Download presentation
Presentation is loading. Please wait.

2
Capsulotomy CCC K.Nasrolahi MD 1387

3
a) Can – opener capsulotomy: is performed by making a series of small connected tears in a circle to remove the central segment of anterior lens capsule
 Can – opener capsulotomy: is performed by making a series of small connected tears in a circle to remove the central segment of anterior lens capsule")
5
This method permits easy access to and subluxation of the lens nucleus, but it usually result in radial tears in the anterior capsule extending from one or more of the initial puncture sites out to the periphery of the capsule

6
The radial tears can enlarge during hydrodissection or nucleus manipulatin, and they can affect IOL placement and stabilization

7
Placement of both IOL haptics in the bag may be difficult, and unequal postoperative contractile forces within the capsular bag may cause IOL dislocation

9
provides a more stable smooth edge to the anterior capsular opening

10
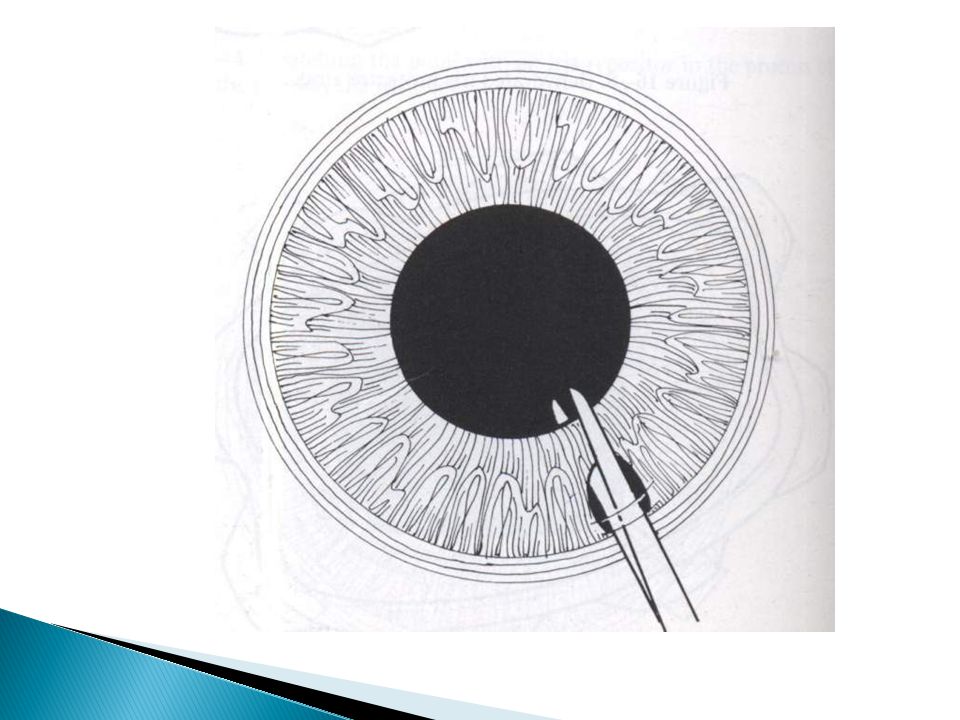
The surgeon begins an anterior capsulorrhexis with a central linear cut in the anterior capsule, using a cystotome needle

12
At the end of the linear cut, the needle is either pushed or pulled in the direction of the desired tear. Allowing the anterior capsule to fold over upon itself

14
The surgeon then engages the free edge of the anterior capsule with either forceps or the capsulotomy needle and the flap is carried around in a circular manner as the surgeon directs the tension toward the center of the lens

16
For maximum control, frequent regrasping of the flap near the tear is helpful

17
Radial extension of the capsulotomy may occur in the setting of forward displacement of the lens with shallowing of the anterior chamber or anterior traction on the capsular flap

18
If the capsulorrhexis tear starts to extend too far peripherally, the flap can sometimes be salvaged and the tear brought more centrally

19
First the surgeon should check for positive vitrous pressure associated with forward displacement of the lens. This may be caused by the capsulotomy instrument, the surgeons fingers, or the lid speculum pressing against the globe It can be corrected.

