Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

4
Visceral, Mucocutaneous and Cutaneous Leishmaniasis
Leishmaniasis is a diseases of different clinical manifestations . Leishmania donovani home the liver and spleen causing (usually fatal) visceral leishmaniasis; 2. Leishmania brasiliensis homes the lining of the nose and throat causing the mucocutaneous disease, 3.Leishmania tropica homes the skin causing the self limiting skin ulcers, called cutaneous leishmaniasis
 visceral leishmaniasis; 2. Leishmania brasiliensis. homes the lining of the nose and throat causing the mucocutaneous disease, 3.Leishmania tropica. homes the skin causing the self limiting skin ulcers, called cutaneous leishmaniasis.")
5
L. tropica L. braziliensis LEISHMANIASIS species of Leishmania :
L. donovani causes visceral leishmaniasis (Kala-azar, black disease, dumdum fever); L. tropica (L.t.major, L.t. minor and L.ethiopica) cause cutaneous leishmaniasis (oriental sore, Delhi ulcer, Aleppo,or Baghdad boil). L. braziliensis ( L. mexicana is a etiologic agents of mucocutaneous leishmaniasis (espundia, Uta, chiclero ulcer).
; L. tropica. (L.t.major, L.t. minor and L.ethiopica) cause. cutaneous leishmaniasis. (oriental sore, Delhi ulcer, Aleppo,or Baghdad. boil). L. braziliensis. ( L. mexicana is a etiologic agents of mucocutaneous leishmaniasis (espundia, Uta, chiclero ulcer).")
6
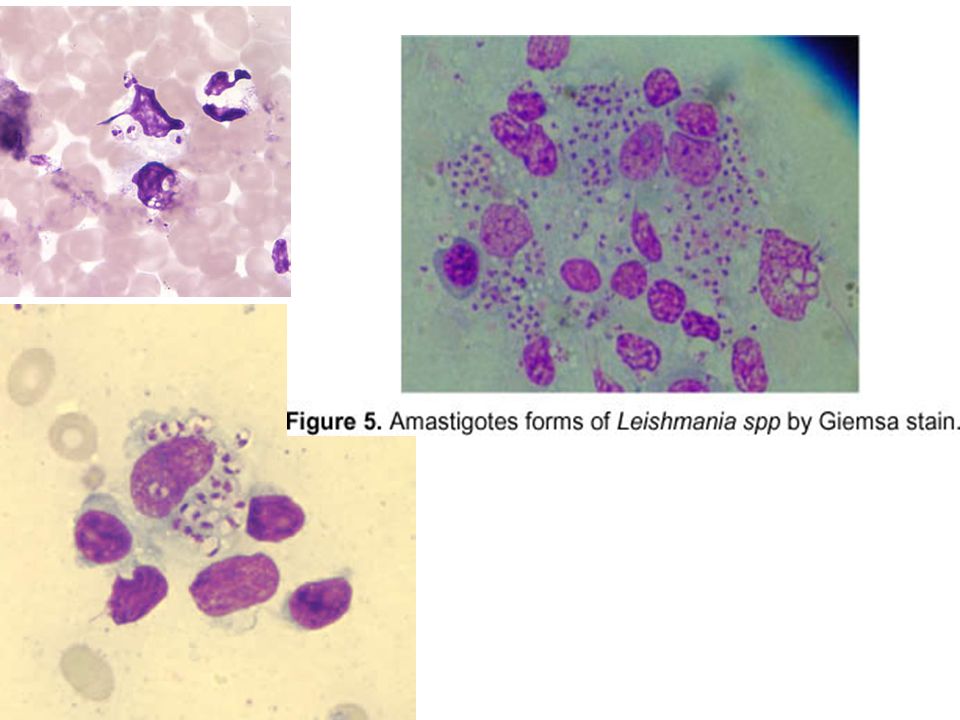
-Amastigote (leishmanial form) is oval and measures 2-5 microns
Morphology -Amastigote (leishmanial form) is oval and measures 2-5 microns -Leptomonad (promastigote form) measures microns a similar size to trypanosomes
 is oval and measures 2-5 microns. -Leptomonad (promastigote form) measures microns. a similar size to trypanosomes.")
7
South east Asia, Indonesia, Pakistan, Mediterranean,
Epidemiology Leishmaniasis is prevalent world wide: South east Asia, Indonesia, Pakistan, Mediterranean, North and central Africa, South and central America.

