Download presentation
Presentation is loading. Please wait.

1
History & examination of patients with abdomen, pelvis or perineum problems
Prof. M K Alam

2
HISTORY CLINICAL EXAMINATION CLINICAL DIAGNOSIS INVESTIGATIONS FINAL DIAGNOSIS TREATMENT

3
IMPORTANT POINTS BEFORE HISTORY-TAKING
Introduce yourself Explain yourself Full attention Treat with respect Let patient talk Guide, not dictate No leading question No short-cuts Try not to write and talk at the same time

4
Different parts of a history
PERSONAL DETAILS PRESENTING COMPLAINT HISTORY OF PRESENT ILLNESS SYSTEMIC INQUIRY PAST MEDICAL/SURGICAL HISTORY FAMILY HISTORY HISTORY OF MEDICATIONS SOCIAL HISTORY OTHER HISTORY

5
PERSONAL DETAILS NAME AGE SEX NATIONALITY MARITAL STATUS OCCUPATION
Record date of history taking and examination

6
PRESENTING COMPLAINT What are you complaining of?
(record in patient’s own words) When more than one complain: (record in order of severity)
 When more than one complain: (record in order of severity)")
7
HISTORY OF PRESENT ILLNESS
Full analysis of the complain or complaints. Get right back to the beginning of the trouble

8
COMMON COMPLAINTS Abdominal pain Abdominal mass or swelling
Change in bowel habit Vomiting Abdominal distension Discharge (abdomen, perineum)
")
9
Analysis of pain Site: ask patient to point- finger vs hand
Onset : Slow- inflammation Sudden- perforation, ischemia Severity: Mild in beginning- inflammation Severe- perforation, ischemia

10
Site: Pain locations (Great degree of overlap)
Right hypochondrium.- gallbladder Left hypochondrium.- pancreas Epigastrium.- Stomach and duodenum Lumber- kidney Umbilical- small bowel, caecum, retroperitoneal Right iliac fossa- Appendix, caecum Left iliac fossa- Sigmoid colon Hypogastrium- Colon, urinary bladder, adenexae

11
Analysis of pain Nature: dull (inflammation), sharp (rupture viscus), colic (intermittent) throbbing (abscess) Progression: steady increase (inflammation), decreasing, fluctuating (colic) Duration: acute or chronic
, decreasing, fluctuating (colic) Duration: acute or chronic.")
12
Analysis of pain Aggravating factors: fatty foods increases pain in gallstone disease Relieving factors: Sitting and leaning forward eases pain in acute pancreatitis. Eating relieves pain in duodenal ulcer

13
Analysis of pain Radiation or referred pain: Shoulder- cholecystitis, Groin- ureteric colic Shifting or migration: periumbilical to RIF in acute appendicitis Cause: Trauma, Food from outside- gastroenteritis Medication (NSAID)- perforation, bleeding
- perforation, bleeding.")
14
Swelling or mass When noticed? Acute (hematoma, abscess) chronic- neoplasm, organomegaly How noticed? Incidentally noticed swelling may be present for a longer duration Painful or painless? Inflammatory, neoplasm Change in size since first noticed? Increase- neoplasms, disappear or reduce in size? -hernias Aggravating/relieving factors: Hernias increase in size with activity Any cause? Trauma- hematoma, cough- hernia

