Download presentation
Presentation is loading. Please wait.

1
Recurrent Aphthous Ulcer
Etiology: Local altered immune response. Systemic etiologies include nutritional deficiencies (iron, B6, B12), diabetes mellitus, inflammatory bowel disease, immunosuppression. Biopsy will rule out other vesiculoulcerative disease.
, diabetes mellitus, inflammatory bowel disease, immunosuppression. Biopsy will rule out other vesiculoulcerative disease.")
2
Recurrent Aphthous Ulcer
Appearance: Minor aphthous ulcer: <0.6 cm shallow ulceration with gray pseudomembrane and erythematous halo on non-keratinized mucosa. Major aphthous ulcer: >0.5 cm ulcer, more painful, lasting several weeks to months; will scar.

3
Recurrent Aphthous Ulcer
Differential Diagnosis: Herpes simplex virus. Chemical/traumatic ulcer Vesiculoulcerative diseases Squamous cell carcinoma Treatment: Topical analgesics Topical steroids

5
Inflammatory Conditions (Denture Related of the Oral Mucosa)
Inflammatory papillary hyperplasia Epulis fissurata (inflammatory fibrous dysplasia) Candidiasis
 Candidiasis.")
6
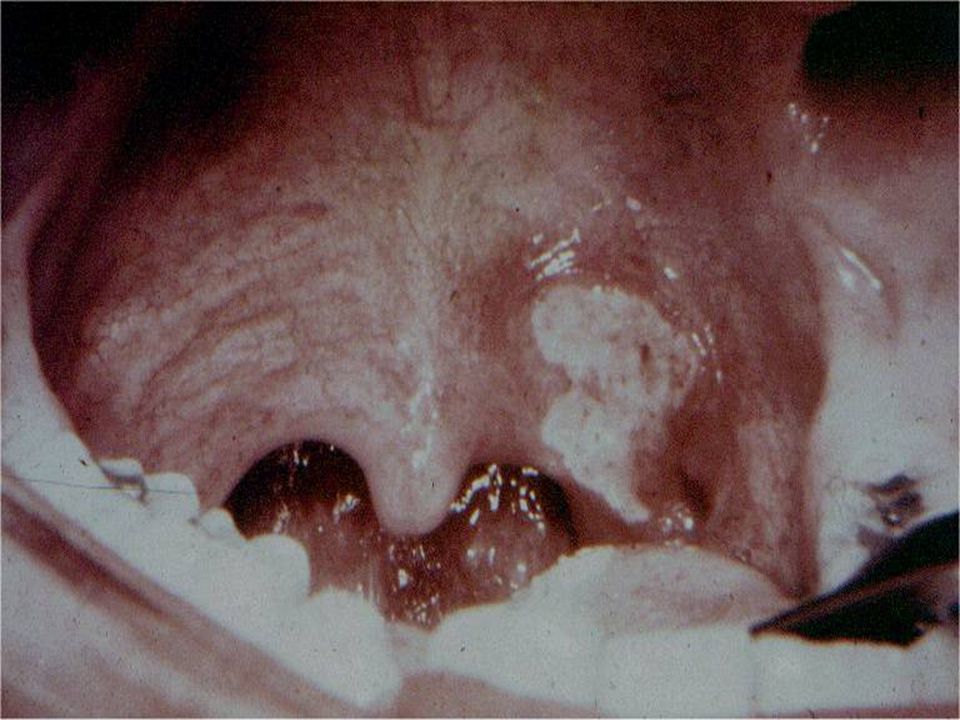
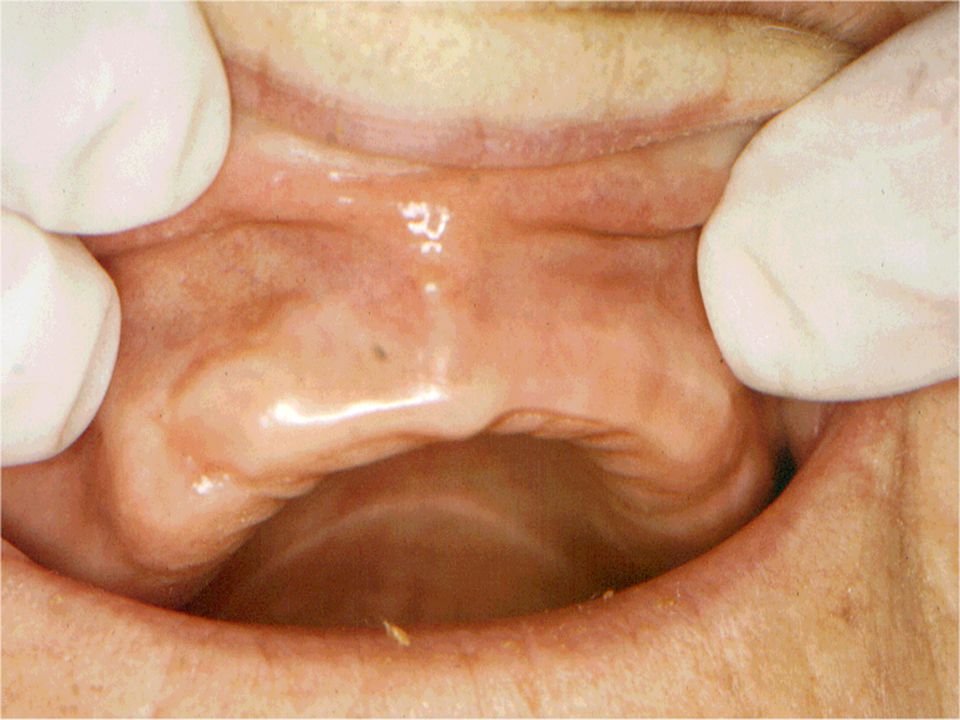
Inflammatory Papillary Hyperplasia
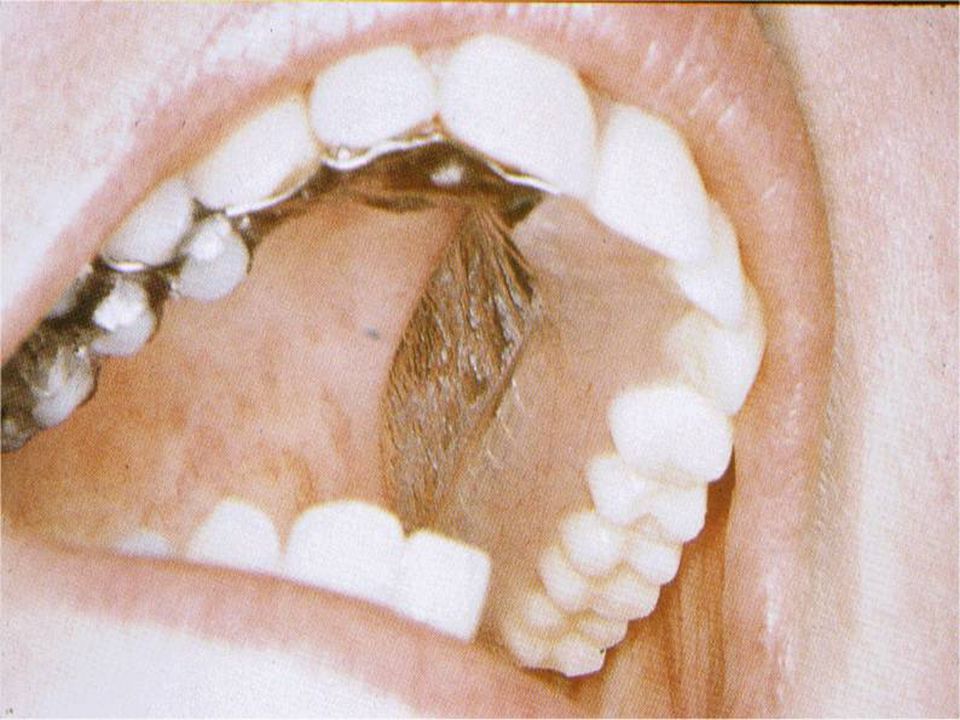
Etiology: Poorly fitting denture Occurs in more than 50% of Denture Wearers Appearance: Multiple small polypoid or papillary lesions. Typically on hard palate, that produces a cobblestone appearance.