9
* Endemic in Saudi Arabia
Disease Species Cutaneous leishmaniasis Leishmania tropica* Leishmania major* Leishmania aethiopica Leishmania mexicana Mucocutaneous leishmaniasis Leishmania braziliensis Visceral leishmianiasis Leishmania donovani* Leishmania infantum* Leishmania chagasi * Endemic in Saudi Arabia

10
zoonotic cutaneous leishmaniasis: wet lesion with sever reaction.
Types of cutaneous leishmaniasis * L.major: zoonotic cutaneous leishmaniasis: wet lesion with sever reaction. . * L.tropica: Anthroponotic cutaneous leishminiasis: dry lesions with minimal ulceration. Oriental sore (most common) classical self-limited ulcer.
 classical self-limited ulcer.")
11
Leishmania major –wet lesion

12
Leishmania tropica: dry type

16
Uncommon types * Diffuse cutaneous leishmaniasis (DCL): caused by L. aethiopica, diffuse nodular non-ulcerating lesion. low immunity to leishmania antigens, numerous parasites. * Leishmaniasis recidiva (lupoid leishmaniasis): sever immunological reaction to leishmania antigen leading to persistent dry skin lesions, few parasites.
: sever immunological reaction to leishmania antigen leading to persistent dry skin lesions, few parasites.")
17
1-Diffuse cutaneous leishmaniasis 2-leishmaniasis recidiva (lupoid)
")
20
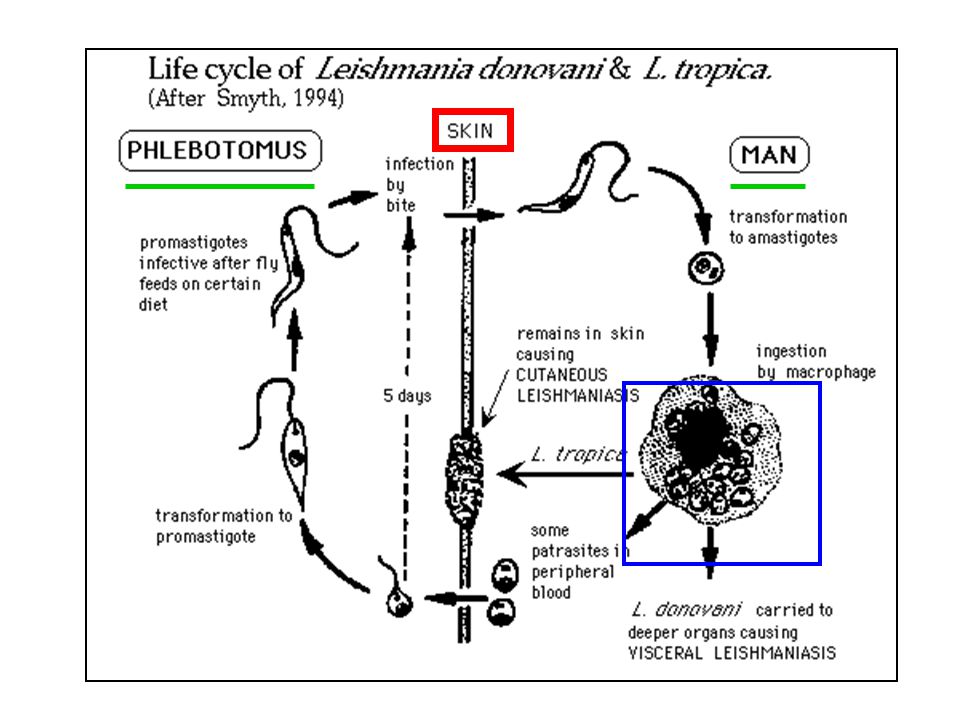
Life cycle The organism is transmitted by blood-feeding sand flies (Phlebotomus) which carry the promastigote . The parasites gain to mononuclear phagocytes where they transform into amastigotes and divide, infected cell ruptures. The released organisms infect other cells. The sand fly take the organisms during the blood meal; the amastigotes transform into flagellate promastigotes and multiply in the gut. Dogs and rodents are common reservoirs.