15
Bowel habit Constipation: habitual, recent (neoplasm)
Absolute constipation (obstipation): Intestinal obstruction Diarrhoea: duration (acute, chronic), number of stool, any blood or mucous (IBD), Color of stool: Bright red (anal, rectum), maroon (colon) black- melena (upper GI)
: Intestinal obstruction. Diarrhoea: duration (acute, chronic), number of stool, any blood or mucous (IBD), Color of stool: Bright red (anal, rectum), maroon (colon) black- melena (upper GI)")
16
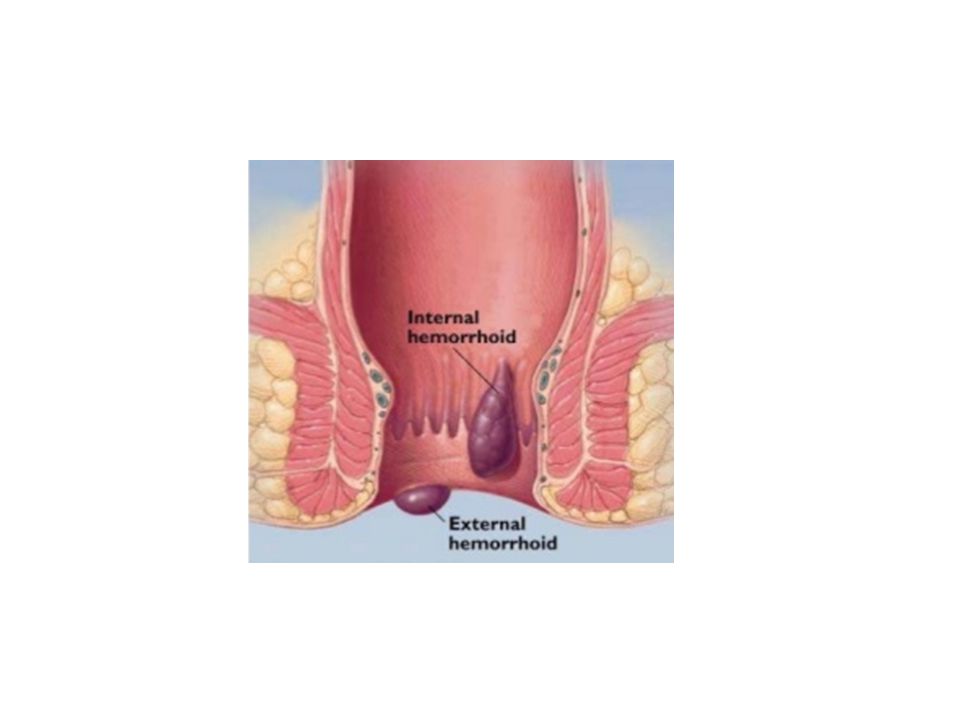
History of discharge Site: anal, perineum, wound Duration
Nature: purulent (anal fistula), bloody (hemorrhoid), fecal from wound ( int. fistula) Relationship to defecation/stool- mixed with stool- IBD, independent of stool- hemorrhoid Any pain? Hemorrhoids- painless, anal fistula- painful
, bloody (hemorrhoid), fecal from wound ( int. fistula) Relationship to defecation/stool- mixed with stool- IBD, independent of stool- hemorrhoid. Any pain Hemorrhoids- painless, anal fistula- painful.")
17
Vomiting Non- bilious: Early stage, late- pyloric obstruction
Bilious: bowel obstruction Faeculent: late stage of bowel obstruction Blood: Duodenal ulcer, oesophageal varices, neoplasm Vomiting relieves pain- gastric ulcer Vomiting food taken few days ago: pyloric stenosis

18
SYSTEMIC INQUIRY Begin with the involved or affected (chief complain) system Example: If chief complaint is related to gastrointestinal system(GI)- continue with the GIT inquiry.
- continue with the GIT inquiry.")
19
SYSTEMIC INQUIRY- GIT Weight- amount, duration Appetite Dysphagia
Nausea Vomiting Heartburn Haematemesis Flatulence Jaundice Abdominal pain Fat intolerance Constipation Diarrhoea Melena Rectal bleeding Stool

20
SYSTEMIC INQUIRY Respiratory system: Cardiovascular system:
Cough, sputum, hemoptysis, wheeze, dyspnea, chest pain Cardiovascular system: Angina (cardiac pain), dyspnea ( rest/ exercise), Palpitations, ankle swelling, claudication
, dyspnea ( rest/ exercise), Palpitations, ankle swelling, claudication.")
21
SYSTEMIC INQUIRY Obstetric & Gynecology LMP Vaginal discharge
Vaginal bleeding Pregnancies Nervous system Headache Fits Depression Facial/limb weakness

22
SYSTEMIC INQUIRY MUSCULOSKELETAL
Muscular pain Bone & Joint pain Swelling of joints Limitation of movements Weakness

23
SYSTEMIC INQUIRY METABOLIC/ENDOCRINE
Bruising/ bleeding (nutrients deficiencies) Sweating (thyrotoxicosis) Thirst (diabetes) Pruritus (skin infection, jaundice, uremia, Hodgkin’s) Alcohol Weight- ?dieting, amount and duration
 Sweating (thyrotoxicosis) Thirst (diabetes) Pruritus (skin infection, jaundice, uremia, Hodgkin’s) Alcohol. Weight- dieting, amount and duration.")
24
PAST MEDICAL/ SURGICAL HISTORY
Rheumatic Fever Tuberculosis/ asthma Diabetes Jaundice Operations/ accident Blood transfusion Mental illness