7
Inflammatory Papillary Hyperplasia
Etiology: Poorly fitting denture Occurs in more than 50% of Denture Wearers Appearance: Multiple small polypoid or papillary lesions. Typically on hard palate, that produces a cobblestone appearance.

8
Inflammatory Papillary Hyperplasia (Papillomatosis)
Treatment: Discontinue using denture Surgical removal of hyperplastic tissue. Occasionally tissue conditioner may reduce the problem, while reconstruction of new denture may be necessary.

9
Epulis Fissurata (Inflammatory Fibrous Dysplasia, Denture Granuloma)
Etiology: Over-extended denture flanges. Resorption of alveolar bone that makes the denture borders over-extended. Appearance: Hyperplastic granulation tissue surrounds the denture flange. Pain, bleeding, and ulceration can develop.

11
Epulis Fissurata (Inflammatory Fibrous Dysplasia, Denture Granuloma)
Differential Diagnosis: Verrucous carcinoma Squamous cell carcinoma Traumatic fibroma Treatment: Small lesions may resolve if flanges of denture are reduced. Surgical excision is necessary prior to rebasing/relining of denture.

12
Oral Candidiasis

13
Candidiasis Four fungal organisms: Candida albicans, Candida stellatoidea, Candida tropicalis, and Candida pseudotropicalis. Candida albicans is most common. Morphologically, presents in 3 forms: yeast cell, hypha and mycelium (last form is pathogenic phase). Carriers of oral candida do not show the mycelial phase.
. Carriers of oral candida do not show the mycelial phase.")
14
Etiology Mixed infection of Candida albicans, staphylococci and streptococci.

15
Classification of Oral Candidiasis
Acute pseudomembranous candidiasis (moniliasis, thrush). Acute atrophic candidiasis (antibiotic sore tongue). Chronic atrophic candidiasis (denture stomatitis). Chronic hyperplastic candidiasis (candidal leukoplakia, median rhomboid glossitis). Angular cheilitis Chronic mucocutaneous candidiasis.
. Acute atrophic candidiasis (antibiotic sore tongue). Chronic atrophic candidiasis (denture stomatitis). Chronic hyperplastic candidiasis (candidal leukoplakia, median rhomboid glossitis). Angular cheilitis. Chronic mucocutaneous candidiasis.")
16
PAS Stained Candida Albicans Hyphae Embedded in The Oral Mucosa