22
Cutaneous leishmaniasis
Pathology Cutaneous leishmaniasis (Oriental sore, Delhi ulcer, Baghdad boil): the organism (L.tropica) multiplies locally, producing a papule . The papule gradually grows to form a relatively painless ulcer. The ulcer heals in 2-10 months, even if untreated but leaves a disfiguring scar . The disease may disseminate in the case of depressed immune function.
: the organism (L.tropica) multiplies locally, producing a papule . The papule gradually grows to form a relatively painless ulcer. The ulcer heals in 2-10 months, even if untreated but leaves a disfiguring scar . The disease may disseminate in the case of depressed immune function.")
24
Mucocutaneous leishmaniasis
(espundia, Uta, chiclero) It is the same as those of cutaneous leishmaniasis, but the lesions spread to near mucous membrane (oral, pharyngeal and nasal) lead to their destruction and hence sever deformity . The organisms responsible are L. braziliensis, L. mexicana.
 It is the same as those of cutaneous leishmaniasis, but the lesions spread to near mucous membrane (oral, pharyngeal and nasal) lead to their destruction and hence sever deformity . The organisms responsible are L. braziliensis, L. mexicana.")
25
mucocutaneous leishmaniasis

26
Cutaneous and mucocutaneous
Diagnosis: Cutaneous and mucocutaneous 1. aspirate material from edge of ulcer and stain (Giemsa). 2. biopsy - pathology sections. (amastigotes = Leishmania donovani bodies =LD bodies) are seen in macrophages of aspirate and biopsy. 3. culture aspirate or biopsy material in special media (NNN) producing promastigotes.
. 2. biopsy - pathology sections. (amastigotes = Leishmania donovani. bodies =LD bodies) are seen in. macrophages of aspirate and biopsy. 3. culture aspirate or biopsy material in. special media (NNN) producing. promastigotes.")
27
Treatment Medical pentavalent antimony Surgical
No treatment- It self healing lesions. Medical pentavalent antimony (Pentostam), Amphotericin B. +/- Antibiotics for secondary bacterial infection. Surgical - Cryosurgery - Excision - Curettage
, Amphotericin B. +/- Antibiotics for secondary bacterial. infection. Surgical. - Cryosurgery. - Excision. - Curettage.")
29
L. tropica L. braziliensis LEISHMANIASIS species of Leishmania :
L. donovani causes visceral leishmaniasis (Kala-azar, black disease, dumdum fever); L. tropica (L.t.major, L.t. minor and L.ethiopica) cause cutaneous leishmaniasis (oriental sore, Delhi ulcer, Aleppo,or Baghdad boil). L. braziliensis ( L. mexicana is a etiologic agents of mucocutaneous leishmaniasis (espundia, Uta, chiclero ulcer).
; L. tropica. (L.t.major, L.t. minor and L.ethiopica) cause. cutaneous leishmaniasis. (oriental sore, Delhi ulcer, Aleppo,or Baghdad. boil). L. braziliensis. ( L. mexicana is a etiologic agents of mucocutaneous leishmaniasis (espundia, Uta, chiclero ulcer).")
30
Leishmania donovani visceral leishmaniasis L
Leishmania donovani visceral leishmaniasis L.infantum :mainly in infant L.donovani :mainly in adult

33
* Endemic in Saudi Arabia
Disease Species Cutaneous leishmaniasis Leishmania tropica* Leishmania major* Leishmania aethiopica Leishmania mexicana Mucocutaneous leishmaniasis Leishmania braziliensis Visceral leishmianiasis Leishmania donovani* Leishmania infantum* Leishmania chagasi * Endemic in Saudi Arabia

36
L.Donovani -visceral leishmaniasis

37
(kala-azar, dumdum fever)
pathology Visceral leishmaniasis (kala-azar, dumdum fever) Organismes are localized and multiply in the mononuclear phagocytic cells of spleen, liver, lymph nodes, bone marrow, intestinal mucosa and other organs. fever. Hepatosplenomegaly.
 Organismes are localized and multiply in the mononuclear phagocytic cells of spleen, liver, lymph nodes, bone marrow, intestinal mucosa and other organs. fever. Hepatosplenomegaly.")
38
(relative monocytosis and lymphocytosis) -anemia and thrombocytopenia
Bone marrow: -leukopenia (relative monocytosis and lymphocytosis) -anemia and thrombocytopenia hyperpigmented granulomatous skin (kala-azar means black disease). Chronic disease renders patients susceptible to other infections. Untreated disease results in death.
 -anemia and thrombocytopenia. hyperpigmented granulomatous skin. (kala-azar means black disease). Chronic disease renders patients susceptible to other infections. Untreated disease results in death.")
39
Post kala- azar dermal leishmaniasis

40
Presentation Fever . splenomegaly, hepatomegaly, hepatosplenomegaly
Weight loss. Anemia, Epistaxis. Cough, Diarrhea. Untreated case can be fetal. After recovery may be post kala –azar dermal leishmaniasis.

