Download presentation
Presentation is loading. Please wait.

2
It is: A style of talking with people constructively about reducing their health risks and changing their behavior.

3
It is designed to: Enhance the client’s own motivation to change using strategies that are empathic and non-confrontational.

4
It can be defined as: A patient-centered directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence.

5
You can recognize it by observing: The powerful behavioral strategies for helping clients convince themselves that they ought to change The “spirit of MI” style in which it is delivered

6
1. Patient and practitioner are equal partners in relationship (collaborative effort between two experts)
.")
7
People are almost always ambivalent about change – ambivalence is normal Lack of motivation can be viewed as unresolved ambivalence.

8
AMBIVALENCE is the key issue to be resolved for change to occur. People are more likely to change when they hear their own discussion of their ambivalence. This discussion is called “change talk” in MI. Getting patients to engage in “change talk” is a critical element of the MI process. *Glovsky and Rose, 2008

10
The person agrees with us Is willing to comply with our recommendations and treatment prescriptions States desire for help Shows distress, acknowledges helplessness Has a successful outcome

11
The probability that a person will enter into, continue, and comply with change-directed behavior

13
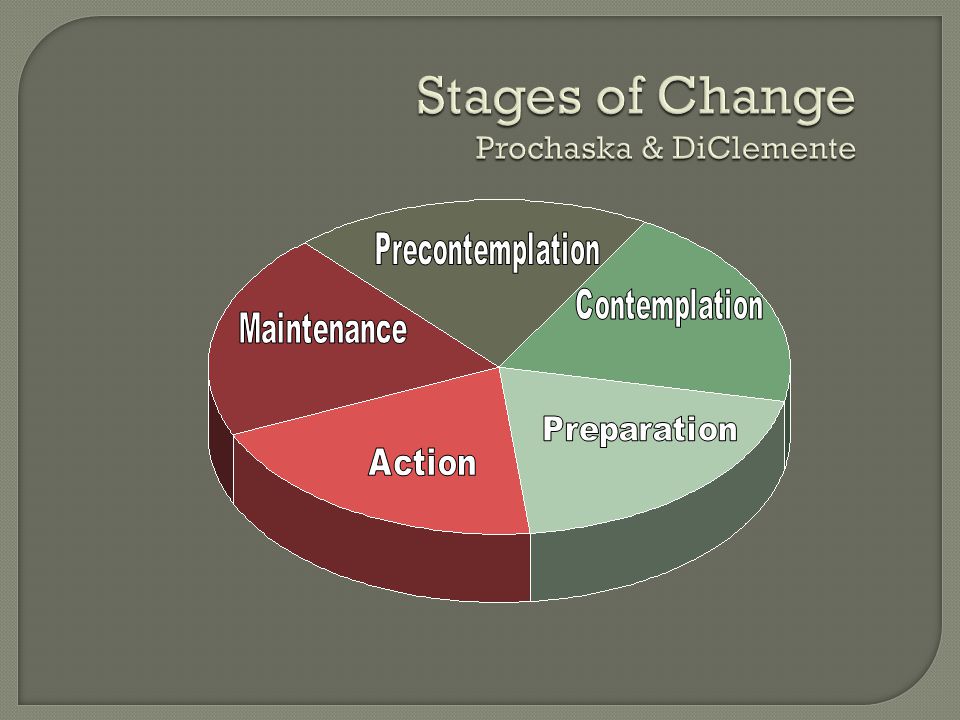
40% in precontemplation 40% in contemplation 20% in preparation or action *Prochaska and DiClemente, 1998

14
Precontemplation Stage Definition Not yet considering change or is unwilling or unable to change Primary task Raising Awareness

15
Offer factual information Explore the meaning of events that brought the person in and the results of previous efforts Explore pros and cons of targeted behaviors

16
In this stage the client sees the possibility of change but is ambivalent and uncertain about beginning the process Primary task Resolving ambivalence and helping the client choose to make the change

17
Talk about the person’s sense of self- efficacy and expectations regarding what the change will entail Summarize self-motivational statements Continue exploration of pros and cons

18
In this stage the client is committed to changing but is still considering exactly what to do and how to do Primary task Help client identify appropriate change strategies

19
Offer a menu of options for change or treatment Help client identify pros and cons of various treatment or change options Identify and lower barriers to change Help person enlist social support Encourage person to publicly announce plans to change

20
In this stage the client is taking steps toward change but hasn’t stabilized in the process Primary task Help implement the change strategies and learn to limit or eliminate potential relapses

21
Support a realistic view of change through small steps Help person identify high-risk situations and develop appropriate coping strategies Assist person in finding new reinforcers of positive change Help access family and social support

22
Maintenance Stage Definition A stage in which the client has achieved the goals and is working to maintain them Primary task Client needs to develop new skills for maintaining recovery

23
Help client identify and try alternative behaviors (drug-free sources of pleasure) Maintain supportive contact Encourage person to develop escape plan Work to set new short and long term goals
 Maintain supportive contact Encourage person to develop escape plan Work to set new short and long term goals")
24
Use the microskills Open-ended questions Affirmations Reflections Summaries to elicit and reinforce self-motivational statements (Change Talk)
")
25
Open-ended questioning Affirming Reflective listening Summarizing Building Motivation using OARS (the microskills)
")
26
Listen to both what the person says and to what the person means Check out assumptions Create an environment of empathy (nonjudgmental) You do not have to agree Be aware of intonation (statement, not question)
 You do not have to agree Be aware of intonation (statement, not question)")
27
1. Expressing empathy 2.Developing discrepancy 3.Avoiding argumentation 4.Supporting self-efficacy

28
Acceptance facilitates change Skillful reflective listening is fundamental Ambivalence is normal

29
Discrepancy between present behaviors and important goals or values motivates change Awareness of consequences is important Goal is to have the PERSON present reasons for change

30
The good things about ______ The not- so-good things about ____ The good things about changing The not-so- good things about changing Decisional Balance

31
Resistance is signal to change strategies Labeling is unnecessary Shift perceptions Peoples’ attitudes shaped by their words, not yours

32
Belief that change is possible is important motivator Person is responsible for choosing and carrying out actions to change There is hope in the range of alternative approaches available

33
Patients are often demoralized and unwilling to consider alcohol and drug abstinence (or manage their dual disorders ) due to: Severe and disabling symptoms Frequent failed treatment episodes Poor functional adjustments
 due to: Severe and disabling symptoms Frequent failed treatment episodes Poor functional adjustments")
34
Staying Clean and Sober Taking Medications Participating in Dual Diagnosis Specialty Program

35
Less resistance Fewer questions about the problems More questions about change Self-motivational statements Resolve Looking ahead Experimenting with change

Similar presentations














. 4-2 How Does Behavior Change? Behavior ABehavior B.>")

 Presentation Objectives Understand theory & spirit of MI Brief review of evidence using MI with teens Learn some MI techniques.>")




