Download presentation
Presentation is loading. Please wait.

1
DA 2 Update for CI 1 November 2013

2
Outline Situation Analysis Priorities for 2013 New Technologies Results 2

3
Situation Analysis Current State:Future State:Impact: Reporting Performance MetricsAnalyzing Performance MetricsEfficiency, Quality, Costs Minimal Predictive AnalyticsFocus on Predictive Analytics Quality, Costs, Population Health Manual Data AbstractionAutomated Data AbstractionEfficiency, Costs Multiple Data Silos Enterprise Data Warehouse (EDW) Efficiency, Quality No Data GovernanceRobust Data GovernanceSafety, Efficiency, Quality Minimal Self-Service CapacityUser Driven Data AccessEfficiency, Quality, Costs Limited Awareness of AnalyticsData is a System AssetData Quality Poor Data Quality High Quality Data/One Source of Truth Data Quality, Efficiency Unmet Analytic NeedsHigh Client SatisfactionEfficiency, Quality, Costs 3
 Efficiency, Quality No Data GovernanceRobust Data GovernanceSafety, Efficiency, Quality Minimal Self-Service CapacityUser Driven Data AccessEfficiency, Quality, Costs Limited Awareness of AnalyticsData is a System AssetData Quality Poor Data Quality High Quality Data/One Source of Truth Data Quality, Efficiency Unmet Analytic NeedsHigh Client SatisfactionEfficiency, Quality, Costs 3")
4
DA 2 Priorities for 2013 1.Performance Metrics: Develop reliable and actionable leading indicators for clinical and non-clinical operational performance metrics 2.Quality and Value: Demonstrate CHS clinical quality, value and improved patient outcomes to payers and employers 3.Population Health: Provide predictive analytics using full range of data available to positively impact patient health by proactive delivery of preventative services. 4

5
Technology to Support Priorities SoftwareDescription VeriskAllows capability to conduct population analysis, employer group analysis, practice pattern variation, episode analysis on claims data HumedicaAllows capability to conduct population analysis and provide medical home reporting using clinical (EMR) data. Can compare, analyze and identify clinical best practices near real time. PredixionRemoves reliance on technical analysts to accelerate predictive analytics capability. Point of care predictive analytics through workflow. 5 Accelerators for Rapid Value Creation:

6
Data CoE Data Services IT Infrastructure Services Shared Resource pool Information Architecture Requests SLA Requests Data Marts, Extracts, Automation, SLA Requests Estimates Models Reports Analytics Requests Abstraction Services Shared Resource pool Requests SLA Requests Services, SLA Opportunity Analysis Demand Management Services, SLA Color Key: Blue = Business Maroon = DA² Green = IT Pink = External Color Key: Blue = Business Maroon = DA² Green = IT Pink = External Client Services Requests Data, SLA Shared Resource Pool Think Tank Leading metric development Key capabilities Analytic Services Analytics CoE Abstraction CoE Research Building an Analytic Competency Service Lines and Functional Units 6

7
DA² New Organization Structure Michael Dulin CCO Melanie Spencer Research Director Allen Naidoo VP Client Services Mike Trumbore AVP Analytic Services John Carew AVP Financial Services Director Marcy Neale Director - Quality Avery Ashby Director Abstraction Svcs Angela Humphrey AVP Data Services Tim Reagan AVP Rodney White Director IT EDW Team 7

8
Organization Impact INNOVATIVE LEADER DA² will apply innovative techniques and tools to the analysis of health information and will challenge the status quo uses of information and move the CHS culture forward to raise the collective CHS analytics IQ. ADVANCED ANALYTICS AND BUSINESS INTELLIGENCE DA² will apply a balanced approach to understanding business needs, promoting data governance and integrity, analyzing routine and complex data, and providing relevant and targeted intelligence to solve business problems. ELEVATE PATIENT OUTCOMES Quality of care is the cornerstone of the CHS business model and DA² is fully aligned to support existing and new initiatives to improve quality. PREDICT HEALTH NEEDS The true advancements will come from the modeling of data to predict the relationship of individuals with disease processes so proactive interventions can be employed. TRANSFORMATIVE SOLUTIONS DA² will focus on projects apt to move CHS in a material and enduring direction toward a successful future state. PROMOTE THE HEALTH OF OUR COMMUNITIES Population health management is an advanced state comprising all of the activities of CHS and DA² to improve the well‐being of the citizens in our services areas. 8