41
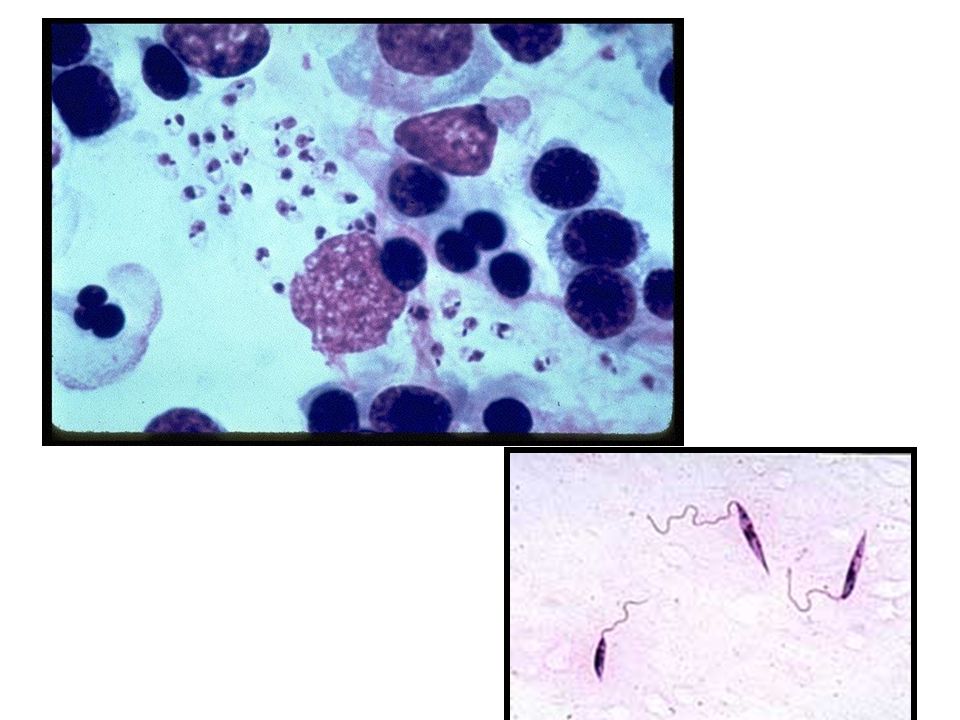
Parasitological diagnosis
*. bone marrow aspirate or spleen puncture and stain (Giemsa) . *.culture material aspirated on (NNN). .Lymph node least sensitive. .tissue biopsy
 . *.culture material aspirated on. (NNN). .Lymph node least sensitive. .tissue biopsy.")
42
1-Bone marrow biopsy 1 2 3-promastigotes 2- rosette shape promastigotes

