Download presentation
Presentation is loading. Please wait.

2
Project Review and Qualitative Process Findings 2007-2010 March 2010 Improving access to health services for vulnerable populations

4
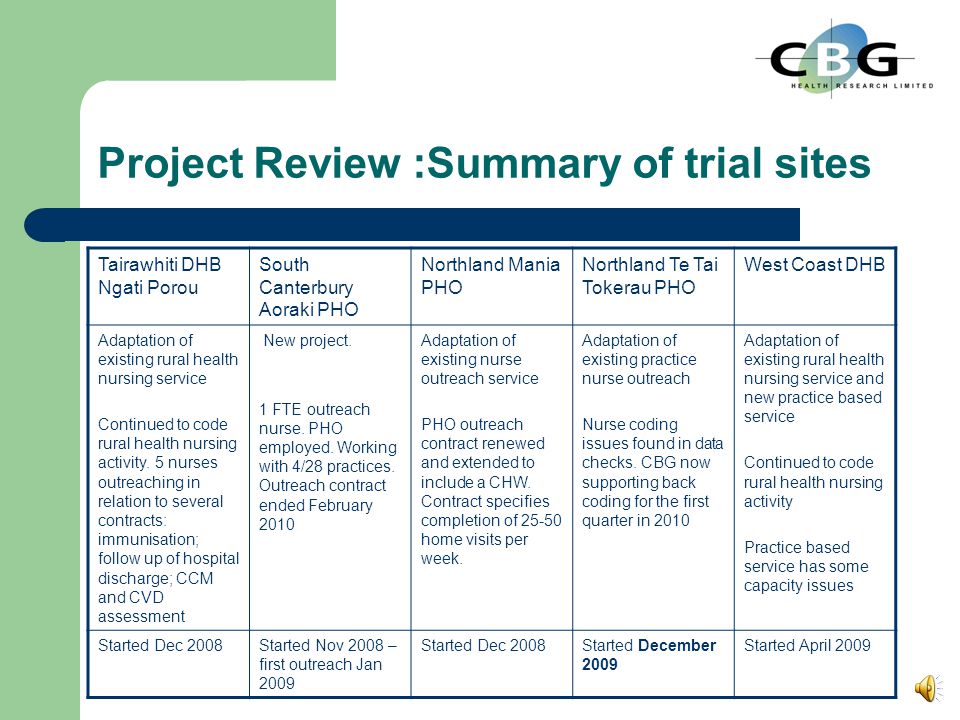
Project Review :Summary of trial sites Tairawhiti DHB Ngati Porou South Canterbury Aoraki PHO Northland Mania PHO Northland Te Tai Tokerau PHO West Coast DHB Adaptation of existing rural health nursing service Continued to code rural health nursing activity. 5 nurses outreaching in relation to several contracts: immunisation; follow up of hospital discharge; CCM and CVD assessment New project. 1 FTE outreach nurse. PHO employed. Working with 4/28 practices. Outreach contract ended February 2010 Adaptation of existing nurse outreach service PHO outreach contract renewed and extended to include a CHW. Contract specifies completion of 25-50 home visits per week. Adaptation of existing practice nurse outreach Nurse coding issues found in data checks. CBG now supporting back coding for the first quarter in 2010 Adaptation of existing rural health nursing service and new practice based service Continued to code rural health nursing activity Practice based service has some capacity issues Started Dec 2008Started Nov 2008 – first outreach Jan 2009 Started Dec 2008Started December 2009 Started April 2009

5
Description of the trial 2. Maximise value of each contact BPAC form – Identification of overdue basic care 3. Cultural awareness training 1. Target outreach Query and PMS information use Listed any registered patients with evidence of asthma, diabetes or ischaemic heart disease who have not been seen in the last 6 months. – Date of last recorded encounter – All Read codes for these conditions – Any prescription for Hypoglycaemic medicines Vasodilating nitrates Inhaled steroids or combination inhalers

6
Outreach activity to date Figures to March 2010

7
Qualitative Process Evaluation Discussions focused on the process of delivering the service, more specifically – Process and operation details – Identification of events that may have affected implementation or outcomes. – Next steps/improvements Interviews completed October 2009 – February 2010

