Download presentation
Presentation is loading. Please wait.

2
Retinal Detachment Abdulkrim Alkharashi, MD

3
RD History: 1. Theory of distension. 2. Theory of hypotony. 3. Theory of exudation. 4. Theory of retinal breaks. Causes of primary RD:-

4
RD History: cont. Beer – 1817 first to detect RD clinically. Von Helmholtz – 1851 invented the ophthalmoscope. Coccius – 1853 first to find retinal breaks (r.b.). De Wecker – 1870 first suggested that r.b. were the causes of RD.
. De Wecker – 1870 first suggested that r.b. were the causes of RD..")
5
RD History: cont. Leber – 1882 found r.b. in 70% of RD, vit. deg. and collapse traction r.b. RD. Changed to pre-retinal memb. r.b. (in PVR). Jules Gonin – 1919 Father of RD surgery. Performed the first RD operation to close r.b. – Ignipuncture of Thermocautery.
. Jules Gonin – 1919 Father of RD surgery. Performed the first RD operation to close r.b. – Ignipuncture of Thermocautery..")
8
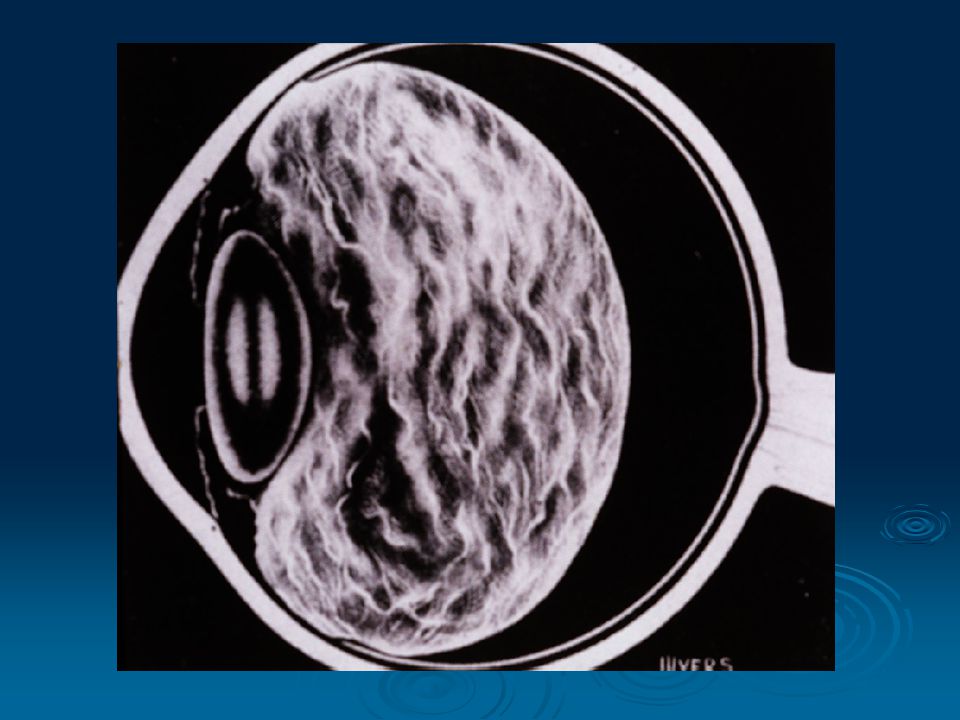
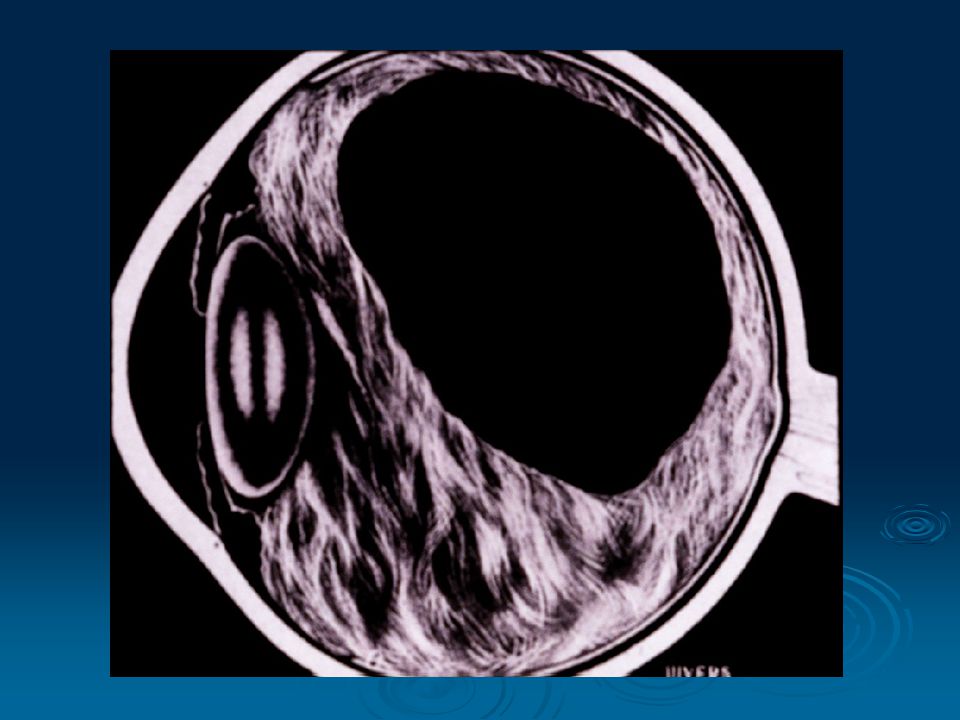
RD: Rhegmatogenous – Greek thegma = rent Tractional Exudative