25
FAMILY HISTORY Diabetes Hypertension Heart disease Malignancy
Cause of death Father/Mother/Siblings/Spouse/Children/Grand parents / Close relatives

26
HISTORY OF MEDICATIONS
Insulin Steroids NSAID Contraceptive pills Antibiotics Others

27
SOCIAL HISTORY Marital status Occupation Travel abroad Accommodation
Habits ( smoking, alcohol ) Dependent relatives
 Dependent relatives.")
28
OTHER HISTORY Psychiatric/ emotional background Allergies
Food Drugs Immunizations Tetanus Diphtheria Tuberculosis Hepatitis Others

29
Review and analyse More questions looking for clues?

30
Clinical Examination Before starting a clinical examination, analyze patient’s history for a possible diagnosis

31
CLINICAL EXAMINATION Observe your patient while history taking:
General health- emaciated (? Malignancy) Intelligence Attitude Mental state (dehydration, encephalopathy) Posture ( peritonitis- flexed & still) Mobility
 Intelligence. Attitude. Mental state (dehydration, encephalopathy) Posture ( peritonitis- flexed & still) Mobility.")
32
CLINICAL EXAMINATION Permission Privacy Presence of a nurse
Precautions

33
CLINICAL EXAMINATION Inspection Palpation Percussion Auscultation

34
CLINICAL EXAMINATION Practice a standard routine every time
Hand- head to toe Head to toe

35
General Examination Weight- loss (malignancy), gain (DU)
Pulse (Tachycardia- infection, fluid/ blood loss Blood pressure (low- fluid loss, bleeding) Temperature ( Fever- infection) Respiration rate- raised in infections
 Temperature ( Fever- infection) Respiration rate- raised in infections.")
36
General Examination Pulse- rate, rhythm, volume, nature
Nails- koilonychia, clubbing Skin- dehydration, moist palm, anemia Anemia- conjunctiva, nail bed Jaundice- sclera, under surface of tongue Oral cavity- mucous membrane for hydration status, tongue for coating Scalp Ear/ nose

37
General Examination Neck- vein, goitre, lymph nodes, other swellings
Chest- asymmetry, expansion, breath sound, added sound Cardiac- rhythm, heart sound, murmur Abdomen (local examination) Limbs- asymmetry, swelling, movement, pulses, power
 Limbs- asymmetry, swelling, movement, pulses, power.")
38
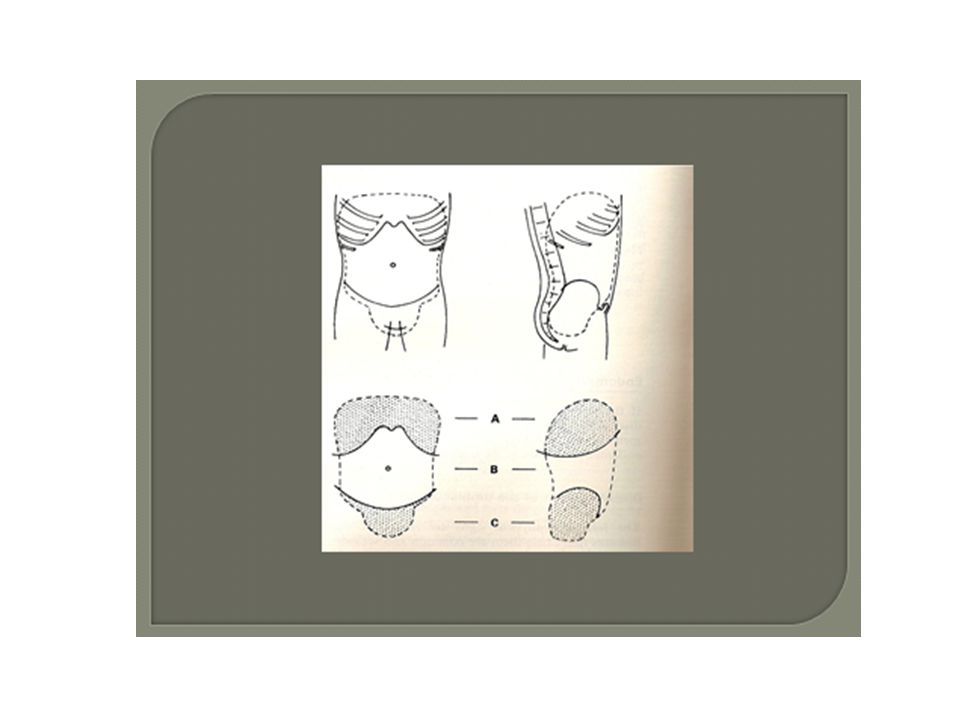
LOCAL EXAMINATION (ABDOMEN)
Abdomen-extends from nipple level to the bottom of the pelvis Exposure: nipples to knees (ideal) Patient lying flat on a pillow Arms by the side ( not under the head!) Sit or kneel beside the patient Adequate light
 Patient lying flat on a pillow. Arms by the side ( not under the head!) Sit or kneel beside the patient. Adequate light.")
42
INSPECTION OF THE ABDOMEN
Asymmetry (from the foot end of the bed)- mass Movement with breathing (restricted- peritonitis) Swelling or mass- location Distension- central (SIO) or peripheral (LBO, ascites) Scar, sinus, wound Prominent veins (portal hypertension) Shape of the umbilicus Cough impulse ( groin, umbilicus, scar)
- mass. Movement with breathing (restricted- peritonitis) Swelling or mass- location. Distension- central (SIO) or peripheral (LBO, ascites) Scar, sinus, wound. Prominent veins (portal hypertension) Shape of the umbilicus. Cough impulse ( groin, umbilicus, scar)")
45
PUH

