Download presentation
Presentation is loading. Please wait.

1
welcome

2
Patient itch/ Itchy Rash

3
Prof. DOULAT RAI BAJAJ FCPS, MCPS Professor & Chairman Dept
Prof. DOULAT RAI BAJAJ FCPS, MCPS Professor & Chairman Dept. of Dermatology LUMHS

4
Goals of Presentation At the end of presentation you would be able to:
Clinically evaluate a patient with itch or itchy rash Make a working diagnosis Manage it at the best

5
How to Evaluate? History Examination Lab investigations

6
History: Age of patient
Infant/child: Atopic Dermatitis Scabies, Pediculosis Infantile seb. dermatitis psoriasis Mastocytosis Insect bites (papular urticaria) Urticaria
 Urticaria.")
7
Age of patient: Young adult
Specific dermatoses: Atopic Dermatitis, Contact Dermatitis, Psoriasis, P. Rosea, lichen simplex chronicus, Prurigo, Infections: Scabies, body lice, Yeast & fungal infections (tineas, P. versicolor)…. Hypersensitivity reactions: urticaria, Dermatitis herpetiformis Miscellaneous: cut. Lymphoma, psychogenic……
…. Hypersensitivity reactions: urticaria, Dermatitis herpetiformis. Miscellaneous: cut. Lymphoma, psychogenic……")
8
History: Old age: Xerosis psoriasis Aging of skin Drug reactions,
Dermatitis Herpetiformis Xerosis psoriasis Aging of skin Drug reactions, Systemic diseases

9
History: Acute vs Chronic
Acute: scabies, pediculosis, drugs, insect bites, urticaria Chronic: AD, ACD, Psoriasis, LSC, prurigo, systemic diseases Gender: pregnancy associated dermatoses Family history: Scabies, pediculosis, psoriasis, AD,

10
History: Presence of Systemic Disease: Renal: CRF, Pt on dialysis
Endocrine: DM, hypo-and hyperthyroidism, Liver Disease Malignancies: any internal malignancy AIDS: Hematological: Polycythmia, anaemia Psychogenic

11
Examination: Type of lesion: macule/patch, papule/plaque, nodule, vesicle/bullae, pustule, erosion/ulcer .. Sites and Distribution: Shape: annular, discoid, polygonal, arcuate… Pattern: discrete, grouped, linear, segmental, dermatomal Colour, consistency, margins etc Secondary features: crust, scale, excoriation,

