Download presentation
Presentation is loading. Please wait.

1
The PMTP Phases of Care Active and Passive Care Prognosis MMI Adjusting Goals, Duration, and Frequency Physiotherapy selection

2
4/3/06 3-1-06

3
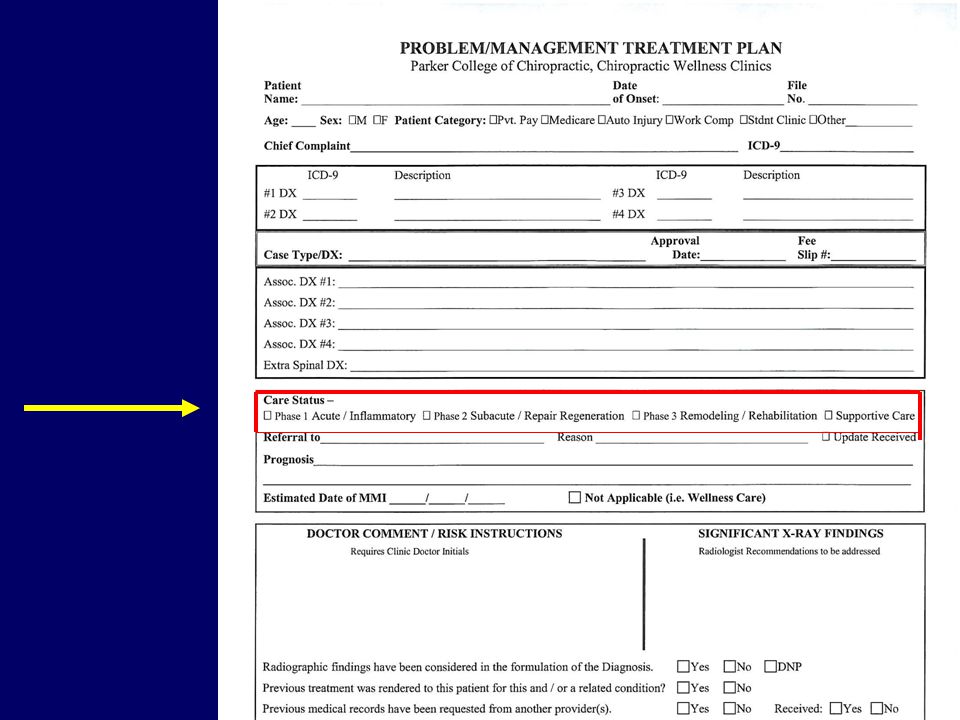
Care Status Phase of Healing Stage of Care Phase I Acute Inflammatory Phase II Repair / Regeneration Phase III Rehab / Remodeling

4
Phase IPhase IIPhase III AcuteRegenerationRemodeling InflammationRepairRehab Mild 2 days Moderate 3-4 days Moderate to severe 7 days Mild to moderate 6 weeks Moderately severe up to 16 wks. Mild 2-3 weeks Moderate 4-8 weeks Moderately severe up to 1 yr. Medicine and Science in Sports and Exercise Examples of Time frames for mild, moderate, and moderately severe conditions and phases of healing.

5
Phase IPhase IIPhase III AcuteRepairRemodeling InflammatoryRegenerationRehab PASSIVE CARE ACTIVE CARE decreases increases Time / Number of Visits Passive / Active Care Examples

6
4/3/06 3-1-06

7
Zeroing in on Prognosis

8
Prognosis Prognosis: What your patient can expect. You forecast as to the probable outcome of their condition. One word descriptions (Good -Poor) are inadequate, offer no explanation as to evidence to support the prognostic conclusion, and are unacceptable.
 are inadequate, offer no explanation as to evidence to support the prognostic conclusion, and are unacceptable..")
9
Prognosis Arriving at a technically certain prognosis after the initial exam may not be possible especially during the acute phase.

10
This patient is in the acute phase of care. Prognosis is deferred until the response to the initial therapeutic trial is determined by progress exam in 4 wks 4/3/06 3-1-06

11
Prognosis deferral Acute Phase Prognosis is deferred until the patient’s response to the initial therapeutic trial has been determined by progress examination in approximately 4 weeks.