17
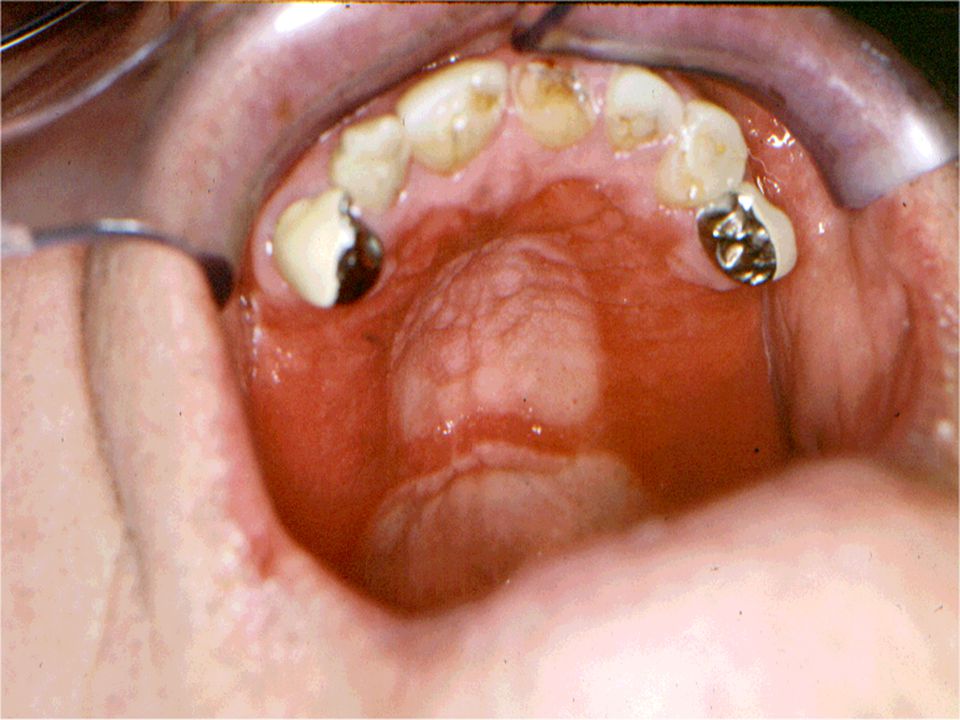
Acute Pseudomembranous Candidiasis (Thrush)
Etiology: Oral candidiasis Appearance: White slightly elevated plaques that can be wiped away leaving an erythmatous base. Direct smear can be fixed and stained using PAS reagent to reveal the candida hyphea microscopically.

19
Acute Atrophic Candidiasis (Antibiotic Sore Tongue)
Etiology: Oral candidiasis secondary to antibiotics or steroids. Appearance: Similar to thrush without overlying pseudomembrane: erythematous and painful mucosa. Differential Diagnosis: Erosive lichen planus. Chemical erosion.

