Download presentation
Presentation is loading. Please wait.

1
Lupus Nephritis

2
Background GM (G036181) 51 year old Caucasian female Presented with nephrotic syndrome and hypertension in 2000
 51 year old Caucasian female Presented with nephrotic syndrome and hypertension in 2000")
3
Presented in 2000 Urine protein +++, 24 hour protein 7 gms Albumin 26, creatinine 90 Creatinine clearance 95 ml/min ANA, anti DNA, ANCA –ve, Complement normal Myeloma screen negative

4
Renal Biopsy 15 glomeruli Evidence of membranous nephritis 2 sclerosed gloms, 3/15 crescents Immuno-IgG, C3 positive, IgA, IgM negative ? Membranous lupus No other features of lupus clinically

5
Course in 2000 Started on 30 mg pred, 100 mg azathioprine ACE added in, changed to ARB due to dry cough Diarrhoea on aza, stopped after a month, resolved on stopping aza. Pred tapered over the next 2 months 24 hr protein 5.7 gms, albumin 27

6
Over the next 6 years… Ongoing proteinuria Stable creatinine- 90 micromol/l Ca breast in 2005 treated with lumpectomy and radiotherapy

7
June 2006 Admitted generally unwell Worsening renal function Creatinine 210 and climbing ANA strongly positive, anti DNA –ve, complement normal, anti smith not tested 24 hr urine protein 5.4 gms Started on modified Ponticelli regime Cycloposphamide 100 mg/day, pred 40 mg Soon reduced to cyclo 50mg and pred 20 mg due to side effects

8
Over the next few weeks…. Creatinine improved from 267 to 200 and stable Abnormal LFTs thought to be due to statins, improved after stopping statins Generalised weakness, stops cyclo in september Desperate to cut down steroids, reduced and stopped over the next few weeks Creatinine stable-200

9
Admission October 2006 Admitted on 25 th oct for repeat biopsy ? Transformation to proliferative lupus nephritis Worsening renal function- creat 328 No change in serum immunology Post biopsy bleed, resolved without intervention