12
Good Prognosis Example The prognosis is good and is based upon – excellent patient compliance in keeping appointments (11/12 kept) and performing home therapy – reduction in pain scores from 6 to 3, – improvement in the NDI from 42% to 18%, – and substantially improved cervical range of motion.
 and performing home therapy – reduction in pain scores from 6 to 3, – improvement in the NDI from 42% to 18%, – and substantially improved cervical range of motion.")
13
Fair Prognosis Example The prognosis in this case is currently considered fair based upon the following: –There were (4) previous episodes of low back pain resulting in loss of work time and light duty restrictions over the past 3 years. –Mild obesity, deconditioning syndrome, and smoking 2 packs of cigarettes / day for past 5 years. –Pain score improvement from 6/10 to 3/10. –Low back Oswestry score improved from 48% to 30%. –9/12 appointments kept over the last therapeutic trial

14
Poor Prognosis Example The prognosis in this case is poor in consideration of the following: –Non-compliance with the agreed upon treatment plan, missing 6/10 appointments. –Non-compliance with the agreed upon home exercise program. –Obesity and moderately severe de-conditioning syndrome. –Diabetes and non-compliance with diet and nutritional recommendations. Document in SOAP notes

15
Poor Prognosis Example The prognosis in this case is poor due to the following: –Low back Oswestry score is 58%, indicating a moderately severe patient perception of disability performing routine activities of daily living. –Moderately severe degenerative disc disease L5/S1 with attendant radiculopathy of the right lower extremity –Decreased coordination, strength, sensation, and proprioreception of the right lower extremity.

16
UNACCEPTABLE PROGNOSIS EXAMPLE The prognosis in this case is good with patient compliance The above Prognosis is unacceptable MUST ANSWER THE QUESTION: WHY?

17
Prognosis One word prognosis is unacceptable. Prognosis is good with patient compliance is unacceptable –ADD THE WORD “BECAUSE” –THINK OF THE PHRASE “BECAUSE OF THE FOLLOWING” –…DUE TO THE FOLLOWING FACTORS / OBJECTIVE FINDINGS –YOU MUST DOCUMENT YOUR REASON(S).
..")
18
This patient is in the acute phase of care. Prognosis is deferred until the response to the initial therapeutic trial is determined by progress exam in 4 wks 3-1-06 In some cases, if you cannot reasonably forecast the patient’s anticipated response to care (the PROGNOSIS) especially during he acute phase based upon a one time exam, how can one be reasonably certain regarding the date of MMI?
 especially during he acute phase based upon a one time exam, how can one be reasonably certain regarding the date of MMI .")
19
MMI Maximum Medical Improvement The patient’s condition is static and stable. Patient symptoms, your objective exam findings, and Outcome Assessments show little or no improvement after 2 progress exams.. When further care does not bring about OBJECTIVE MEASURABLE IMPROVEMENT! The patient may then be a candidate for supportive care.

20
Supportive / Palliative Care Treatment rendered after achieving maximum medical / therapeutic benefit. Periodic trials of withdrawal from care fail to sustain previous treatment gains. Excluded from Medicare coverage. Not considered medically necessary. –Excluded from most insurance policy coverage

21
MMI DOES NOT MEAN RELEASING THE PATIENT WITH A PAIN SCORE OF 0, OR AN OSWESTRY SCORE OF 0%, OR WITH NORMAL R.O.M MEASUREMENTS CONFIRMED BY YOUR INCLINOMETER! Maximum Therapeutic Benefit (MMI?): when there are NO DETECTABLE measurable changes (improvements) identified over the course of 2 therapeutic trials as determined by 2 progress exams AND OUTCOME ASSESSMENTS
: when there are NO DETECTABLE measurable changes (improvements) identified over the course of 2 therapeutic trials as determined by 2 progress exams AND OUTCOME ASSESSMENTS.")
22
MMI Uncomplicated Case An uncomplicated mild to moderate ankle sprain –6 WEEKS OF CARE ESTIMATED –OPPORTUNITY TO SEE THE PATIENT THROUGH THE 3 PHASES OF HEALING –ESTABLISH THE MMI DATE ABOUT 6 WEESK OUT FROM THE BEGINNING CARE.

23
MMI Date for Complicated Case Low back pain 6/10, Oswestry score 50% Moderately severe DDD L5S1 with weakness of the R LE Overweight smoker with significant deconditioning Acute on chronic condition with PMHX of multiple disabling events, Compliance to home therapy, nutrition, and in-office care is fair, keeping 7/10 appts. Anticipated MMI date 16-24 weeks out from initial care, pending results of further diagnostic testing, referrals, and measurable change to Outcome Assessments.