9
Results DA2 Acute Care Predictive Analytics (Readmissions) DA2 Ambulatory Analytics Population Health – Population Segmentation and Stratification 9
 DA2 Ambulatory Analytics Population Health – Population Segmentation and Stratification 9")
10
DA 2 Predictive Analytics Impacting Readmissions

11
SegmentsLow Risk Medium RiskHigh Risk Very High Risk Total Volume 9 x 9, Emergency and Medicare 3.90%1.13%3.42%2.41%10.86% Lengthy Stays, Large Number of Orders 2.84%2.10%3.80%5.77%14.51% New Patients, Longer Visits 3.44%2.18%7.32%1.44%14.37% New Patients, Shorter Visits 7.94%11.98%3.79%0.15%23.85% Older Frequent Flyers 0.29%0.72%0.79%8.57%10.37% Simpler than 9 x 9, Medicine, Discharged Home 1.02%0.20%0.50%1.98%3.70% Younger and Healthy 2.71%4.70%2.37%0.54%10.32% Younger Frequent Flyers 2.88%1.98%3.02%4.15%12.02% Total Volume25.00% 100.00% Readmission Risk Modeling and Patient Segmentation 200,000 Hospitalizations 600 Predictor Variables Readmission Risk Model 40 Key Predictors Patient Segmentation

12
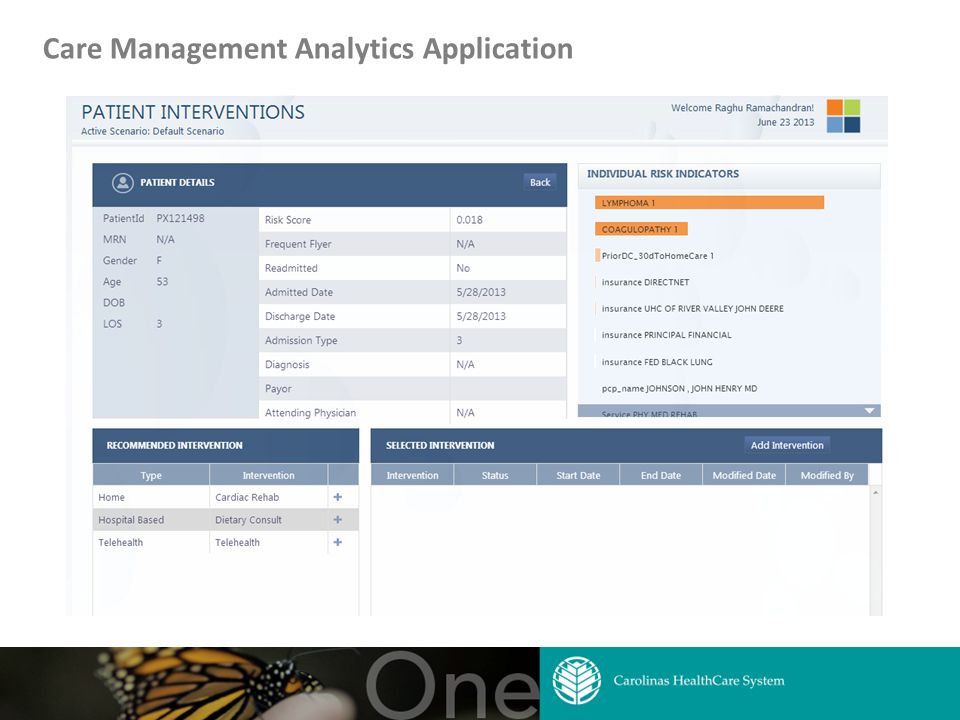
Care Management Analytics Application