10
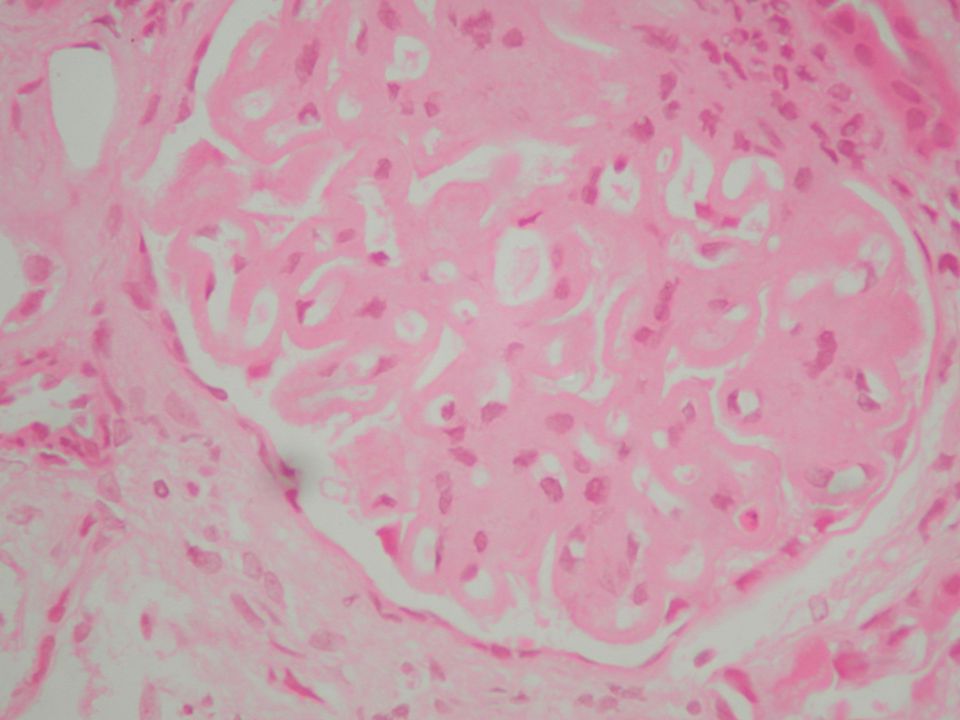
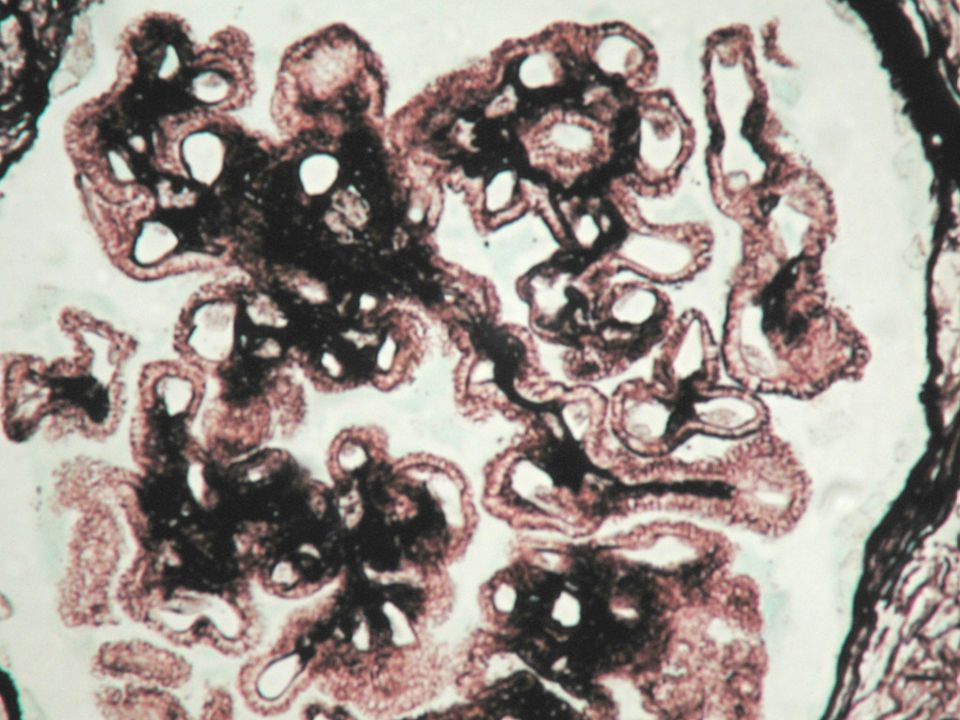
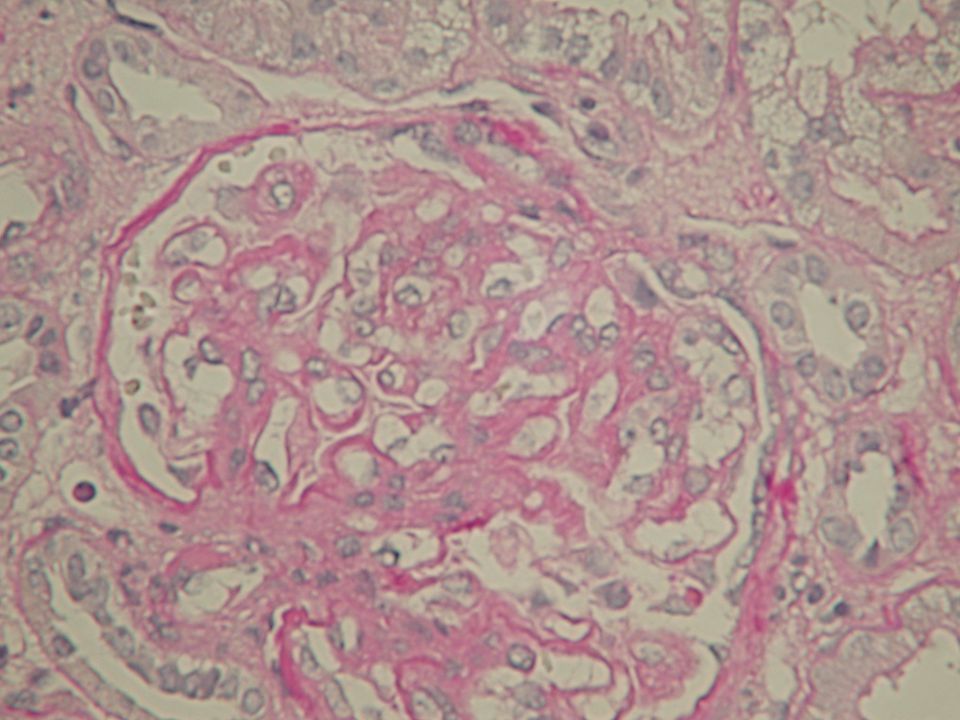
Renal biopsy October 2006 20 gloms-6 sclerosed Membranous GN and some proliferative changes. No necrotising lesions, no crescents Mild to moderate background damage Full house immunology –IgG+++,IgA+, IgM++, C3++, C1q++ EM- Numerous electron dense deposits with many subepithelial deposits Class 5 + 4 lupus nephritis