24
Establishing an MMI date 1.Determine if it is a mild, moderate, or moderately severe condition. 2.Are there complicating factors that adversely affect prognosis? 3.Is the patient compliant with home care and keeping appts? 4.It is better to select an MMI date a little further out and releasing the patient early, than to repeatedly miss the mark you select (target date)
.")
25
DOCUMENT THE PROGNOSIS AND MMI DATE AS SOON AS REASONABLY POSSIBLE 1.During the initial exam or 2.At the time of the the first progress exam 3.The prognosis may be updated / changed based upon the availability of new information

26
MMI Maximum Medical (Chiropractic) Improvement is determined by the results of all of the components of your examination –Ortho –Neuro –ROM –Strength –Outcome Assessments / effects on ADL AS WELL AS HOW YOU SET UP YOU TREATMENT PLAN AND TX GOALS!
 Improvement is determined by the results of all of the components of your examination –Ortho –Neuro –ROM –Strength –Outcome Assessments / effects on ADL AS WELL AS HOW YOU SET UP YOU TREATMENT PLAN AND TX GOALS!")
27
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (739.1) and the lumbar spine at L5 (739.3). Begin Diversified adjusting week 2, after acute pain and spasm have been reduced 3 times per week for 3 weeks

28
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment

29
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment Ultrasound-pulsedReduce acute inflamm / swelling3x week for 1 week 97035

30
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential97014High and low frequency for pain modulation and swelling / inflammation, and muscle spasm 3x week for 2 weeks 97035

31
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential97014High and low frequency for pain modulation and swelling / inflammation, and muscle spasm 3x week for 2 weeks Muscle Spasm Violent involuntary contraction of muscle attended by pain and interference of function. An ACUTE phenomenon. Mostly commonly seen the 1 st week post trauma, and resolved within a few weeks. Possibly seen and palpated during an acute on chronic episode. If muscle spasm is commonly documented during the subacute (repair regeneration) phase and the rehab (remodeling) phase, it lessens the credibility of the provider and may trigger a fraud investigation by 3 rd party payors. Muscle spasms that occur 4, 6, and 10 weeks into the treatment plan would be extremely rare and may require referral, and minimally an advanced neurological examination 97035
 phase and the rehab (remodeling) phase, it lessens the credibility of the provider and may trigger a fraud investigation by 3 rd party payors. Muscle spasms that occur 4, 6, and 10 weeks into the treatment plan would be extremely rare and may require referral, and minimally an advanced neurological examination")
32
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential97014High and low frequency for pain modulation and swelling / inflammation, and muscle spasm 3x week for 2 weeks 97014 EMS unattended 97032 EMS attended / manual- applied by the hand of the therapist requiring constant attendance for therapy to take place 97035

33
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential97014High and low frequency for pain modulation and swelling / inflammation nd muscle spasm 3x week for 2 weeks Soft foam cervical collar.Verbal and written instructions supplied DATE Cold pack. Written and verbal instructions supplied DATE

34
Intern signature legible! ALWAYS 7 + 6 + 8 = 21 / 3 = 7 QVAS score

35
Reduce and stabilize joint dysfunction of the cervical spine at C2 and C5 (7391.) and the lumbar spine at L5 (739.3). Begin Diversified adjusting 2 nd week of treatment after acute pain has been reduced and stabilized. 3 times per week for 3 weeks Joint mobilization97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential97014High and low frequency for pain modulation and swelling / inflammation 3x week for 2 weeks Soft foam cervical collar.Verbal and written instructions supplied DATE Cold pack. Written and verbal instructions supplied DATE 7/10 Reduce QVAS from 7 to 5 in 4 weeks (achieve this goal on or before the progress exam See entire acute care tx plan above

36
Intern legible signature My back and neck hurt me more when I try to get in and out of my car C2C2 C2C2 F5F5 D3D3 D3D3 D3D3 D3D3 D3D3 C2C2 D3D3

37
Intern legible signature My back and neck hurt me more when I try to get in and out of my car C2C2 C2C2 F5F5 D3D3 D3D3 D3D3 D3D3 D3D3 C2C2 D3D3 27 pts X 2= 54 54% Oswestry Disability Score