9
RD Epidemiology: o Incidence 1: 10,000 / year. o In aphakics: 1– 3%. o In the second eye (-): 5%. o In the second eye (+): 10%. o 99% of untreated symptomatic RD blindness. o 5 – 15% of population with retinal break(s) 7% of these develop new break(s).
: 5%. o In the second eye (+): 10%. o 99% of untreated symptomatic RD blindness. o 5 – 15% of population with retinal break(s) 7% of these develop new break(s)..")
10
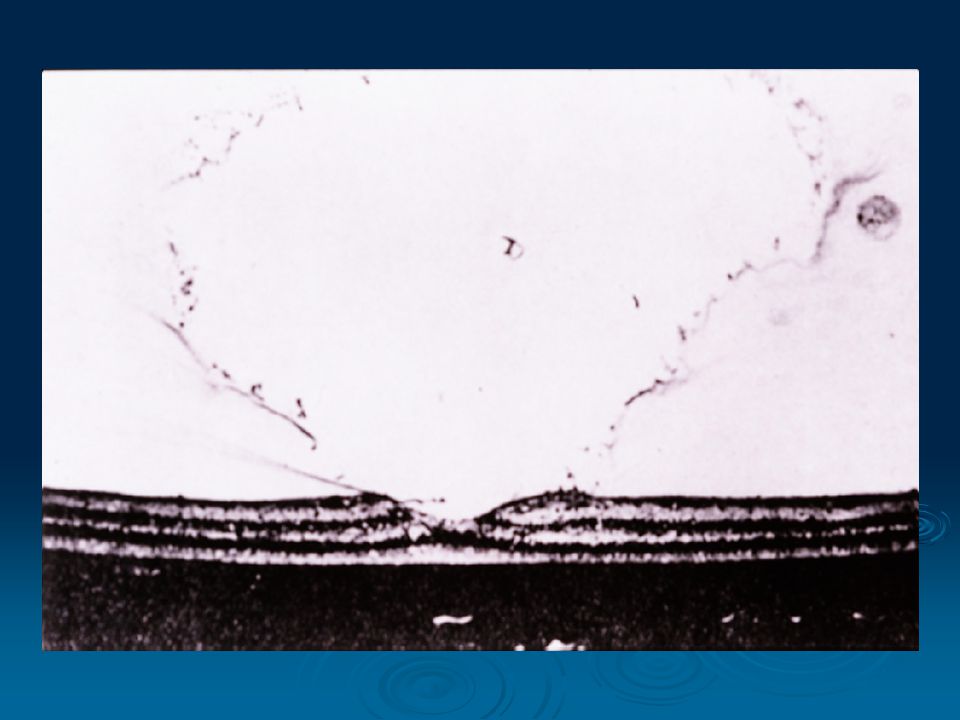
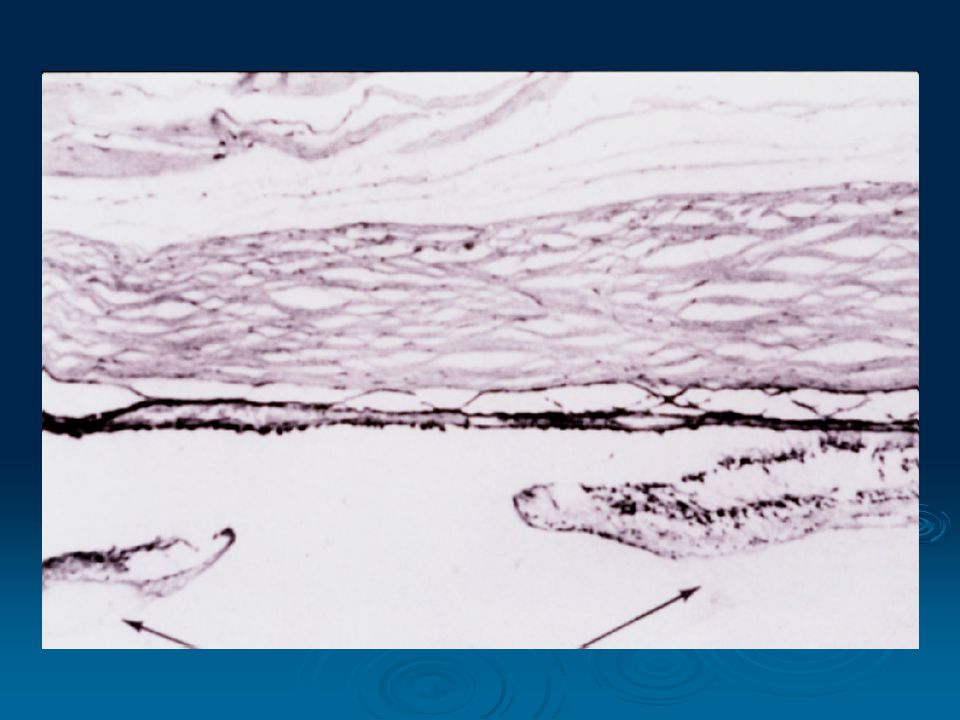
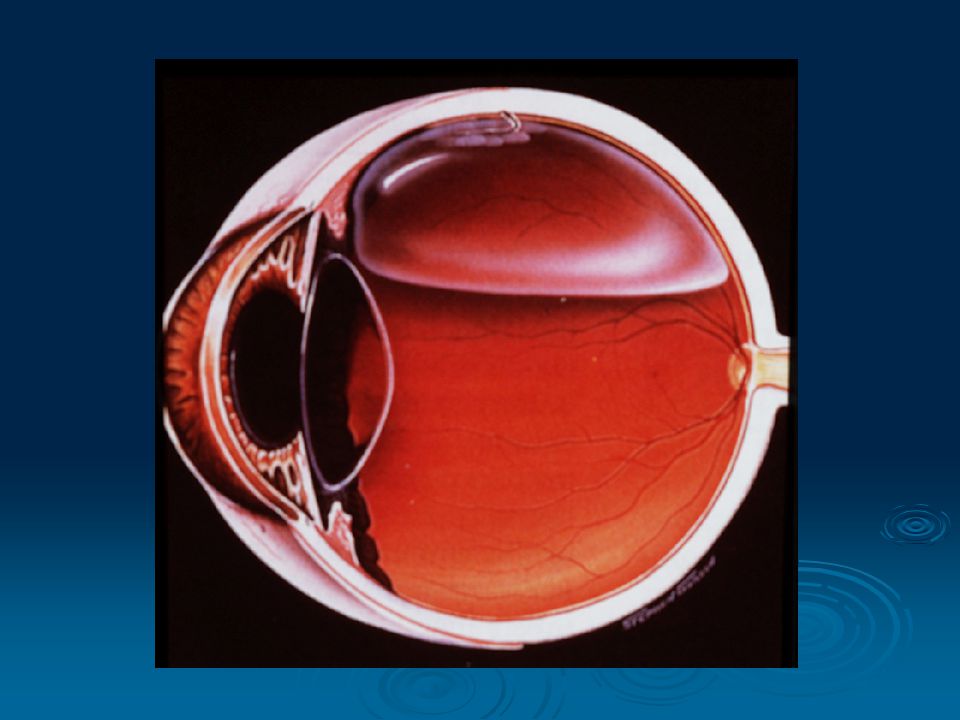
Rhegma. RD: Some degree of vitreous liquifaction. Retinal break: - tear - hole - hole - dialysis - dialysis Eye movements (Edie’s currents) PVD, V-R traction Pre-requisite:-