21
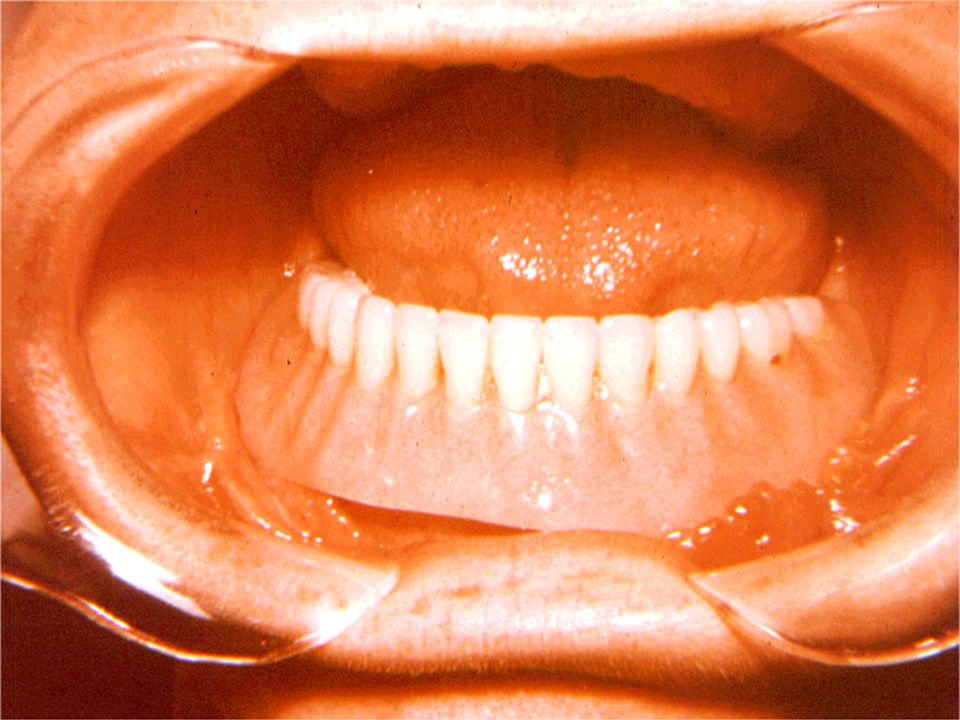
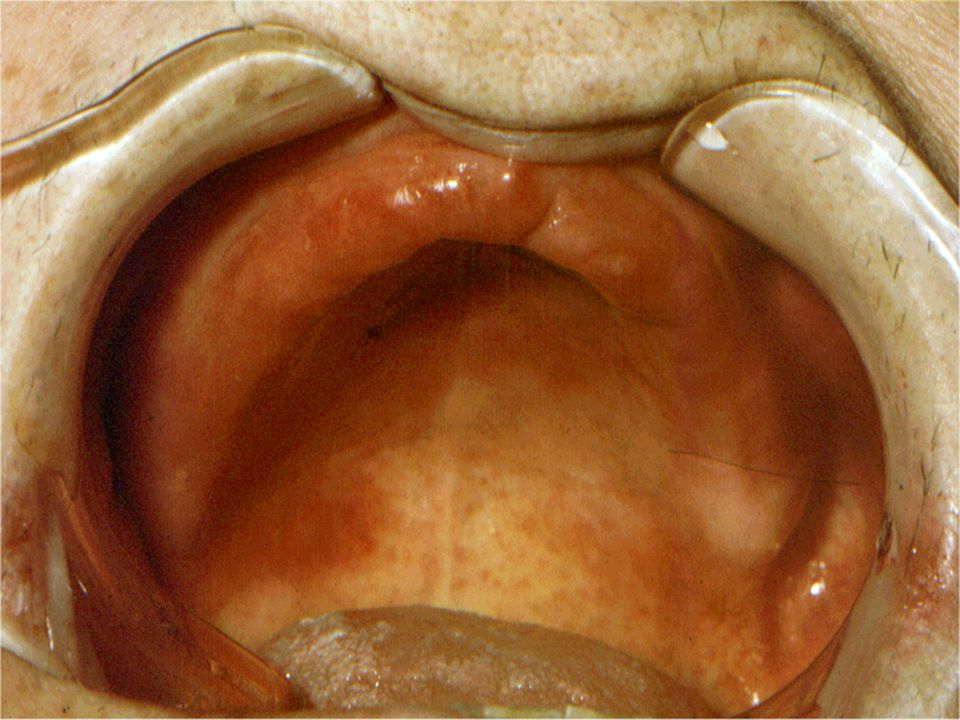
Chronic Atrophic Candidiasis (Denture Sore Mouth)
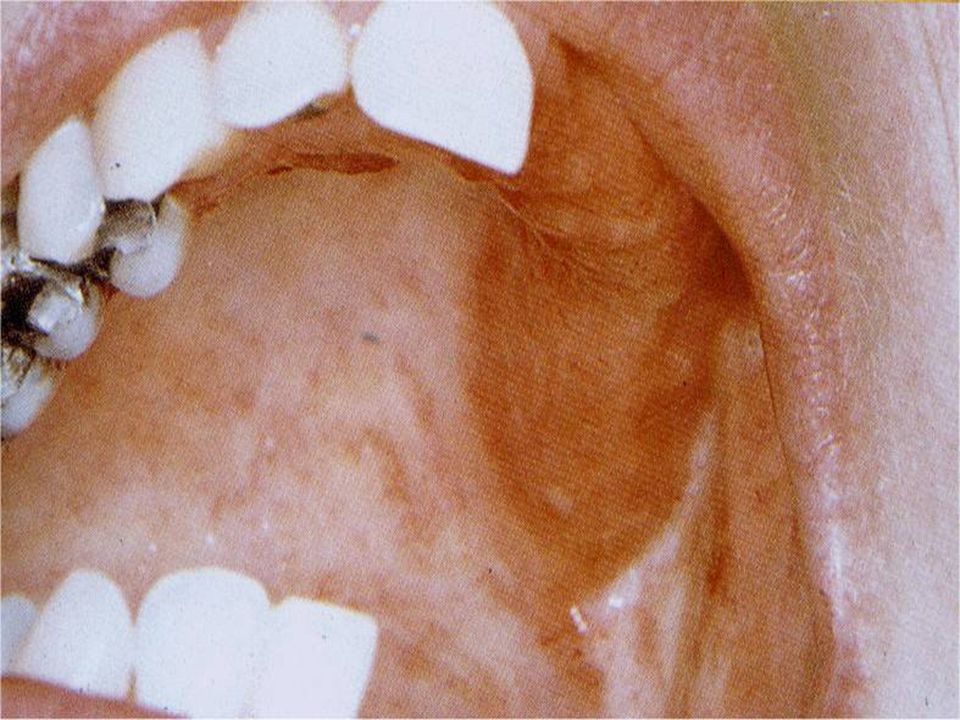
Etiology: Most common form of oral candidiasis; candidal infection of denture as well. Treatment should be directed towards mucosa and denture.