8
Findings Stocktake, literature review and formative findings available at www.improving access.co.nz

9
Targeting outreach and maximising the value of each contact Few nurses use the PMS effectively Outreach has largely been referral led with limited checking of eligibility Reasons 1. Nurse attitude towards delivering health care in the home 2. Home visits criteria 3. Employment status 4. Use of IT 5. Capacity issues

10
Nurses attitude towards offering health care in the home Exposure to home environments – Some nurses reluctant to, or unsure about how and when, to approach health issues – Confronted with socioeconomic problems Involvement is time consuming Not necessarily qualified to deal with the issues Transition to health care – Not smooth – Not always possible Uncertainty about when to approach health issues – Embroiled in some situations – Provider, rather than facilitator of access to, services – Struggle to replace themselves in the service equation “ You have to prove yourself when you get in there – Show that you are going to help. Sort out their benefits so that they can pay for care. You can’t plough in there asking to take their blood pressure – Not right away!’

11
Where Home visit criteria exists Criteria varied across the sites – Commonly included recall checks – Related to underlying contract requirements – Typically included one or more of the following: Did not attend secondary care appointment (list provided by the hospital) Recently discharged from hospital (Electronic discharge summary sent to PMS) Avoidable hospital admission (List provided by the DHB) Overdue screen, immunisation, diabetes follow up (queries run in the PMS) No CVD risk assessment recorded (PHO generated list) Palliative care (referral from a practitioner) CCM programme (List of those eligible from PHO)
 Recently discharged from hospital (Electronic discharge summary sent to PMS) Avoidable hospital admission (List provided by the DHB) Overdue screen, immunisation, diabetes follow up (queries run in the PMS) No CVD risk assessment recorded (PHO generated list) Palliative care (referral from a practitioner) CCM programme (List of those eligible from PHO)")
12
Run PMS queries Generate a list of potential outreach recipients Assess the list through PMS record check and use of professional’s knowledge about the family Confirm reason for outreach activity or home visit NoYes Adjust PMS record accordingly (e.g. correct coding) Code outreach in the PMS and complete PMS record results in Receive referrals Complete recall. In the event of no response Complete outreach activity Referral Based Nursing Outreach Start Run PMS queries Generate a list of potential outreach recipients Assess the list through PMS record check and use of professional’s knowledge about the family Confirm reason for outreach activity or home visit NoYes Adjust PMS record accordingly (e.g. correct coding) End : Code outreach in the PMS and complete PMS record Start Receive referrals Complete recall. In the event of no response Complete outreach activity Some referrals will not meet the trial eligibility criteria For example: Those seen at the clinic and referred for follow up
 Code outreach in the PMS and complete PMS record results in Receive referrals Complete recall. In the event of no response Complete outreach activity Referral Based Nursing Outreach Start Run PMS queries Generate a list of potential outreach recipients Assess the list through PMS record check and use of professional’s knowledge about the family Confirm reason for outreach activity or home visit NoYes Adjust PMS record accordingly (e.g. correct coding) End : Code outreach in the PMS and complete PMS record Start Receive referrals Complete recall. In the event of no response Complete outreach activity Some referrals will not meet the trial eligibility criteria For example: Those seen at the clinic and referred for follow up.")
13
Employment status PHO employed – Protected time to deliver the service – Work across a number of practices – Estimate 1FTE can work across 10-14 GPs or patient population of 20- 30,000 Require help to judge eligibility – More likely to accept all referrals at face value – Takes time for referees to understand the service Practice employed – More likely to be prohibited from outreaching by other duties – Have the trust of the practice Know the patients so can judge eligibility

14
Use of IT Use PMS to identify those eligible for outreach Use best practice reports to identify / address overdue aspects of care Code all outreach activity In addition to good PMS record keeping. The trial required outreach nurses to:

15
Use of IT: Findings Use PMS to identify Queries abandoned Many referrals accepted at face value with little interrogation of PMS Use best practice reports to identify / address overdue aspects of care 1 in 3 did not use the report facility Code all outreach Activity 1 in 5 did not correctly code PMS record keeping. Some clinical information is incorrectly entered as free text Some referrals are not recorded in the PMS Some nurses use external software to provide outreach reports Reasons: Varied understanding, no adoption of new practice, preferences for more traditional practice/referrals based service