38
Joint mobilization 97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential 97014 High and low frequency for pain modulation and swelling / inflammation 3x week for 2 weeks Soft foam cervical collar.Verbal and written instructions supplied DATE Cold pack. Written and verbal instructions supplied DATE 7/10 Reduce QVAS from 7 to 5 in 4 weeks (achieve this goal on or before the progress exam See entire acute care tx plan above Oswestry Low Back Disability Score DATE 54% Improve patient comfort and safety transfer in and out of their car ADL training975351x per week for 2 weeks 97035

39
Legible intern signature DATE ALWAYS

40
Legible intern signature DATE ALWAYS 28 pts X 2 = 56% NDI score

41
Joint mobilization 97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential 97014 High and low frequency for pain modulation and swelling / inflammation 3x week for 2 weeks Soft foam cervical collar.Verbal and written instructions supplied DATE Cold pack. Written and verbal instructions supplied DATE 7/10 Reduce QVAS from 7 to 5 in 4 weeks (achieve this goal on or before the progress exam See entire acute care tx plan above Oswestry Low Back Disability Score DATE 54% Improve patient comfort and safety transfer in and out of their car ADL training975351x per week for 2 weeks 97035 Neck Disability Index56%

42
There are a lot of Activities of Daily Living issues with this case as documented by the Oswestry and NDI. In the ACUTE phase, it is better to focus on helping them with the reachable and critical necessities Self care Driving – transfer in and out of vehicle Sitting- getting in and out of chair Recreational activities and lifting heavier objects are examples that may be addressed in later phases with active care / rehab. currently Goal to achieve by progress exam date

43
Joint mobilization 97140 3x week for 1 week Gently increase intersegmental ROM, pump out inflamm exudates, prepare joints for grade V manipulation / adustment UltrasoundReduce acute inflamm / swelling3x week for 1 week EMS- Interferential 97014 High and low frequency for pain modulation and swelling / inflammation 3x week for 2 weeks Soft foam cervical collar.Verbal and written instructions supplied DATE Cold pack. Written and verbal instructions supplied DATE 7/10 Reduce QVAS from 7 to 5 in 4 weeks (achieve this goal on or before the progress exam See entire acute care tx plan above Oswestry Low Back Disability Score DATE 54% Improve patient comfort and safety transfer in and out of their car ADL training975351x per week for 2 weeks 97035 Neck Disability Index56% To look after herself normally despite pain by the next progress exam ADL Training-verbalize and demonstrate ability to perform 97535 1x and re-evaluate in 1 week. See SOAP notes for additional ADL info.

44
Acute Inflammatory Phase Activity restrictions / work restrictions –Based upon exam findings, outcome assessments, job description etc. Short term immobilization and bracing –Collar, belt, rest Reduce inflammation and pain –Home therapy –Physiotherapy –Nutritional intervention Document advice / ADL instructions Adjusting vs. mobilization (joint motion w/o thrust)
.")
45
PMTP Example Phase II Repair- Regeneration

46
PMTP Example Repair Regeneration Phase II Low back patient –Prognosis –Adjusting goals –Outcome Assessments Treatment plan Treatment goals

47
Intern signature legible! ALWAYS 4 + 4 + 7 = 15 / 3 = 5 QVAS score

48
Legible signature 40% Oswestry Score 2 1 4 2 2 2 1 3 1 2 My back hurts more and feels weak when I lift and care for my 2 y/o baby

49
Prognosis to date is good based upon excellent compliance to the treatment plan, approx 50% improvement in ROM, fewer + orthopedic tests, reduction in pain, Oswestry, and Neck Disability Index scores. Biomechanical and structural pathology from Rad report goes here. Will this info affect the prognosis? Are any of these findings worthy of making it up to the Diagnosis section

50
Prognosis to date is good based upon excellent compliance to the treatment plan, approx 50% improvement in ROM, fewer + orthopedic tests, reduction in pain, Oswestry, and Neck Disability Index scores. Biomechanical and structural pathology from Rad report goes here. Will this info affect the prognosis? Are any of these findings worthy of making it up to the Diagnosis section CVA/ cardiovascular risk Safety issues collected from outcome assessment data. Work / recreational issues – re-injury / joint protection

51
Reduce moderately severe alterations in joint endplay hypomobility (739.3) at L4. 3x week for 4 weeks

52
Reduce moderately severe alterations in joint endplay hypomobility (739.3) at L4. 3x week for 4 weeks EMS - Interferential 970143x week for 2 weeksFor pain control

53
Reduce moderately severe alterations in joint endplay hypomobility (739.3) at L4. Increase intersegmental and global ROM per clinical exam and inclinometry ROM testing 3x week for 4 weeks EMS - Interferential970143x week for 2 weeksFor pain control Therapeutic exercises97110Increase ROM and, strength2x week for 4 weeks