14
DA 2 Ambulatory Analytics Using Analytics to Improve Outcomes for Patients with Diabetes

15
15 Capabilities

16
16 Capabilities Outline Identify patients who are out of compliance for recommended tests or visits Identify patients with heavy disease burden who are no being actively managed Gaps in Care Identify and stratify patients at high risk of hospitalization or disease complication Predictive Modeling Track patients and providers with high utilization scores (ER or IP Visits within time period) Monitor readmissions and post-discharge follow-up Cost & Utilization Management Profile poly-chronic patients Discover actionable clinical insights by patient cohort High Risk Patient Management Identify costly drug prescribing patterns in relation to clinical outcomes Track compliance against medical protocols Prescribing Patterns
 Monitor readmissions and post-discharge follow-up Cost & Utilization Management Profile poly-chronic patients Discover actionable clinical insights by patient cohort High Risk Patient Management Identify costly drug prescribing patterns in relation to clinical outcomes Track compliance against medical protocols Prescribing Patterns")
17
17 Benchmarking Opportunities Anonymous Built into Humedica MinedShare ® Ambulatory tool CHSMG Ambulatory data compared to blinded comparator group Comparator group includes all of Humedica’ s ambulatory clients, but can be filtered based on criteria such as region and size Anonymous Transparent CHSMG is included in American Medical Group Association (AMGA) and the Anceta Collaborative through Humedica Anceta uses data to identify opportunities for improvement and best performance Collaborative members share and learn from each other Transparent
 and the Anceta Collaborative through Humedica Anceta uses data to identify opportunities for improvement and best performance Collaborative members share and learn from each other Transparent")
18
Sample Output 18

19
Sample Output 19

20
DA 2 Population Health Efforts

21
Storyline Current Status Foundational Efforts Underway Potential Care Management Activities 21

22
Vital Statistics 1,524,282 Unique Patients* accessed CHS IP/OP Hospital Services and/or Medical Group Practice Services during August 2012 – July 2013 22 Medical Group Practice Services Charges $2.641B IP/OP Hospital Services Charges $10.171B * Unique patients are determined using IBM® Initiate Master Data Service® products looking across IDX, STAR, and Cerner

23
Patient & Charged Amount Distribution 23 1% Patients (15,243) $3,674,713,631 or 28.7% Total Charged Amount Mean = $242,299 4% Patients (60,971) $4,013,166,277 or 31.3% Total Charged Amount Mean = $65,820 25% Patients (381,071) $4,123,756,151 32.2% Total Charged Amount Mean = $10,821 70% Patients (1,066,997) $999,518,908 7.8% Total Charged Amount Mean = $985*
 $3,674,713,631 or 28.7% Total Charged Amount Mean = $242,299 4% Patients (60,971) $4,013,166,277 or 31.3% Total Charged Amount Mean = $65,820 25% Patients (381,071) $4,123,756, % Total Charged Amount Mean = $10,821 70% Patients (1,066,997) $999,518, % Total Charged Amount Mean = $985*")
24
70% Patients (858,461) $847,618,912 7.8% Total Charged Amount (Mean = $1,038** ) Core Market* Vital Statistics 24 1,226,372 Core Market Unique Patients accessed IP/OP Hospital Services and/or Medical Group Practice Services during August 2012 – July 2013 ** Core Market defined by patient’s zip code (Management Company); CHS standard for all planning & reporting purposes ** Does not include patients with zero total charges in the calculation 80% of Unique Patients 84% of Charged Amount 1% Patients (12,264) $3,011,776,739 or 27.9% Total Charged Amount Mean = $245,599 4% Patients (49,054) $3,348,738,254 or 31.1% Total Charged Amount Mean = $68,265 25% Patients (306,593) $3,576,082,446 33.2% Total Charged Amount Mean = $11,664
 $847,618, % Total Charged Amount (Mean = $1,038** ) Core Market* Vital Statistics 24 1,226,372 Core Market Unique Patients accessed IP/OP Hospital Services and/or Medical Group Practice Services during August 2012 – July 2013 ** Core Market defined by patient’s zip code (Management Company); CHS standard for all planning & reporting purposes ** Does not include patients with zero total charges in the calculation 80% of Unique Patients 84% of Charged Amount 1% Patients (12,264) $3,011,776,739 or 27.9% Total Charged Amount Mean = $245,599 4% Patients (49,054) $3,348,738,254 or 31.1% Total Charged Amount Mean = $68,265 25% Patients (306,593) $3,576,082, % Total Charged Amount Mean = $11,664")
25
8 County View – Unique Patient Counts* 25 Anson Cabarrus Cleveland Gaston Lincoln Mecklenburg Stanly Union 10,531 142,825 68,272 74,285 41,208 530,244 23,625 120,567 * Unique patients utilizing CHS IP/OP Hospital Services and/or Medical Group Practice Services during Aug 2012 – Jul 2013