 PVD, V-R traction Pre-requisite:-.")
11
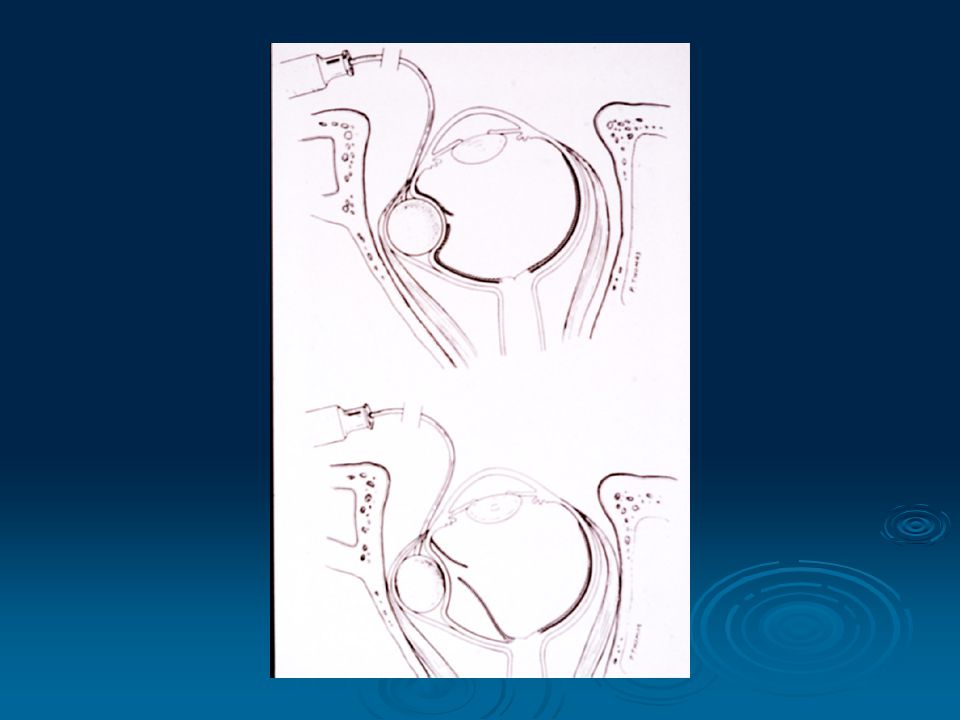
PVD _______________________________ Due to loss of hyaluronic acid collapse of vit. collagen with liquefaction. Rare before 30 yrs. Increases with age (63% in > 70 yrs.) Most PVDs are asymptomatic. 2 nd eye in 1 yr. 15% of acute PVD have a retinal tear (pathologic). Increases significantly after cataract extraction: pathologic vs. physiologic PVD.
 Most PVDs are asymptomatic. 2 nd eye in 1 yr. 15% of acute PVD have a retinal tear (pathologic). Increases significantly after cataract extraction: pathologic vs. physiologic PVD..")
12
RD 13-19% of PVD have vit. Hem. PVD + hem. 70% with tears. PVD + no hem. 2-4% with tears. PVD