16
Treatment Refused IV cycloposphamide Treated with MMF and methyl prednisolone Creatinine peaked at 370 Improved to 200 after 2 weeks

17
Lupus nephritis Renal involvement common in idiopathic SLE Abnormal urinalysis common finding – with or without renal impairment Proteinuria most frequently observed abnormality (80%) – (Rothfield- 1981) plasma creat 30% pts – evidence of decreased renal functions uncommon in first few years of diagnosis
 – (Rothfield- 1981) plasma creat 30% pts – evidence of decreased renal functions uncommon in first few years of diagnosis")
18
Diagnosis Clinical manifestations Immunological tests Renal biopsy

19
Immune complex disease Class I: normal glomeruli (~8% of biopsies) Class II: pure mesangial alterations (~40% of biopsies) Class III: focal glomerulonephritis (~15% of biopsies) a.Class IIIA: focal segmental glomerulonephritis (~12% of biopsies) b.Class IIIB: focal proliferative glomerulonephritis Class IV: diffuse glomerulonephritis (~25% of biopsies) Class V: diffuse membranous glomerulonephritis (~8% of biopsies) Class VI: advanced sclerosing glomerulonephritis
 Class II: pure mesangial alterations (~40% of biopsies) Class III: focal glomerulonephritis (~15% of biopsies) a.Class IIIA: focal segmental glomerulonephritis (~12% of biopsies) b.Class IIIB: focal proliferative glomerulonephritis Class IV: diffuse glomerulonephritis (~25% of biopsies) Class V: diffuse membranous glomerulonephritis (~8% of biopsies) Class VI: advanced sclerosing glomerulonephritis")
20
Immune complex disease Distinct histologic, clinical and prognostic characteristics Substantial overlap – 15 to 50% evolve from one form to another – suggested in several studies One pathological finding relatively specific to lupus is presence of tubuloreticular structures in glomerular endothelial cells

21
Immunological tests Pts. with SLE synthesize a variety of different autoantibodies – many react to well characterized nuclear antigens Some antibodies also found in other CTD 3 antinuclear antibodies diagnostically useful – anti-DNA; anti-Sm; and anti-RNP

23
Treatment of lupus nephritis Optimal treatment varies with type of disease Mesangial disease – good renal prognosis – requires no treatment unless progression to more severe glomerular involvement Focal proliferative disease – IIIa prognosis good-no treatment;IIIb-treated like DPLN

24
Membranous lupus Renal prognosis variable – (appel- 1987;Donadio-1977;Sloan-1996) Natural history uncertain Clinical features associated with poor outcome- plasma creat. at presentation,heavy proteinuria –(Sloan-1996)
.")
25
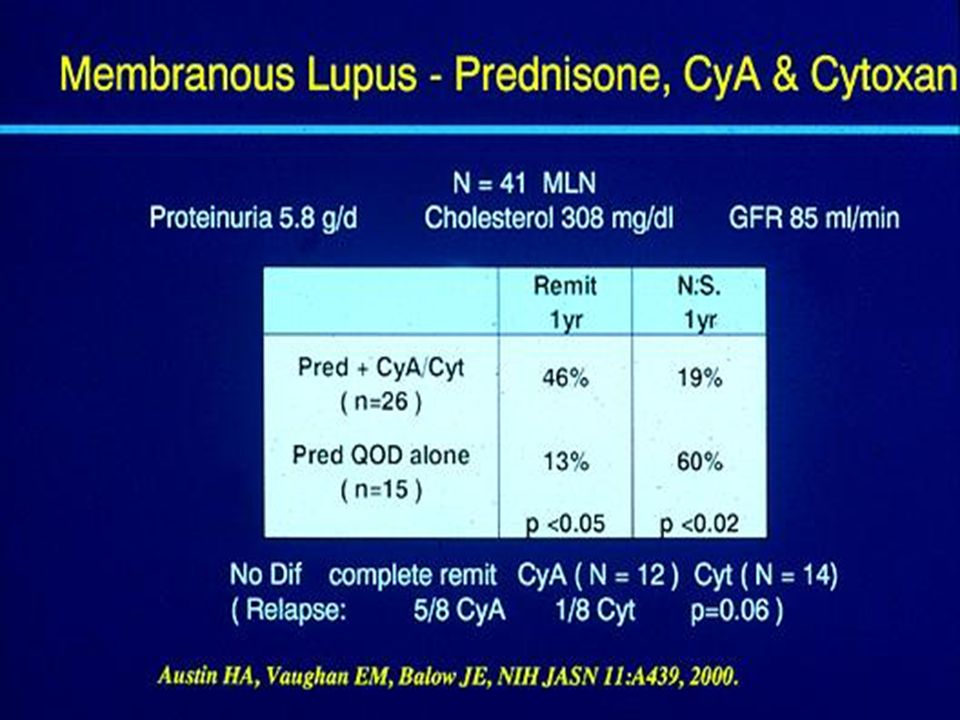
Membranous lupus Optimal therapy uncertain Asymptomatic patients often not treated;those with moderate disease may be treated with prednisolone Those with worsening renal functions or marked NS treated with same regimen as DPLN NIH study comparing cyclophosphamide or cyclosporin to prednisolone