12
Investigations: Woods’ light examination
Scrappings for fungal infections Skin Biopsy:

13
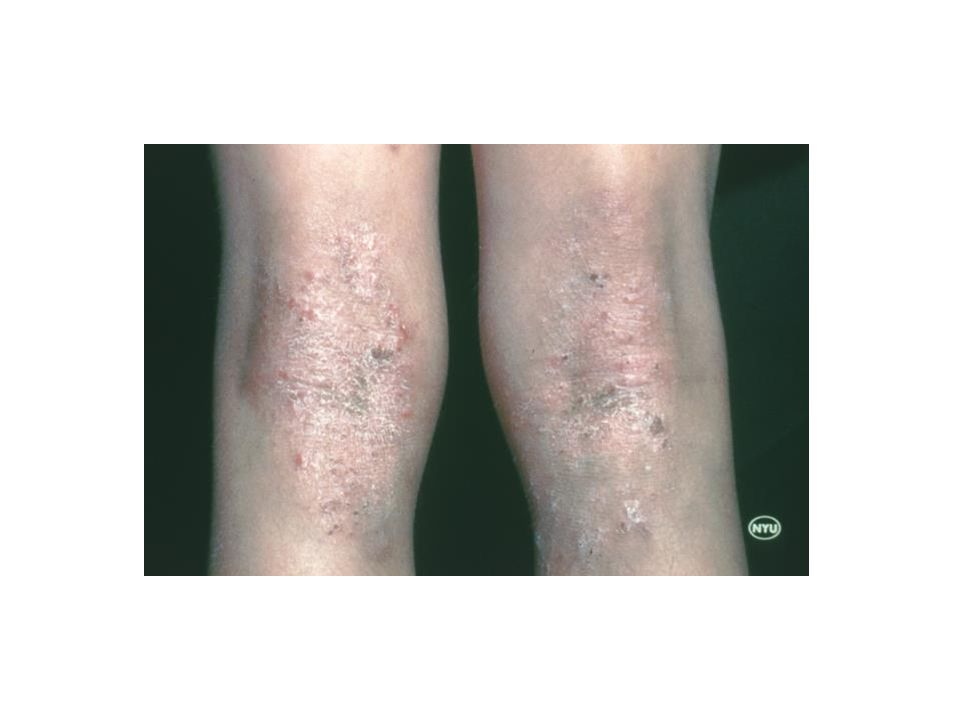
Atopic Dermatitis

14
ATOPIC DERMATITIS Clinically manifested by: ASTHMA
“ATOPY” is a genetically determined tendency to produce increased amounts of reagens (IgE), in response to allergens. Clinically manifested by: ASTHMA HAY FEVER ATOPIC DERMATITIS
, in response to allergens. Clinically manifested by: ASTHMA. HAY FEVER ATOPIC DERMATITIS.")
16
IMMUNITY Antigen T cell IL-1 IL-4 B cell IgG IgM IgA IgD IgE Plasma
Macrophage IMMUNITY T cell IL-1 IL-4 B cell IgG IgM IgA IgD IgE Plasma cell

17
ALLERGY Macrophage Antigen T cell IL-1 IL-4 B cell Plasma cell IgE

18
Major features (must have 4)
Pruritus Early age of onset Typical morphology and distribution Infants & Children: Face & extensors Adults: Flexureal lichenification & linearity Chronic course Personal or family history of atopy (asthma, rhino-conjuctivitis, dermatitis).
.")
19
Minor features Dryness of skin
Ichthyosis , palmar hyperlinearity/keratosis pilaris Hand/foot dermatitis Lip dermatitis Nipple eczema Increased cutaneous infections e.g. Staph. aureus & H.Simplex)
")
20
Common Clinical Features:
Itching Erythematous Macules, Papules, vesicles Eczema with crusting, Lichenification, Excoriation Dry skin Secondary infection

21
ACUTE vs Chronic AD Acute AD Chronic AD Redness Swelling Papules
Vesicles Exudation Cracking Less vesiculation/ exudation More Thickening, pigmentation & Lichenification (due to rubbing & scratching) Fissures Scratch marks
 Fissures. Scratch marks.")
23
Infantile/childhood AD Adult AD
Red Itchy scaly lesions on scalp, cheeks, wrists & trunk Diaper area spared Extensor aspects of limbs (begins to Crawl) Irritable & restlessness Crusts Pustules Lichenified, pigmented papules, plaques scattered all over body Bothering itch Prominent infra-orbital crease General dry skin
 Irritable & restlessness. Crusts. Pustules. Lichenified, pigmented papules, plaques scattered all over body. Bothering itch. Prominent infra-orbital crease. General dry skin.")
28
Sebhorroic Dermatitis

29
Seb. Derm Characterized by: Erythematous scaly plaques Greasy scaling
yellow crusted patches & plaques There is very minimal itch (vs AD) Age of onset: Below 06 months: infantile SD After puberty: adult SD
 Age of onset: Below 06 months: infantile SD. After puberty: adult SD.")
30
Sites: Infantile SD: Adult SD: Scalp (Cradle Cap),
Face & Neck (eye brows, Ears & sides of neck). Trunk & Flexures, starting in napkin area. Adult SD: Scalp Forehead Face: Eyebrows, Nasolabial folds, ear canals, behind pinnae, Trunk: sternal area, interscapular region & flexures
. Trunk & Flexures, starting in napkin area. Adult SD: Scalp. Forehead. Face: Eyebrows, Nasolabial folds, ear canals, behind pinnae, Trunk: sternal area, interscapular region & flexures.")
34
Irritant Contact Dermatitis Allergic Contact Dermatitis

35
Irritant Contact Dermatitis
Non-allergic reaction of the skin caused by exposure to irritating substance Any person can develop ICD if concentration & duration of contact sufficient About 80% of occupational dermatitis is irritant in nature C/F: Erythema, Edema, Vesiculation, Weeping