19
RD F/U: Examine periphery. + vit. Hem. - rest, patching examine. - rest, patching examine. U/S. Acute PVD:-

20
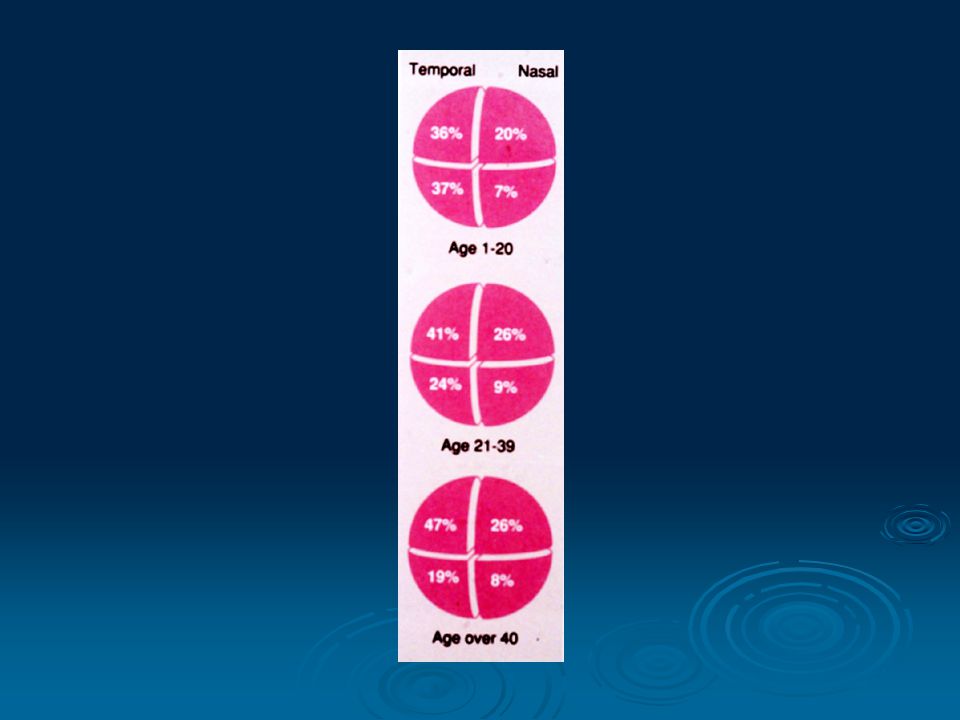
RD Risk Factors: Present in 8% of the population. In SA – 9.1% As a cause of RD in 20-30%. In RDs with L.D.:- 30-45% Atrophic holes. 30-45% Atrophic holes. 55-70% A tear at edge of L.D. 55-70% A tear at edge of L.D. 1. Lattice and other peripheral deg.:

29
RD Risk Factors: cont. > 6 D. 60 yr. myope risk of RD is 2.4% whereas normal risk 0.06% 2. High myopia:

30
RD Risk Factors: cont. Increases PVD: Does it convert physiological PVD to a pathological one? 1.3% RD in aphakes. ICCE > ECCE. Risk of RD increased with:- - P.C. otomy: 1.3%. - P.C. otomy: 1.3%. - Vit. loss. - Vit. loss. 50% of RDs in 1 st year. 3. Cataract surgery:

31
RD Risk Factors: cont. In general population – 1% COAG. In RD patients – 4-7% COAG. > in pigment dispersion synd. ? myopia. ? myopia. Miotics & RD. 4. Glaucoma:

32
RD Risk Factors: cont. 5. RD in fellow eye or F/H of RD. 6. Trauma.

34
RD Symptoms: PVD – flaches & floaters. Painless loss of peripheral VF. Painless loss of central vision.

35
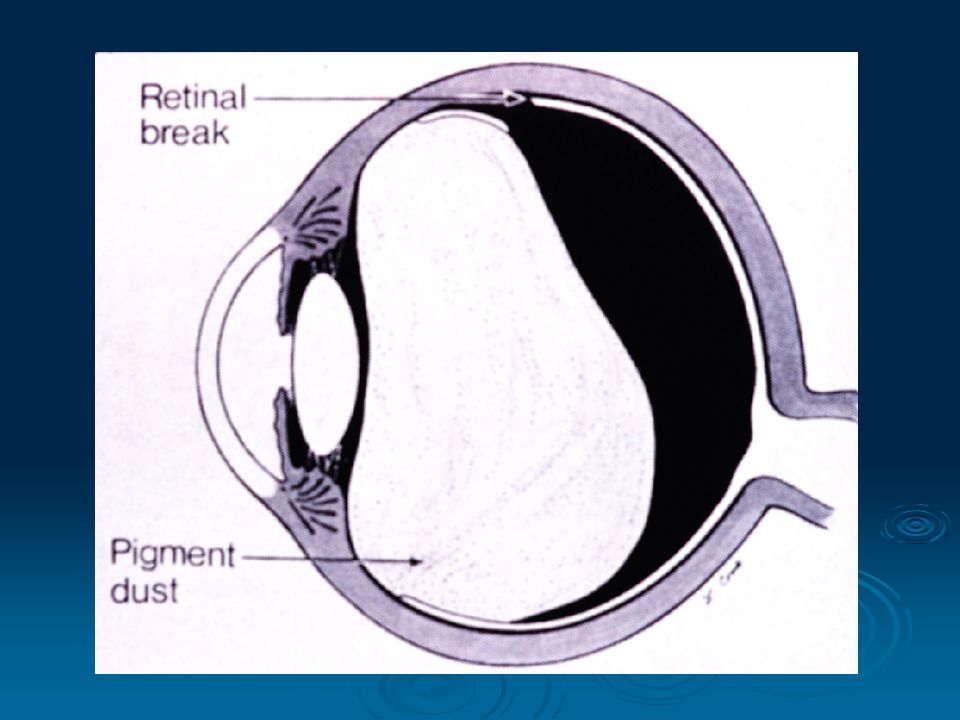