43
Serological diagnosis:
- direct agglutination test, ELISA, IFAT. - Skin test leishmanin test for survey and follow up after treatment. - non spesfic detection of hyper-gammaglobulinemia by formaldehyde (formol gel test ) or by electrophoresis. - PCR
 or. by electrophoresis. - PCR.")
44
Treatment - Pentavalent antimony
(Pentostam) is the drug of choice. - Amphotericin B. - Treatment of anemia, bleeding, and infection.
 is the drug of choice. - Amphotericin B. - Treatment of anemia, bleeding, and. infection.")
46
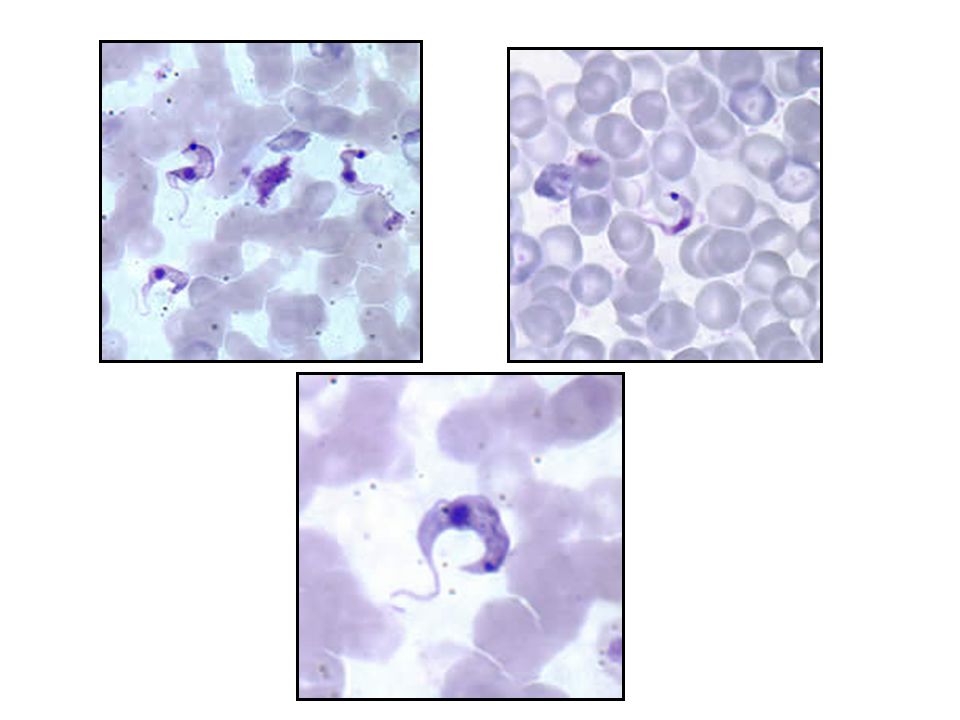
African trypanosomiasis

47
African trypanosomiasis
2 species: -Trypanosoma brucei gambiense (Africa :west of Rift valley) -Trypanosoma brucei rhodesiense (Africa :east of Rift valley)
 -Trypanosoma brucei rhodesiense. (Africa :east of Rift valley)")
49
The reservoir Humans and wild animals (zoonosis) The vector
Glossina (Tsetse) flies
 flies")
50
Glossina

51
African Trypanosomiasis
(African Sleeping Sickness) A hemo-flagylate found only in Africa. In East Africa disease, transmitted from resevoir animal to man by the vector tsetse fly (Glossina) zoonosis. In west Africa it is transmitted by tsetse human to human..
 A hemo-flagylate found only in Africa. In East Africa disease, transmitted from resevoir animal to man by the vector tsetse fly (Glossina) zoonosis. In west Africa it is transmitted by tsetse human to human..")
53
Life cycle The infective metacyclic trypanosome is injected into host during a bite by tsetse fly . it enters the draining lymphatic and blood stream. The trypanosomal form enters the vector during the blood meal and travels through the alimentary canal to the salivary gland where it proliferates as epimastigotes form and matures to infectious metacyclic forms.

55
Pathogenesis Tsetse bites man and injects saliva containing trypanosomes into the wound. These multiply locally producing a local lesion. trypanosome multiplies by binary fission extracellularly producing fever and lymphadenopathy . then reaches the central nervous system producing a meningoencephalitis.

56
Lymphatic &

57
Trypomastigotes can traverse the walls of blood and lymph capillaries into the connective tissues
at a later stage, cross the choroid plexus into the brain and cerebrospinal fluid. The organism can be transmitted through blood transfusion.

58
Clinical picture - trypanosomal chancre - parasitemia with fever
- lymphadenopathy generalized organ involvement. - central nervous system meningoencephalitis, coma and death

59
Bite reaction: T.chancre A non-pustular, painful, itchy chancre appears 1-3 weeks after the bite and lasts 1-2 weeks. It leaves no scar

62
Winterbottom's sign lymphadenopathy Lymphatic involvement imp

63
central nervous system
meningoencephalitis, coma and death

64
Leptomeningitis in brain

65
Trypanosomes found in blood Serological tests (IFAT)
Diagnosis Trypanosomes found in blood lymph and cerebrospinal fluid . Serological tests (IFAT)
")
67
Treatment Suramin Pentamidine (T.gambiense only)
Cases with CNS involvement should be treated with Mel- arsoprol, an organic arsenic compound. -di-fluoro-methly-ornithine (DFMO)
")
68
Major problems - how to control Tsetse fly
-(killing off all wild animal reservoirs?) - vaccine production very difficult because of antigenic variation of trypanosome
 - vaccine production very difficult because of antigenic variation of trypanosome.")
70
Losses due to nagana are estimated at $ 1.5 - 4 billion annually ,
estimated to be new cases of human sleeping sickness with deaths annually (WHO)
")
71
American trypanosomiasis
Chagas' disease