54
If your examination documents loss of strength, endurance, range of motion, or flexibility, the selection and performance of 97110 may be considered medically (chiropractically) necessary. It would not be appropriate to select 97110 to decrease pain. 97110therapeutic exercises to develop strength and endurance, range of motion and flexibility, one or more areas, each 15 minutes

55
Reduce moderately severe alterations in joint endplay hypomobility (739.3) at L4. Increase intersegmental and global ROM per clinical exam and inclinometry ROM testing 3x week for 4 weeks EMS - Interferential970143x week for 2 weeksFor pain control 5Reduce QVAS score to 3. Decrease pain at its worst from 7 to 5 in 4 wks. EMS – Interferential Therapeutic exercises97110Increase ROM, flexibility, strength2x week for 4 weeks 97014 3x week for 2 weeks

56
Legible signature 40% Oswestry Score 2 1 4 2 2 2 1 3 1 2 My back hurts more and feels weak when I lift and care for my 2 y/o baby

57
EMS - Interferential 970143x week for 2 weeksFor pain control 5 Reduce QVAS score to 3. Decrease pain at its worst from 7 to 5 in 4 wks. Therapeutic exercises97110Increase ROM, flexibility, strength 2x week for 4 weeks Oswestry Score 40% The pt. will demonstrate the ability to safely lift her 2 y/o baby using proper mechanics and joint protection ADL training975351x per week for 2 weeks

58
Legible signature ADL Issues *Lifting *Walking *Standing

59
Don’t Ignore Documented ADL issues It would be appropriate to address some of these ADL issues during Phase II Repair Regeneration Phase of Care / Healing –Walking –Standing –Lifting?

60
Oswestry Score 40% The pt. will demonstrate the ability to safely lift her 2 y/o baby using proper mechanics and joint protection ADL training 97535 1x per week for 2 weeks Oswestry Low Back Score40% Improve walking and standing tolerances (endurance). NOTE: LIFTING HEAVIER WEIGHTS MAY BE AN INNAPROPRIATE GOAL DURING PHASE II HEALING AND CAUSE FURTHER INJURY. PHASE II SHOULD BE PREPARATION FOR MORE AGGRESSIVE EXERCISE IN PHASE III Therapeutic exercises 97110 2x week for 4 weeks Improve walking and standing tolerances (endurance). Demonstrate ability to lift 1.5 x the weight of her baby from the floor and various elevations up to waist level.
. NOTE: LIFTING HEAVIER WEIGHTS MAY BE AN INNAPROPRIATE GOAL DURING PHASE II HEALING AND CAUSE FURTHER INJURY. PHASE II SHOULD BE PREPARATION FOR MORE AGGRESSIVE EXERCISE IN PHASE III Therapeutic exercises x week for 4 weeks Improve walking and standing tolerances (endurance). Demonstrate ability to lift 1.5 x the weight of her baby from the floor and various elevations up to waist level..")
61
Phase II Repair Regeneration Phase Adjustments Physiotherapy –EMS –Microcurrent –Traction –Soft tissue work – ischemic compression Therapeutic exercises –Home therapy / stretches –ROM exercises, isometrics –ADL activity improvements This phase represents a combination of passive and active care.

62
Phase III Rehab Remodeling

63
PMTP Example Rehab / Remodeling Phase Example –Prognosis –Adjusting goals –Outcome Assessments Treatment plan Treatment goals

64
PMTP Example Areas involved: Lumbar spine Severity: Mild to Moderate Outcome Assessments –QVAS (Quadruple Visual Analog Scale) –Oswestry (Low back)
 –Oswestry (Low back)")
65
Prognosis is good based upon a 50% improvement in the pain score and Oswestry score the past 4 weeks. ROM has improved in all planes except lumbar extension. Lumbar neural tension signs are negative. This patient is ready for an aggressive rehab / conditioning program.

