach 2005;27:10-28 Testing internal consistency and construct validity during evaluation of performance in a patent simulator. Anesthesia Annals 1998;86:1160-4. Tarver S. Anesthesia simulators: concepts and applications. Am J Anesthesia 1999;26:393-6. High Fidelity medical simulation in the difficult environment of a helicopter: feasibility, self-efficacy and cost Stewart W Wright, Christopher J Lindsell, […], and Gail Heimburger

Similar presentations

















>")