46
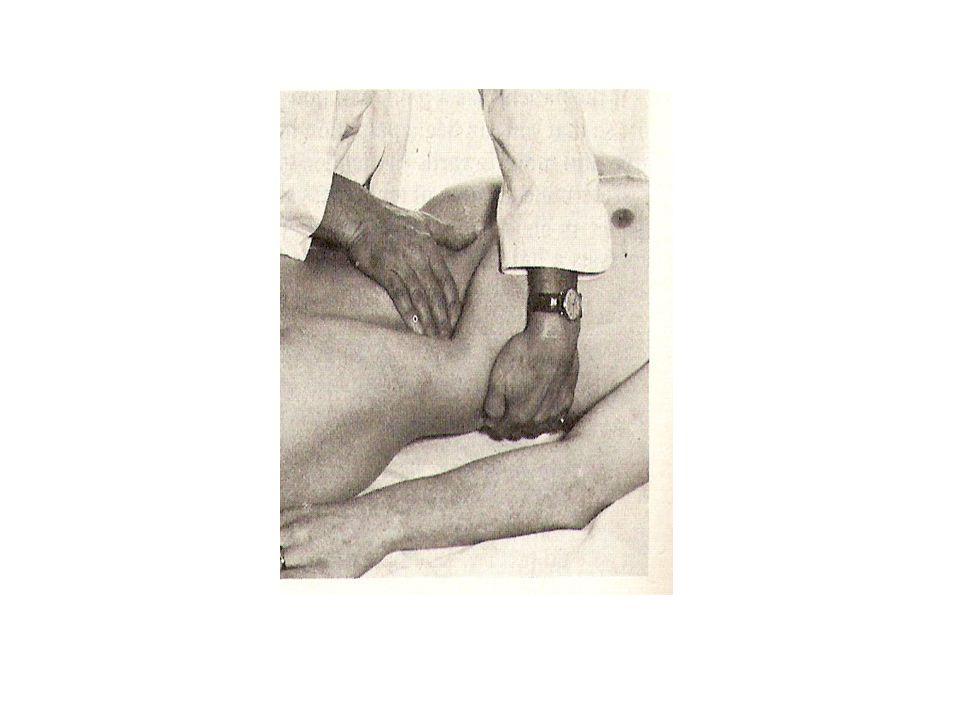
PALPATION OF THE ABDOMEN
Gentle palpation: start away from the area of pain- for tenderness Deep palpation- deep tenderness- acute pancreatitis, Murphy’s sign, Rovsing’s sign Guarding: muscle contracted overlying the tender area- acute inflammations

47
Palpation Organomegaly: liver , spleen, kidneys
Other masses- abdominal wall or intra-abdominal Define all the features of a mass (site, size, surface, borders, tenderness, pulsation, mobility) Cough impulse
 Cough impulse.")
50
Palpable masses Mass in RUQ: ca. hepatic flexure, enlarged gallbladder, enlarged right kidney, hepatomegaly Mass in epigastric region: liver, gastric carcinoma, abdominal aortic aneursym Mass in LUQ: splenomegaly, carcinoma descending colon, swelling in tail of pancreas, enlarged left kidney Mass in periumbilical region: PUH, ca. transverse colon, tumour deposit (Sister Mary Joseph's nodule)
")
51
Palpable masses Mass in LLQ: faecal scybala, carcinoma descending colon Mass in the suprapubic region: distended urinary bladder, pregnancy, ovarian mass Mass in RLQ: appendiceal disease, ca. ascending colon, Crohn's disease of ileo-caecal area Mass in inguinal region: hernia, lymphadenopathy, aneurysm