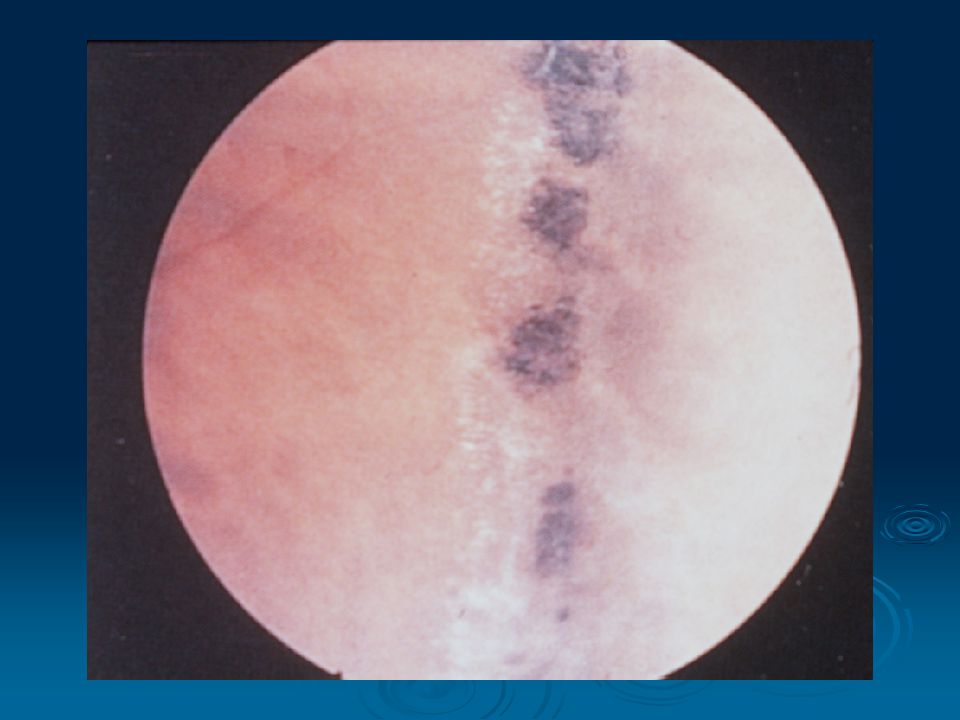
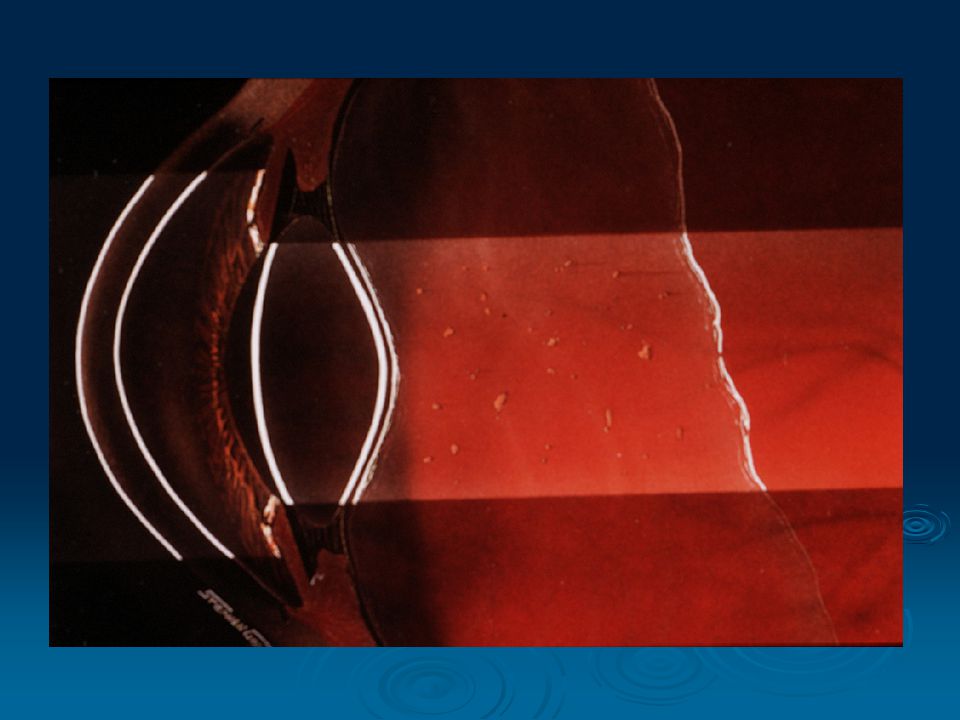
RD Examination: VA. IOP. SLE – blood, pigment (Shafer’s sign) in the vitreous. Careful binocular indirect ophthalmoscopy with scleral indentation. C.L. exam.