27
Membranous lupus Combination therapy with steroids and chlorambucil may be beneficial Retrospective study by Ponticelli group – 8 pts in the methypred and 11 pts in methylpred/chlorambucil 7 of 8 pts in steroid alone group had flares and 3 had complete or partial remission after 114 months mean f/u 1 of 11 in comination therapy group had flare and 10 had complete or partial remission after 83 mos mean f/u

28
Diffuse proliferative disease Aggressive therapy indicated – (appel-1987;Austin- 2000) Despite aggressive treatment,some pts. will progress to renal insufficiency Severity of tubulointerstitial disease and crescent formation also correlate with long term prognosis- (Austin-1994)
.")
29
Treatments available Steroids – oral prednisolone/IV methylprednisolone Cyclophosphamide – IV/oral Azathioprine Cyclosporin MMF Anti-CD20 monoclonal antibody

30
Boumpas DT et al,Lancet.1992

36
NIH study – Conteras et al 59 pts (12 in class III,46 in class IV,1 in class Vb) – seven monthly boluses of iv cyclophosphamide(0.5 to 1.0g/m 2 BSA) plus steroids Randomly assigned to 1 of 3 maintanance therapies – quarterly iv cyclo/oral Aza(1 to 3 mg/kg/d)/oral MMF(500 to 3000mg/d) for 1 to 3 years
 – seven monthly boluses of iv cyclophosphamide(0.5 to 1.0g/m 2 BSA) plus steroids Randomly assigned to 1 of 3 maintanance therapies – quarterly iv cyclo/oral Aza(1 to 3 mg/kg/d)/oral MMF(500 to 3000mg/d) for 1 to 3 years")
37
NIH study During maintanance – 5 pts died(4 in cyclo group/1 in MMF),CRF in 5(3 in cyclo/1 each in Aza and MMF) 72 month event free survival rate for composite end point of death or CRF higher for MMF and Aza groups Rate of relapse free survival higher in MMF group Incidence of hospitalization, amenorrhoea, infections was significantly lower in MMF and Aza groups
,CRF in 5(3 in cyclo/1 each in Aza and MMF) 72 month event free survival rate for composite end point of death or CRF higher for MMF and Aza groups Rate of relapse free survival higher in MMF group Incidence of hospitalization, amenorrhoea, infections was significantly lower in MMF and Aza groups")
38
More evidence for MMF Hong Kong group – JASN,Feb 2005 Extended long-term study, with median f/u of 63 mos Role of MMF as continuous induction- maintenance tretment for DPLN 33 pts. in MMF arm and 31 pts. In cyclo/Aza arm both in combination with prednisolone

39
More evidence for MMF Complete or partial remission in 90% in each group Improvement in serology and proteinuria comparable between both groups Relapse- free survival and hazard ratio for relapse similar Fewer infections with MMF 4 pts in cyclo/Aza as compared to 1in MMF reached composite end point of death or CRF

40
Anti-CD20 monoclonal antibody(Rituximab) B cell depletion using monoclonal antibody Prolonged remissions achieved in lupus pts. Case reports in lupus nephritis RCTs needed

41
Conclusions 1 Renal involvement common in lupus Diagnosis of lupus nephritis based on a combination of renal bx and immunological tests Anti-ds DNA most useful test for diagnosis and monitoring of disease activity

42
Conclusions 2 Immunosuppressive treatment for class IIIb,IV and some cases of V DPLN poorest prognosis Cyclophosphamide and steroid based regimens traditionally Very good latest evidence for MMF with less side-effect profile Rituximab seems promising

43
Thank you Questions?

Similar presentations








>")














 Characteristics : Proteinuria ( urine protein loss > 2 gm/day ) Hypo-proteinemia ( serum albumin < 2.5 gm/dL ) Edema Hyperlipidemia.>")