26
26 Aug 2012 – July 2013

27
27 Aug 2012 – July 2013

28
FOUNDATIONAL FRAMEWORK PCP Attribution Indigent Identification & Modeling DA 2 Patient 360º Information 28

29
PCP Attribution Time Period CPT Codes Provider Level SpecialtyVolume Visit Recency DIVISION PROVIDER 29 Note: Attribution is first determined in the most recent 12 months, and then if needed, looks within the previous 12 months. Future state may include variation in the time frame used, based on patient demographics/conditions.

30
Indigent Identification & Modeling Common system-wide definition Tagging of patients known to be indigent Predicting patients of becoming charity or over due using social determinants/financial and other information Micro-segmenting for outreach opportunities to enable primary care and community resource utilization 30

31
DA 2 Patient 360º Information 31

32
POTENTIAL INITIATIVES FOR IMPACT DA 2 Ambulatory Analytics Use Cases DA 2 Predictive Analytics Use Cases DA 2 Segmentation 32

33
DA 2 Ambulatory Analytics Use Cases – Diabetes Focused Diabetic Outreach based on Lab Data 33 http://www.diabetes24-7.com

34
DA 2 Predictive Analytics Use Cases – Top 5% Readmission Risk at CMC 34 Statistically significant differences between the top 5% and the remaining 95% for: Insurance Type Race Age Admission Type * Gender was not statistically different Patient segments will be identified, mapped across the CHS service area, and proper outreach developed

35
Patient Mapping 35 There were 183 patients with 100 in Mecklenburg County

36
DA 2 Research

37
Asthma CER 37

40
AHRQ Asthma 40

41
Asthma Comparative Effectiveness (ACE) Research Database Outcome measures for 12,581 eligible asthma patients Service Utilization Medication Compliance Appropriate Care Quality of Life (QoL) ACER Billing Data Medicaid Claims Spatial Data School Data Clinical Data Patient Surveys
 Research Database Outcome measures for 12,581 eligible asthma patients Service Utilization Medication Compliance Appropriate Care Quality of Life (QoL) ACER Billing Data Medicaid Claims Spatial Data School Data Clinical Data Patient Surveys")
42
ACE Database: Data Collection Patient-Level Measures –Insurance –QoL Score –Visit History –Demographics –Medication Orders –Comorbid Conditions 42 Facility-Level Measures –Treatment Group –Intervention Dates Community-Level Measures Crime Poverty Education Housing values Access to services

43
Shared Decision Making Results 43 TimeNPrePost Chang eP-value 3 months (n=171)17118.70 % 9.40%-9.40%0.011 6 months (n=121)12131.40 % 23.10 % -8.30%0.114
 % 9.40%-9.40% months (n=121) % % -8.30%0.114")
44
AHRQ Asthma Population *Patients with first SDM visit in 2012Q1 or earlier

45
Appropriate Care Measures 45

Similar presentations



 Assessing.>")
 Lee Feb. 9 th, 2007.>")














 Where Louisiana Medicaid is Today and Where it Will To Be in the Future April 17, 2012.>")