52
Percussion Organs and masses Liver span Ascites: fluid thrill, & shifting dullness Auscultation Bowel sounds: normal, increased (bowel obst.) absent (peritonitis, ileus) Bruit- vascular lesions Succussion splash (pyloric stenosis)
 absent (peritonitis, ileus) Bruit- vascular lesions. Succussion splash (pyloric stenosis)")
53
Abdominal wall hernias
Swelling Vary in size: Disappear or reduce with rest. Increase in size with activity- standing, coughing Pain- mild to severe Irreducibility

54
Examination of abdominal wall hernias
Inspection: (?standing vs lying) Site ( groin, scars) Extension to scrotum, Scar, Cough impulse Reducibility
 Site ( groin, scars) Extension to scrotum, Scar, Cough impulse. Reducibility.")
58
Percussion- resonant if content is bowel Auscultation- bowel sound
Palpation: ?Can get above it-inguinoscrotal swellings Tenderness Cough impulse Reducibility Defect Control by blocking internal ring Percussion- resonant if content is bowel Auscultation- bowel sound

60
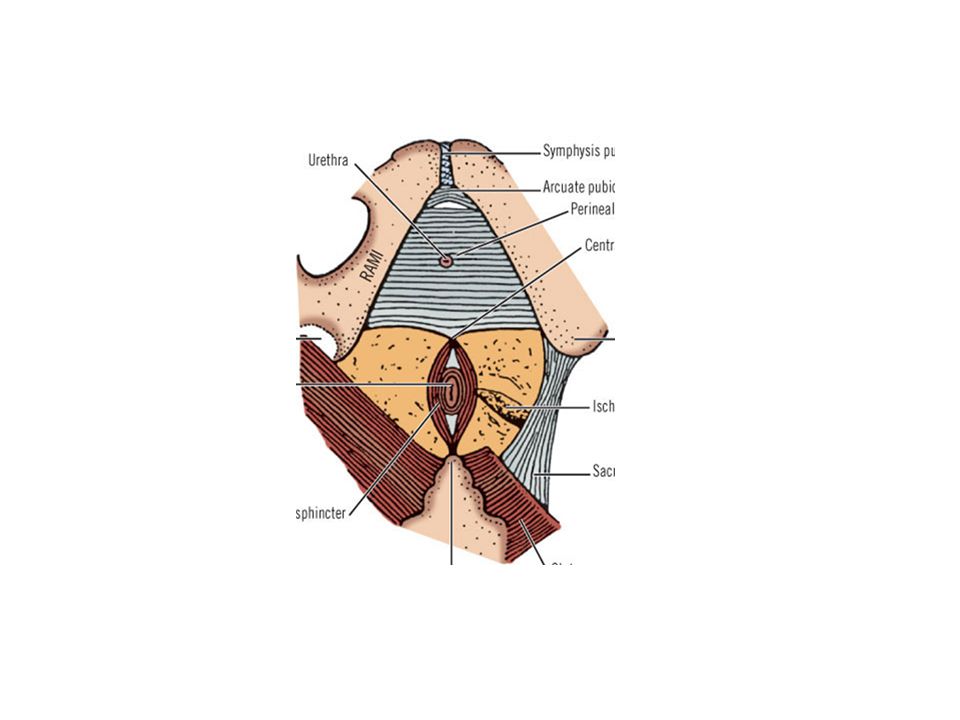
EXAMINATION OF THE PERINEUM
External genitalia Perineum examination: left lateral position, hips flexed to 90º and knees flexed to less than 90° Lift uppermost buttock to expose the area

62
Inspection: scar of previous surgery, sinus (one opening blind track), fistula (track connecting two epithelial surfaces) fecal soiling, blood/mucous discharge, mass protruding from anus Palpation: tenderness, discharge, mass Rectal examination: Tone, tenderness, mass, prostate, blood, stool

65
Thank you!

Similar presentations











>")



 The McGraw-Hill Companies, Inc. Permission required for reproduction or display. 23-1 Chapter 23 Abdominal and Gastrointestinal Disorders.>")












>")