23
Chronic Atrophic Candidiasis (Denture Sore Mouth)
Appearance: Mucosa beneath denture is erythematous with a well-demarcated border. Swabs from the mucosal surface may provide a prolific growth, but biopsy shows few candida hyphae in spite of high serum and saliva antibodies to candida. Differential Diagnosis: Inflammatory papillary hyperplasia.

27
Chronic Hyperplastic Candidiasis (Candida Leukoplakia)
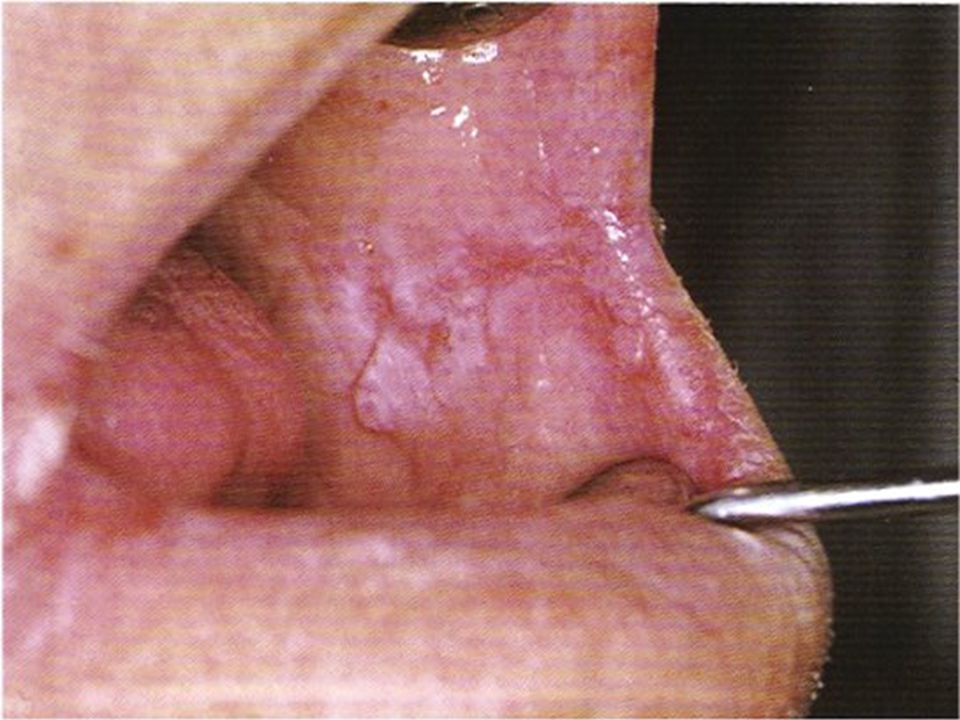
Etiology Oral Candidiasis lesions should be considered as potentially premalignant. Treatment should be directed toward mucosa and Leukoplakia. Appearance Confluent leukoplakic plaques characterized by Candida invasion of oral epithelium with marked atypia.