40
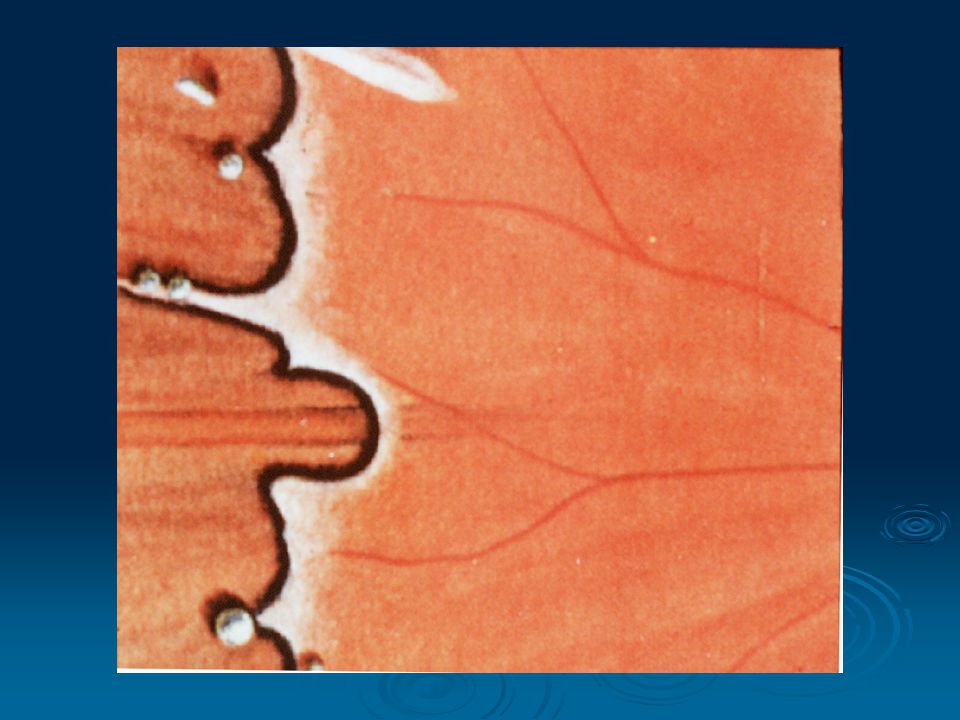
RD Types of Breaks: Fresh (acute) tear either:- Symptomatic tear. Symptomatic tear. Tear with retinal hem. at the edge. Tear with retinal hem. at the edge. A new tear in that location. A new tear in that location. Flap (horseshoe) tear. An operculated hole. Atrophic holes.
 tear. An operculated hole. Atrophic holes..")
43
RD DDX: Neoplasms. Inflammations – VKH, ICSC, post. Scleritis. Cong. Anomalies – optic pit, morning glory, choroidal coloboma, nanophthalmos, uveal effusion syndrome Exudative RD:-

44
RD DDX: cont. Traction RD. Retinoschisis – senile, juvenile. Choroidal detachment.

47
RD Treatment: Olny selected breaks require Rx. A symptomatic tear – caused by PVD or vit. Traction in the eye of a pt. C/O photopsias +/- floaters. Prophylactic Rx:-

48
Indications for Prophylactic Treatment of Retinal Tears and Holes in Symptomatic Patients: Flap tears Frequently (always) Operculated holes Sometimes Atrophic holes No Macular holes Rarely Lesion Treatment _____________________________________
 Operculated holes Sometimes Atrophic holes No Macular holes Rarely Lesion Treatment _____________________________________")
49
RD Treatment: Cryotherapy. Photocoagulation. Surround it ant. & post. Macular pucker. Tears at margins of Rx scar. Prophylactic Rx to breaks:-