20
Refilling the anterior chamber with viscoelastic, and inserting a second instrument ( such as an iris spatula ) through the paracentesis to press posteriorly on the lens may help reduce forward displacement of the lens and allow for redirection of the capsular tear.
 through the paracentesis to press posteriorly on the lens may help reduce forward displacement of the lens and allow for redirection of the capsular tear.")
22
1) No tags or flaps anterior capsular remnants interfere with surgery, especially the aspiration of the peripheral cortex
 No tags or flaps anterior capsular remnants interfere with surgery, especially the aspiration of the peripheral cortex")
23
2) The mechanical forces exerted onto the zonules were minimal with this technique.
 The mechanical forces exerted onto the zonules were minimal with this technique.")
24
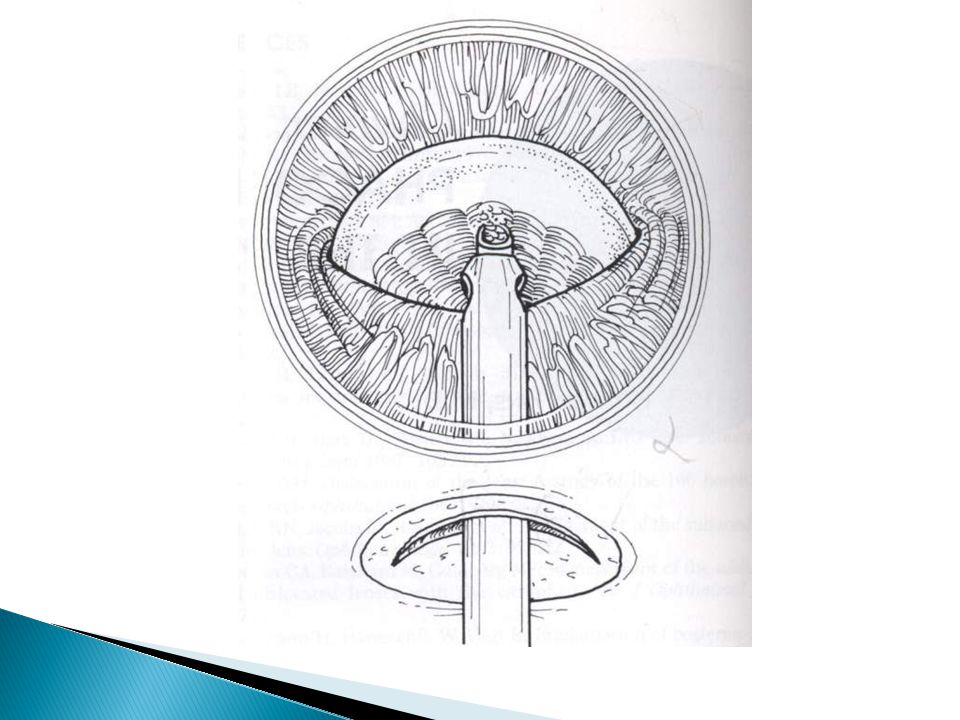
3)The capsular bag is wide open during surgery especially with a closed system approach ;the posterior capsule is ballooned posteriorly.
The capsular bag is wide open during surgery especially with a closed system approach ;the posterior capsule is ballooned posteriorly.")
25
This gives the surgeon ample space to work in far away from the cornea and with greatly reduced risk of catching the posterior capsule as compared with when it is flaccid.

26
4)With an intact capsulorrhexis, manipulations within the capsualr bag such as tilting or cracking the nucleus or implanting an IOL, no longer entail the risk of extending radial teras in the anterior capsulse into the posterior capsule.
With an intact capsulorrhexis, manipulations within the capsualr bag such as tilting or cracking the nucleus or implanting an IOL, no longer entail the risk of extending radial teras in the anterior capsulse into the posterior capsule.")
27
5)Even in the case of a posterior capsule defect, regaedless of its size an intact anterior capsulorrhexis provide the possibility of implanting an IOL safely into the ciliary sulcus
Even in the case of a posterior capsule defect, regaedless of its size an intact anterior capsulorrhexis provide the possibility of implanting an IOL safely into the ciliary sulcus")
30
1) Discontinuity of the anterior capsular rim. 2) Capsulorhexis with too small a diameter. 3) Viscoelastic incarcerations.
 Viscoelastic incarcerations..")
31
To avoid this complication the capsulorhexis should never be completed inside out. Stellate bursts originating from initial puncturing attempts with a blunt needle may desroy an intact capsular margin. In the course of surgery to form a discontinuity. The only effective remedy to repair discontinuity by transformation of the tear in to smooth edge.

32
Discontinuity of the anterior capsular rim

33
- In performing the capsulorhexis, the surgen may realize that the original arc is too small _ The capsulorhexis can be expanded by spiralling outward to the desired diameter and then “closing the circle “

34
_ If the anterior capsular rim adheres to the anterior IOL surface after implantation, viscoelastics residues may trapped behind the lens. _ If it does, mostly the lense blocks the passage for the viscoelastics in to the anterior chamber and at the same time allows the aqueous to invade the area behind the implant.

35
Thus pushing the IOL in to the cornea. _ in such a situation an additional puncture of the peripheral anterior or in narrow pupils – posterior capsule is required to provide for a release of the viscoelastics in to the anterior chamber or the vitreous.