29
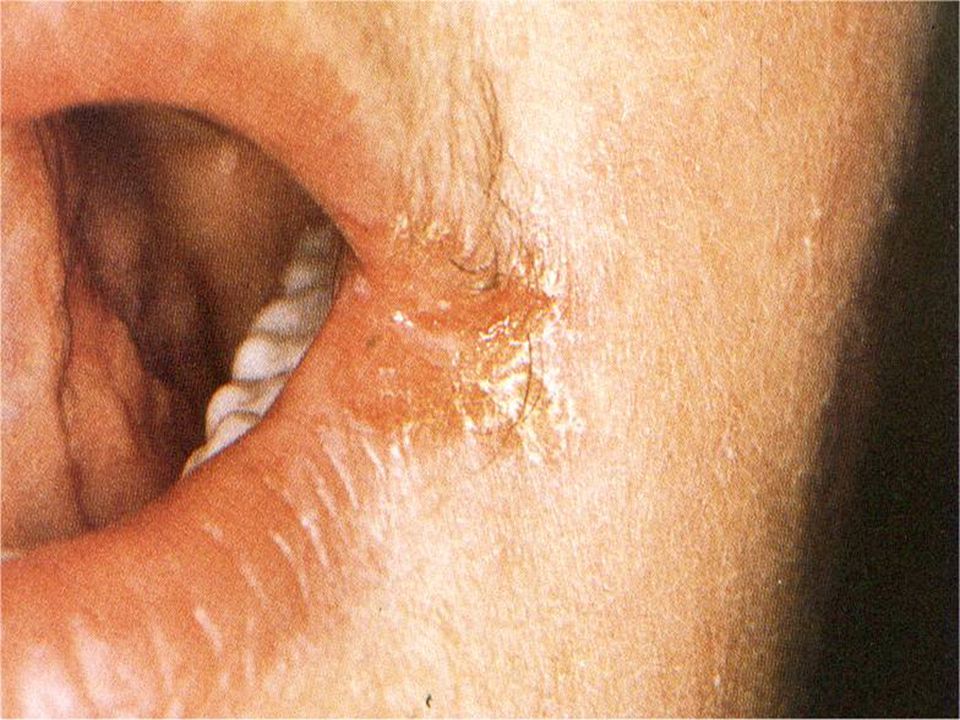
Angular Cheilitis Etiology: Appearance:
Diminished occlusal vertical dimension Vitamin B or iron deficiencies Superimposed candidiasis Affects approximately 6% of General Population Appearance: Wrinkled and sagging skin at the lip commisures. Desiccation and mucosal cracking.

31
Angular Cheilitis Differential Diagnosis: Dry chapped lips.
Basal cell carcinoma. Squamous cell carcinoma.

32
Angular Cheilitis Rx: Nystatin-triamcinolone acetonide ointment.
Disp: 15 gm tube. Sig: Apply to affected area after each meal and qhs. Concomitant intraoral antifungal treatment may be indicated.

33
Chronic Mucocutaneous Candidiasis

34
Diagnostic Criteria C.F.U. in Candidiasis can vary from 1,000/ml to 20,000/ml. As an adjunct to saliva samples, smears stained with PAS. Thus clinical manifestations, salivary culture and stained smears are needed to confirm a diagnosis of Candidiasis.