66
Cervical spine joint dysfunction (739.1) has resolved. Continue CMT to lumbar spine level L5 (739.3) to improve intersegmental ROM and reduce the 2mm retrolisthesis at this level. 1x week for 4 wks
 to improve intersegmental ROM and reduce the 2mm retrolisthesis at this level. 1x week for 4 wks.")
67
Cervical spine joint dysfunction (739.1) has resolved. Continue CMT to lumbar spine level L5 (739.3) to improve intersegmental ROM and reduce the 2mm retrolisthesis at this level. 1x week for 4 wks Therapeutic exercises 97110Develop strength, ROM and flexibility3x week for 4 wks
 to improve intersegmental ROM and reduce the 2mm retrolisthesis at this level. 1x week for 4 wks Therapeutic exercises 97110Develop strength, ROM and flexibility3x week for 4 wks.")
68
Cervical spine joint dysfunction (739.1) has resolved. Continue CMT to lumbar spine level L5 (739.3) to improve intersegmental ROM and reduce the 2mm retrolisthesis at this level. 3 1x week for 4 wks Improve pain at its worst from a 6 to a 3 CMT-Adjustment989401x week for 4 weeks Therapeutic exercises 97110Develop strength, ROM and flexibility
 to improve intersegmental ROM and reduce the 2mm retrolisthesis at this level. 3 1x week for 4 wks Improve pain at its worst from a 6 to a 3 CMT-Adjustment989401x week for 4 weeks Therapeutic exercises 97110Develop strength, ROM and flexibility.")
69
Legible signature 32% Oswestry 1 0 4 2 3 2 1 1 1 1

70
It is common for OT’s and PT’s to select the next letter or two up as a target goal to achieve by the next progress exam

71
3 Improve pain at its worst from a 6 to a 3 Oswestry Score 32% Improve to lifting heavier objects that are conveniently positioned. Improve walking tolerance to ½ mile or 20 mins; improve sitting tolerance to 1 hour Therapeutic exercises971103x week for 4 weeks. Gradually increase exercise time to 30 minutes. See SOAP notes for addtl data ? For post workout soreness, home stretches etc? CMT - adjusting 989401x week for 4 weeks

72
Phase III Rehab Remodeling Phase Adjustments less frequent. Generally not in the 3x week mode. Minimal to no physiotherapy modalities Active care: ROM exercises, stretches Weight machines Tubing exercises, exercise ball Balance boards, proprioreception, Treadmill, exercise bike, upper body ergonometer

73
Phase IPhase IIPhase III AcuteRepairRemodeling InflammatoryRegenerationRehab PASSIVE CARE ACTIVE CARE decreases increases

74
Acute on Chronic Reduce and stabilize the acute episode Move the patient through the phases of care / healing. Get them to the rehab phase as quickly as possible, not jeopardizing pt. health, joint integrity, or cause further re-injury.

76
Clinic Fee Update Examples 98940 CMT 1-2 areas$10$20 98941 CMT 3-4 areas$12$23 98942 CMT 5-6 areas$13$26 98943 CMT extraspinal$10$16 Police Fire Active Duty

77
Clinic Fee Update Examples Therapy –97010 hot pack / cold pack $7 $10 –97012 posture pump / wedge$7 $10 –97014 muscle stim unattended$7 $10 –97032 muscle stim attended $7 $10 –97035 ultrasound$7 $13 –97140 Myofascial trigger point$7 $13 Percussor$7 $13 –

78
Clinic Fee Update Examples Active Therapy –97110 therapeutic exercise$7$15 –97112 neuromuscular re-ed.$7$15 –97535 ADL / self care$7$15

79
ROF Visit The ROF is typically performed on the 2 nd or possibly in some cases the 3 rd visit. Performing a Report of Findings on the initial visit may be possible and advisable in rare cases, and would represent the exception, not the rule.

80
Clinic Fee Update 99213 E/M code for Report of Findings –To be used if the ROF is performed on the 2 nd or 3 rd visit –SOAP notes must be documented thoroughly Total time spent. Begin time and end time What was discussed? –Hx, CC, exam, x-ray, restrictions, nutrition, exercise, DX, prognosis Document patients questions and concerns Acceptance of tx plan –A one line sentence indicating that a ROF was performed is inadequate documentation and will no longer be accepted. Credit will not be approved for that visit unless the ROF visit is thoroughly documented.

81
Report of Findings Visit –SOAP notes must be documented thoroughly Total time spent. Begin time and end time What was discussed? –Hx, CC, exam, x-ray, restrictions, nutrition, exercise, DX, prognosis Document patients questions and concerns Acceptance of tx plan –A one line sentence indicating that a ROF was performed is inadequate documentation and will no longer be accepted. Credit will not be approved for that visit.

82
Clinic Update Dr. Thomas Professional Behavior Physical Contact –Clinic Staff –Patients

Similar presentations