36
ALLERGIC CONTACT DERMATITIS
Immunologically-mediated, Delayed (type IV) hypersensitivity Occurs in persons already sensitized Not dose related, Not restricted to area of contact C/F: erythema, edema, papules, papulovesicles it is difficult to distinguish C/F of ACD from irritant or constitutional dermatoses(AD, SD)
 hypersensitivity. Occurs in persons already sensitized. Not dose related, Not restricted to area of contact. C/F: erythema, edema, papules, papulovesicles. it is difficult to distinguish C/F of ACD from irritant or constitutional dermatoses(AD, SD)")
37
Common sensitizer: Hair dyes Nickel, Chromate, cobalt Leather, Rubber Topical Drugs: neomycin, gentamicin, lignocaine Plants

38
Pathogenesis ACD

40
Dry scaly dermatitis

41
ACD due to items in pocket

46
LEATHER

47
ADHESIVE TAPE

48
PLANTS

49
Tatoos causing ACD

50
TREATMENT

51
Treatment Principles Avoid known triggers
Moisturize, moisturize, moisturize Itch Control Topical corticosteroids Other topical therapies Systemic therapy

53
Avoid Irritants Allergen avoidance during pregnancy and or infancy (mild benefit shown from avoiding cow’s milk, eggs, and dust mites) Big Five: dryness, dust mites, animal dander, cigarette smoke, wool Others include water and chemicals

54
Dry Skin Care Baths and showers not hot and short
Mild soap (Dove) – best to avoid alkali soaps Blot dry and immediately moisturize (skin should still be slightly damp) Creams and ointments better than lotions and oils
 – best to avoid alkali soaps. Blot dry and immediately moisturize (skin should still be slightly damp) Creams and ointments better than lotions and oils.")
55
Itch Control Avoid topical antihistamines
Products containing menthol, camphor & weak conc: of phenol may be helpful Cool compresses Avoid hot/sweaty conditions

56
Antihistamines In children generally sedating AH used. No role of non-sedating AH in children with AD A combination of sedating & non-sedating AH indicated in adults with eczema. For AD: Zonalon=topical doxepin – qid for maximum of eight days. Never occlude, some systemic absorption, very sedating, risk of ACD

57
TOPICAL STEROIDS Steroid Potency Vehicle Amount Site
Clinical stage of eczema Weather Duration of treatment Disease

58
Super Potent Potent Mild Moderate Potent
Clobetasol propionate 0.05% (dermovate) Diflucortolone valerate (volog) Flucinolone acetonide 0.2% Halcinonide Fluticasone propionate (cutivate) Amcinonide Mometasone Furoate (hivate) Betamethasone dipropionate (diprolene) Betamethasone valerate 0.1% (betnovate) Triamcinolone acetonide (kenacomb) Desonide (desone) Methylprednisolone aceponate 0.1% (advantan) Betamethasonvalerate 0.025% Prednicarbate Hydrocortisone Methyl prednisolone acetate 0.25% Flucinolone acetonide %
 Diflucortolone valerate (volog) Flucinolone acetonide 0.2% Halcinonide. Fluticasone propionate (cutivate) Amcinonide. Mometasone Furoate (hivate) Betamethasone dipropionate (diprolene) Betamethasone valerate 0.1% (betnovate) Triamcinolone acetonide (kenacomb) Desonide (desone) Methylprednisolone aceponate 0.1% (advantan) Betamethasonvalerate 0.025% Prednicarbate. Hydrocortisone. Methyl prednisolone acetate 0.25% Flucinolone acetonide %")
59
Other Topical Therapies
Tar Salicylic acid Topical Tacrolimus, pimecrolimus

60
Antimicrobials Antibiotics for culture proven infections
Ketoconazole for head and neck based atopic dermatitis (reduce yeast counts)
")
61
Phototherapy UVB Narrow Band UVB UVA/PUVA Sunlight

62
Other Therapies Leukotriene Inhibitors do not work
Oral cromolyn sodium results conflicting Interferon gamma daily s/c inj. helps Cyclosporine Azathioprine Hydroxychloroquine

63
Some Specific Types of Eczema

64
Discoid/Nummular eczema
Circular or oval plaques A clearly demarcated edge Related to atopy, emotional stress, bacterial infection Usually lesions dry. Exudative ones always associated with bacterial infections. Treatment: Emollients, topical steroids, antibacterials