16
Capacity Large variation in number of calls, visits and other activities accomplished by 1 FTE per week – Predominantly associated with underlying contract and employment arrangements 1. “I complete 4-5 visits in two and a half days” [PHO employed working across 2 practices with limited management support and no activity requirements specified in the service contract] 2. “We have done about 30 visits in the last couple of months – To be honest I have been busy with other things. We are one practice nurse down and we are just trying to fit this in when we can.” [Practice nurses with no activity requirements specified in the service contract] 1. “About 4-5 visits a day –most weeks it would be 20-30. Our PHO contract requires that number of visits – I have to follow up all DNAs and all those who don’t have a CVD risk measurement and now immunisations and screening.” [Practice employed, number of outreach visits required specified in the service contract ]

17
Service delivery Resource use Reengagement with health services often depends on – Actions of other services – Nurses address of socioeconomic issues Struggle to navigate and secure help Exposes gaps in and problems gaining access to other services Who should fund? Can the health budget sustain use of its resource to address socioeconomic problems?

18
Local service directories Did not exist in some areas Nurses assimilated their own information – Time taken and process used variable – End result was sometimes an informal directory that could not be used by others

19
Other events affecting the services External Environment H1N1 influenza Adverse weather conditions Recession and associated increase in unemployment Capacity issue Preventing travel in some areas Resulting in increased demand to address socioecon problems

20
Feedback on cultural awareness training Content of the three sessions did not : Take into account existing cultural accreditation, knowledge or practice Meet attendees’ expectations Advance existing knowledge or practice Delivery of the 3 sessions was criticized on the basis of: Facilitator skill and experience level Expectation that the course would be delivered by a recognized cultural expert Time involved for practices in relation to outcome from session attendance Delivery style not conducive with group interaction, and perception that it could be effectively delivered by distance learning

21
Lessons for the future IssueFuture considerations Wide variation Who receives outreach Contact rates Service contracts should make explicit: 1. Outreach criteria that details who is eligible and the criteria for a home visit 2. The expected contact rates by type (call/visits/other) per FTE per week Large amount of socioeconomic work The sectors involved should explore possible multi-sectorial models of funding and service delivery Risk of inappropriate referrals 1. The outreach criteria should be made available, and explained, to each referrer 2. Referral acceptance should be subject to : Further investigation using the PMS records and practitioner knowledge to identify and record the fit with the agreed outreach criteria Acceptance by a senior manager who is responsible for the implementation of the service in accordance with the contract specifications.
 per FTE per week Large amount of socioeconomic work The sectors involved should explore possible multi-sectorial models of funding and service delivery Risk of inappropriate referrals 1. The outreach criteria should be made available, and explained, to each referrer 2. Referral acceptance should be subject to : Further investigation using the PMS records and practitioner knowledge to identify and record the fit with the agreed outreach criteria Acceptance by a senior manager who is responsible for the implementation of the service in accordance with the contract specifications..")
22
Lessons for the future IssueFuture considerations Value of nurse involvement and the need for some standards in practice The nursing sector should advise on post graduate education for outreach nurses. At a minimum nurses should receive training on: 1. The outreach role 2. Cost of outreach services 3. Engaging harder to reach audiences 4. Implementation of outreach criteria 5. Working with a defined scope of outreach practice 6. How to investigate and triage outreach referrals 7. Use of the PMS to record activities, code work, and identify and address overdue aspects of care 8. How to approach health issues in the home environment and transition between socioeconomic issues and health problems 9. Effective use of service directories Employment arrangements for outreach nurses PHO employed nurses should be afforded more time to engage practice staff in the outreach work Practice based nurses require protected time to complete outreach activities.

23
Lessons for the future IssueFuture considerations Room to advance outreach cultural awareness training The course should be delivered by an experienced group facilitator who is also a recognized cultural expert. The content should be advanced to: 1. Include more expert advice on the impact of cultural beliefs on health states and perceptions and use of general practice services. 2. Provide education on face to face and telephone engagement of people and teachings about Maori structure and its importance. 3. Invite practices to provide insight into their existing knowledge levels and practice friendliness strategies. 4. Tailor the offering to build on existing problems, strategies, knowledge and practice 5. Ensure course attendees receive expected learning outcomes which highlight how the course will help to build on existing strategies and knowledge.

Similar presentations



 has been commissioned by Ipswich and East Suffolk CCG to establish and run.>")
