39
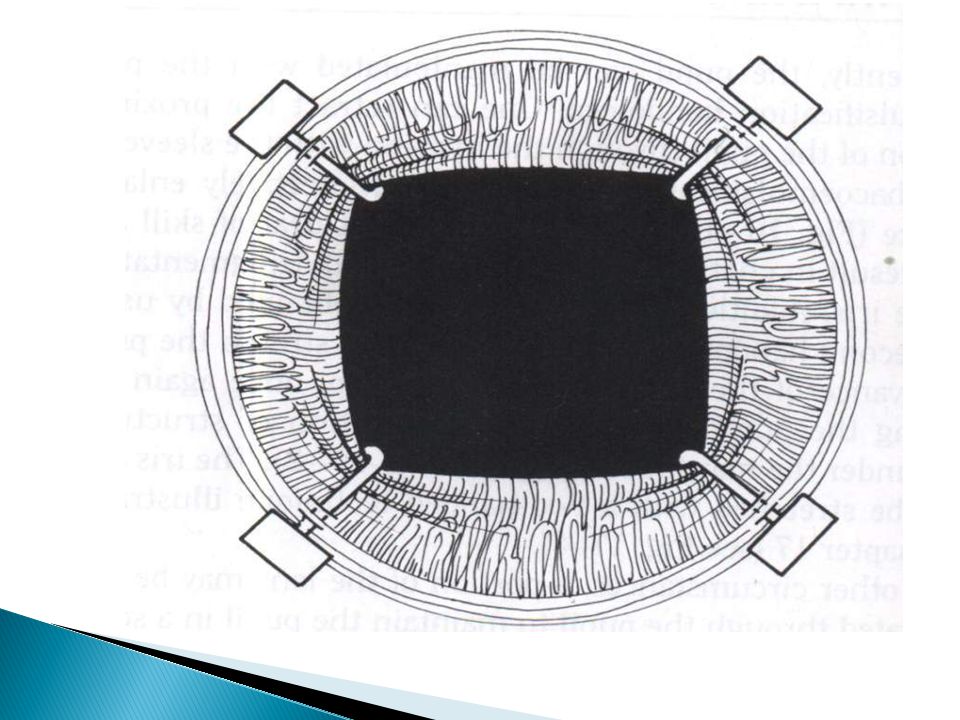
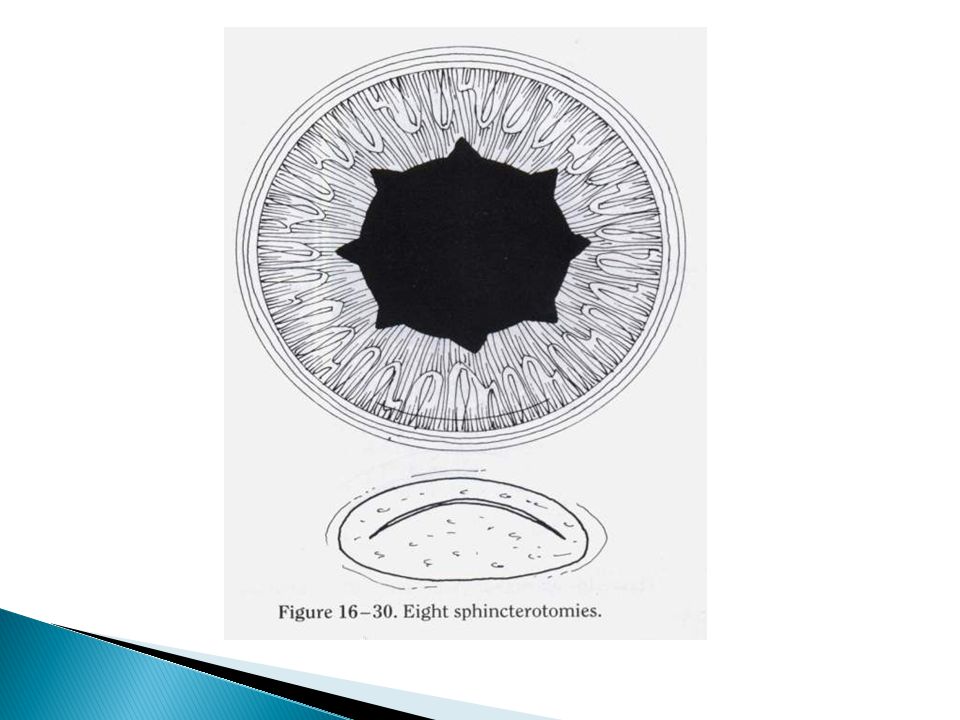
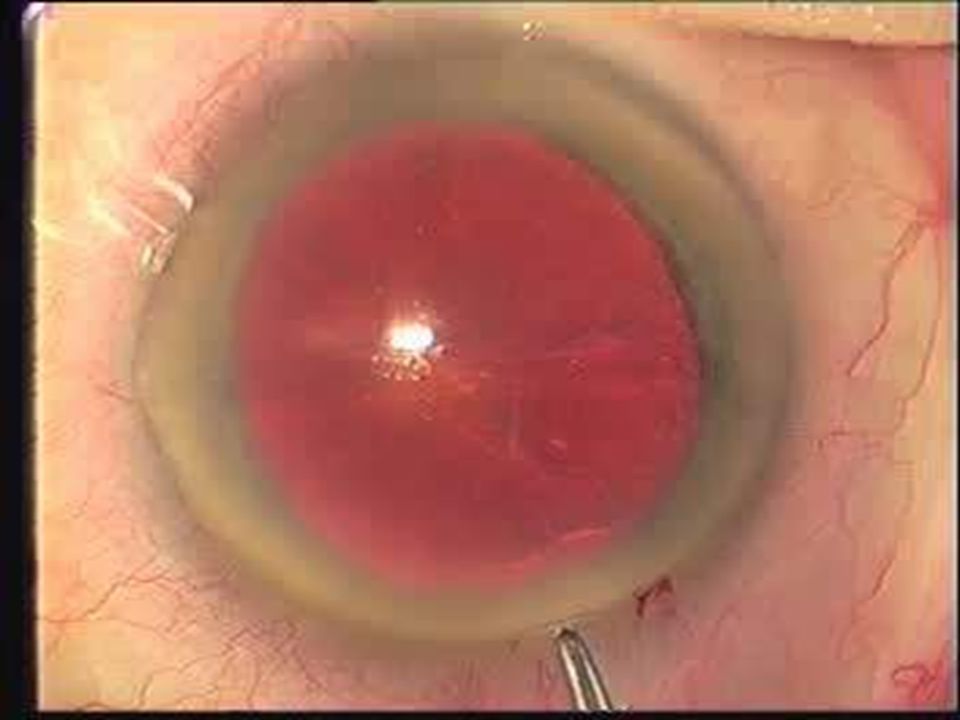
Small pupil: 1) Removal of the pupillary membrane 2) Removal of synechiae 3) Bimanual stretching 4) Iris retractors 5)Pupil dilator
 Removal of the pupillary membrane 2) Removal of synechiae 3) Bimanual stretching 4) Iris retractors 5)Pupil dilator")
52
_ This complication is not known in any other capsulotomy technique and solely relates to the CCC. _ The genuine pathomechanism could not be clarified untile tody. Disadvantages of the CCC : Capsular shrinkage syndrom or capsularphimosis