74
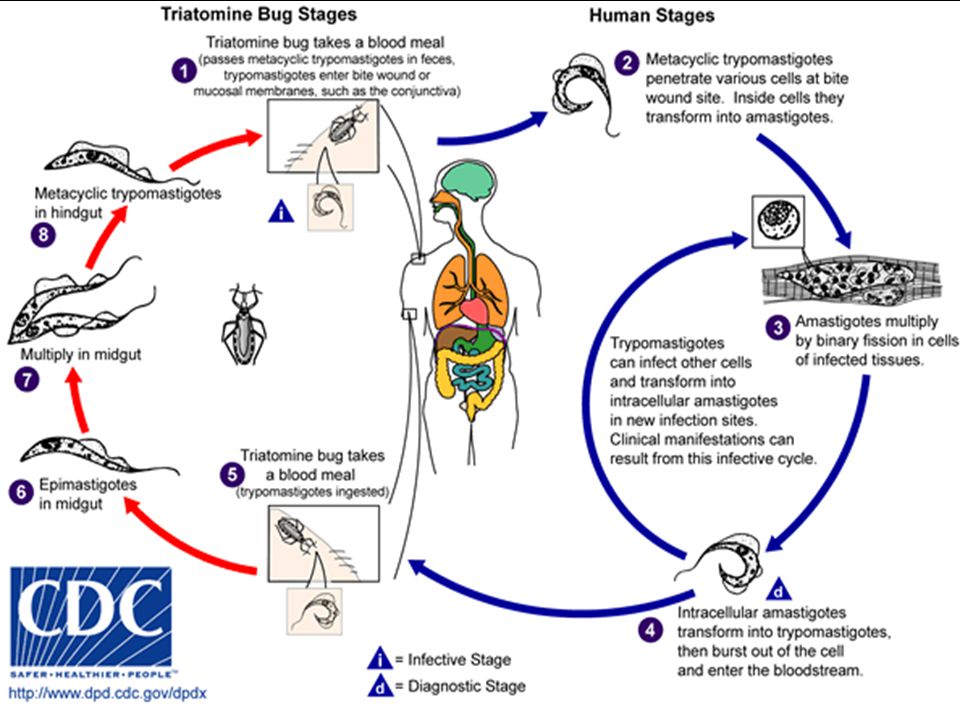
Triatoma winged bug

75
1-The primary lesion, chagoma, appearing at the site of bite
Symptoms Chagas' disease can be divided into three stages: 1-The primary lesion, chagoma, appearing at the site of bite . Infection in the eyelid, resulting in a unilateral conjunctivitis and orbital edema (Ramana's sign)
")
78
2-Acute Stage: Fever, bone and muscle pains. hepatomegaly, and rash.
lymphadenopathy. Diffuse myocarditis, sometimes pericarditis and endocarditis. In children, Chagas' disease may cause meningo-encephalitis and coma. Death occurs in 5-10 percent.

79
3-The chronic: stage results in an abnormal function of the hollow organs, particularly the heart, esophagus and colon. The cardiac changes include myocardial insufficiency, cardiomegaly. Disturbances of peristalsis lead to megaesophagus and megacolon .

84
Treatment Xenodiagnosis imp Diagnosis Trypanosomes found in blood
Serological tests (IFAT or ELISA) Polymerase chain reaction PCR Xenodiagnosis imp Treatment Supportive Benznidazole or nifurtimox
 Polymerase chain reaction PCR. Xenodiagnosis imp. Treatment. Supportive. Benznidazole or nifurtimox.")
86
الحمد لله

87
الحمد لله

Similar presentations





























>")

>")




 Leishmania form Rounded shape, absence of free flagellum,>")


, contain only two genera that parasitize.>")


 (VL) Leishmania tropica (CL) Leishmania major (CL) Leishmania aethiopica (CL) Leishmania mexicana (Complex)>")