67
Lichen Simplex Chronicus
An eczematous dermatosis characterized by Lichenified plaques, usually 1-2 in number Typical sites: nape of neck, scrotum, wrists skin thickened, pigmented with prominent skin markings Associated with atopy, emotional stress Tr: Superpotent steroids with keratolytic agents. I/L steroid injections

68
LSC

70
Nodular Prurigo Characterized clinically by chronic, intensely itchy papules & nodules lesions range from small papules to hard nodules, 1–3 cm in diameter, with a raised, warty surface. The early lesion is red later becoming pigmented. Tr: superpotent steroids, oral steroids, UVB, PUVA, thalidomide

72
Pompholyx Pompholyx is characterized by the
sudden onset of clear vesicles over hands. Symptoms: No erythema, less pruritus but more heat and prickling sensation. Sites: sides and dorsa of fingers & hands Vesicles may become confluent and present as large bullae, especially on feet. Itching may be severe, preceding the eruption of vesicles

75
Pityriasis Rosea (P. rosea)
An acute, self-limiting disease, probably infective in origin, affecting mainly children and young adults. The first lesion is “Herald patch” a large circular, sharply defined eryhematous patch with fine scales on thigh/trunk. This is followed by an eruption of discrete oval lesions, dull pink in colour, covered by fine, dry, silvery scales forming a collarette at edges. The centre tends to clear and assumes a wrinkled, atrophic appearance. The lesions appear in crops.

76
P.Rosea contd……. The lesions tend occur in ‘chrismas tree’ pattern along the rib cage. There are usually no symptoms. Some pts. have mild to moderate pruritus Tr: The common asymptomatic, self-limiting cases require no treatment. If itch is severe or the appearance distressing, a topical steroid (moderate potent) or UVB can be helpful.
 or UVB can be helpful.")
80
Asteototic Eczema Eczema developing in dry skin
Seen on legs, arms and hands. Tends to be more marked in the winter and in elderly people. Skin is dry, scaly showing a criss-cross skin markings. Finger pulps are dry and cracked; retaining a prolonged depression after pressure (‘parchment pulps’). Associated with hypothyroidism, zinc deficiency, diuretic use and cimetidine use
. Associated with hypothyroidism, zinc deficiency, diuretic use and cimetidine use.")
83
Pityriasis alba D/D: vitiligo, P. versicolor, PIH
A mild eczema in which hypopigmentation is the most conspicuous feature. (NO CALCIUM Deficiency Predominantly seen in children b/w ages of ys. The individual lesion is circular, oval or irregular hypopigmented patch with NOT well defined edges. Lesions often slightly erythematous & have fine scale Common sites: cheeks & around the mouth & chin Less commonly on neck, arms, shoulders & trunk. D/D: vitiligo, P. versicolor, PIH Tr: mild steroids, emollients

86
SUMMARY

87
Disease Typical morphology Diagnostic clues Irritant CD Allergic CD Atopic Dermatitis Sebhorroic dermatitis Xerotic/asteotic eczema Nummular /discoid eczema Pompholyx Sharply demarcated macular erythema, little vesiculation Exzematous, scaly edematous plaques with vesiculation Eczematous, honey-crusted scaly plaques, lichenified in chronic cases Greasy scaly papules, minimal itch Crackled parchment like patches, no edema, no vesiculation Coin-shaped, well demarcated, scaly or weepy plaques, bilateral, symetrical, kissing lesions Deep seated papulo-vesicles on palmar plantar surfaces, volar edges More burning less itch, only at area of contact Pruritis, primary lesion at area of contact , Flexural areas, neck predominance Hair bearing areas, glabella, nasolabial folds Lower legs Arms, legs, dorsal hands Palms, soles, typical dorsal involvement

88
Conclusions Eczema management rests on three pillars: avoid irritants, moisturize, topical management Use steroids to quiet a flare then switch to a nonsteroidal therapy Treating hot spots can prolong remissions Control itch!

89
This presentation is available on www.lumhs.edu.pk/DFHC/html
THANK YOU This presentation is available on DFHC

Similar presentations





































>")



 -Dyshidrotic.>")