54
Clinically this problem can be observed especially in patients suffering from pseudoexfoliation syndrome (PEX), uveitis, rtinopathy pigmentosa or subluxation in combination with PMMA or silicone IOL implantation. _ All these diseases have a considerably reduced number of zonula fibers in common.

55
_ This complicltion has not been described in patients suffering from these diseases in context with an acrylic IOL implantation. Allows the conclusion that a certain mechanical intraction of acrylic lenes surface and capsule successfully prevents this problem so that the acrylic IOL is presently the lense of choise in such cases.

56
_ This is not valid for low _ water acrylics. _ A potential remedy to avoid capsular phimosis is the insertion of a capsular tention ring.

64
1) In exfoliation syndrome a basement membrane – like fibrillogranular white material is deposited on the lens, cornea, iris, anterior hyaloid face, ciliary processes, zonular fibers, and trabecular meshwork
 In exfoliation syndrome a basement membrane – like fibrillogranular white material is deposited on the lens, cornea, iris, anterior hyaloid face, ciliary processes, zonular fibers, and trabecular meshwork")
65
2) Associated with this condition are atrophy of the iris at the pupillary margin, deposition of pigment on the anterior surface of the iris, poorly dilating pupil, increased pigmentation of the trabecular meshwork, capsular fragility zonular weakness, and open – angle glaucoma
 Associated with this condition are atrophy of the iris at the pupillary margin, deposition of pigment on the anterior surface of the iris, poorly dilating pupil, increased pigmentation of the trabecular meshwork, capsular fragility zonular weakness, and open – angle glaucoma")
66
3) Patients with exfoliation syndrome may also experience weakness of the zonular fibers and spontanous lens subluxation and phacodonesis
 Patients with exfoliation syndrome may also experience weakness of the zonular fibers and spontanous lens subluxation and phacodonesis")
67
4) Poor zonular integrity may affect cataract surgery technique and IOL implantation
 Poor zonular integrity may affect cataract surgery technique and IOL implantation")
68
5) The exfoliative material may be elaborated even after the crystalline lens is removed Poorly dilating pupil ( small pupil)
 The exfoliative material may be elaborated even after the crystalline lens is removed Poorly dilating pupil ( small pupil)")
Similar presentations
































 Can – opener capsulotomy: is performed by making a series of small connected tears in a circle to remove the central.>")




 Dislocation M.R. Akhlaghi MD.>")