36
Management of Candidiasis

37
Candidiasis Rx: Nystatin oral suspension 100,000 units/ml.
Disp: 60 ml. Sig: Swish and swallow 5 ml qid for 5 min. Rx: Nystatin ointment. Disp: 15 gm tube. Sig: Apply thin coat to affected areas after each meal and qhs. Rx: Clotrimazole trouches 10 mg. Disp: 70 trouches Sig. Let 1 trouch dissolve in mouth 5 times daily.

38
Candidiasis Rx for Dentures: Improve oral hygiene of appliance.
Keep denture out of mouth for extended periods and while sleeping. Soak for 30 min in solutions containing benzoic acid, 0.12% chlorhexidine, or 1% sodium hypochlorite and thoroughly rinse.

39
Candidiasis Apply a few drops of Nystatin oral suspension or a thin film of Nystatin ointment to inner surface of denture after each meal.

40
Rx for Refractory Candidiasis
Fluconazole 100 mg (20 tabs; 2 tabs stat, then 1 tab daily). Itraconazole 100 mg (20 tabs; 1 tab bid). 2-4 weeks of Ketoconazole 200 mg (20 tabs, 1 tab daily).
. Itraconazole 100 mg (20 tabs; 1 tab bid). 2-4 weeks of Ketoconazole 200 mg (20 tabs, 1 tab daily).")
45
DIAGNOSIS AND MANAGEMENT
OF XEROSTOMIA IN THE ELDERLY PATIENT:

46
Salivary Gland Dysfunction and Xerostomia (Dry Mouth)
")
48
XEROSTOMIA Xerostomia (dry mouth) is defined as a subjective complaint of dry mouth that may result from a decrease in the production of saliva.
 is defined as a subjective complaint of dry mouth that may result from a decrease in the production of saliva.")
49
XEROSTOMIA It affects 17-29% of samples populations based on self-reports or measurements of salivary flow rates. More prevalent in women. Can cause significant morbidity and a reduction in a patient’s perception of quality of life.

50
SALIVA It keeps the teeth healthy by providing a lubricant, calcium and a buffer. It also helps to maintain the health of the gums, oral tissues (mucosa) and throat. It also plays a role in the control of bacteria in the mouth.
 and throat. It also plays a role in the control of bacteria in the mouth.")
51
It helps to cleanse the mouth of food and debris.
It provides minerals such as calcium, fluoride, and phosphorus. It helps in swallowing and digesting food.

52
Lack of saliva will make the mouth more prone to disease and infection.
Lead to a burning feeling.

56
Antimicrobial Factors in Human Whole Saliva
Non-immunoglobulin Factors Origin Lysozyme Salivary glands, crevicular fluid (PMNs) Lactoferrin Salivary glands, crevicular fluid (PMNs) Salivary peroxidase Salivary glands SCN- Salivary glands, crevicular fluid H2O2 Salivary glands, crevicular fluid (PMNs), bacterial and yeast cells Myeloperoxidase Crevicular fluid (PMNs) Cl- Salivary glands, crevicular fluid Agglutinins, aggregating proteins Salivary glands Histidine-rich polypeptides Salivary glands Proline-rich proteins Salivary glands Immunoglobulin Factors Secretory IgA Salivary glands IgA, IgG, IgM Crevicular fluid
 Lactoferrin Salivary glands, crevicular fluid (PMNs) Salivary peroxidase Salivary glands. SCN- Salivary glands, crevicular fluid. H2O2 Salivary glands, crevicular fluid (PMNs), bacterial and yeast cells. Myeloperoxidase Crevicular fluid (PMNs) Cl- Salivary glands, crevicular fluid. Agglutinins, aggregating proteins Salivary glands. Histidine-rich polypeptides Salivary glands. Proline-rich proteins Salivary glands. Immunoglobulin Factors. Secretory IgA Salivary glands. IgA, IgG, IgM Crevicular fluid.")
Similar presentations



















 Pathogenesis` (Mechanisms:inflammation) Clinical Features (Signs and Symptoms) Fever,>")