50
RD Treatment: cont. Emergency. Localization of break(s). Creation of C-R adhestion around the break(s). Closure of break(s). Relief of V-R traction. Principles of Surgery:-
. Closure of break(s). Relief of V-R traction. Principles of Surgery:-.")
51
RD Treatment: cont. Scleral buckle. Orbital balloon. Pneumatic retinopexy. Primary vitrectomy + GFX, Long-term tamponade. LA/GA Surgical techniques:- Surgical techniques:-

58
RD prognosis & VA: 90-95% - Anatomic success. Overall 40-50% 20/50 or > 25% 20/60 – 20/100 25% 20/60 – 20/100 25% 20/200 or < 25% 20/200 or <

59
RD prognosis & VA: cont. If macula off. If macula off 1-8 wk – 50% 20/70 pr >. If macula on 90% Preop. VA pucker, CME, recurrent RD.

62
RD Prognosis: Detachments due to dialysis or to small or round holes. Detachments with demarcation lines. Detachments with minimal subretinal fluid. 1. Excellent prognosis (nearly 100%):
:.")
63
RD Prognosis: cont. Aphakic detachments. Total detachments. Detachments with associated detachment of the nonpigmented epithelium of the pars plana. Detachments caused by flap tears. 2. Slightly poorer prognosis (95%):
:.")
64
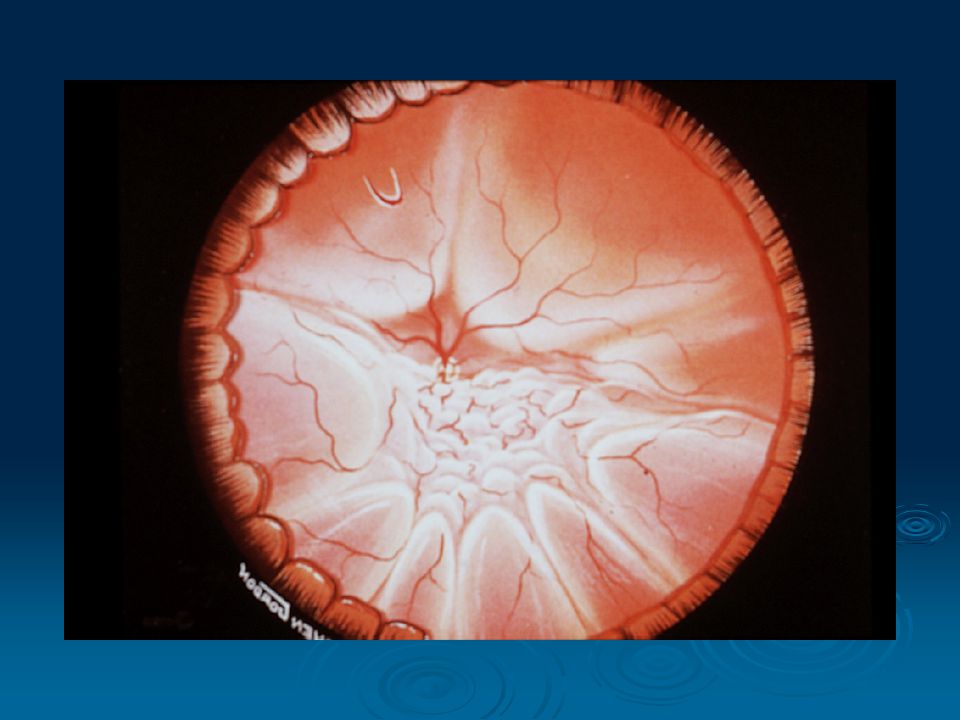
RD Prognosis: cont. Detachments with associated choroidal detachment Detachments with breaks larger than 180 . Detachments with PVR. Detachments in patients with stickler’s syndrome. Detachments caused by acute retinal necrosis. 3. Poor prognosis (50 to 70%):
:.")
Similar presentations































 Waxman MD PhD>")













(C.S.C)>")
 Dislocation M.R. Akhlaghi MD.>")
 occludes a branch of the central retinal vein Blockage causes bleeding from that branch Concerned about neovascularization.>")