Download presentation
Presentation is loading. Please wait.

1
Acute Respiratory Diseases in the Tropics: diagnosis and treatment protocols for resource poor areas of sub-Saharan Africa Taste of Tropical Medicine Bill Stauffer University of Minnesota Departments of Medicine and Pediatrics, Infectious Diseases

2
Introduction Acute respiratory illness is the leading cause of mortality of children worldwide. Resources will vary, these protocols will be most useful in resource limited settings and must be adapted to each new clinical setting depending on: Disease epidemiology (i.e. malaria endemic) Diagnostics available Medications available
 Diagnostics available. Medications available.")
3
Unwell child or infant older than 2 months
Exclude malaria Take a full history and perform an examination using unwell child and infant history and examination form What is the child’s main complaint/symptom? Difficulty in breathing and cough Diarrhoea Fever (not malaria) Irritability, neck stiffness or bulging fontanelle Acute Respiratory Distress Protocol Gastroenteritis Treatment Protocol Septic Child Protocol Meningitis Treatment Protocol
 Irritability, neck stiffness or bulging fontanelle. Acute Respiratory Distress. Protocol. Gastroenteritis Treatment Protocol. Septic Child Protocol. Meningitis Treatment Protocol.")
4
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardia and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
5
Pneumonia Protocol: Infants and Children > 2 months
Does the infant have indrawing of the chest wall? Yes No Does the infant have any of the following? Central cyanosis off oxygen Severe respiratory distress Inability to drink Yes No Very Severe Pneumonia Severe Pneumonia Pneumonia Ceftriaxone Ampicillin plus Chloramphenicol Amoxicillin or Ampicillin Worsens or fails to respond in hours

6
Pneumonia Protocol: Infants and Children > 2 months
Very Severe Pneumonia Severe Pneumonia Pneumonia Ceftriaxone ( mg/kg IV divided Bid (may give IM if no IV access) Give ampicillin (100 mg/kg IV/IM every 6 hours) and chloramphenical (50 mg/kg every 8 hours) for at least 48 hours Give oral amoxicillin (or IV ampicillin) Give the first dose in the clinic The child MUST be discussed with a doctor and reviewed as soon as possible *IV flush 10-20 mls/kg of NS Child should be checked by a nurse every 6 hours and by a doctor or medic every day **Maintenance fluid (D5NS) Obtain a chest x-ray Weight Fluid ml/hour 2kg 8 4kg 16 6kg 25 8kg 33 10kg 42 12kg 46 14kg 50 16kg 54 18kg 58 20kg 63 22kg 65 24kg 67 26kg 69 Monitor and ensure oxygen saturations >90% Ensure that the child is receiving adequate fluid Encourage breastfeeding and oral fluids If child cannot drink: For Severe Pneumonia: pass a nasogastric tube and give maintenance fluid in one hourly amounts, or, For Very Severe Pneumonia give IV flush* if dehydrated and start on D5NS maintenance, the doctor and all medics on duty must be aware of this child, especially overnight Give paracetamol (15mg/kg as needed up to 4 times a day) for fever
 Give ampicillin (100 mg/kg IV/IM every 6 hours) and chloramphenical (50 mg/kg every 8 hours) for at least 48 hours. Give oral amoxicillin (or IV ampicillin) Give the first dose in the clinic. The child MUST be discussed with a doctor and reviewed as soon as possible. *IV flush mls/kg of NS. Child should be checked by a nurse every 6 hours and by a doctor or medic every day. **Maintenance fluid (D5NS) Obtain a chest x-ray. Weight. Fluid ml/hour. 2kg. 8. 4kg kg kg kg kg kg kg kg kg kg kg kg. 69. Monitor and ensure oxygen saturations >90% Ensure that the child is receiving adequate fluid. Encourage breastfeeding and oral fluids. If child cannot drink: For Severe Pneumonia: pass a nasogastric tube and give maintenance fluid in one hourly amounts, or, For Very Severe Pneumonia give IV flush* if dehydrated and start on D5NS maintenance, the doctor and all medics on duty must be aware of this child, especially overnight. Give paracetamol (15mg/kg as needed up to 4 times a day) for fever.")
7
Pneumonia Protocol: Infants and Children > 2 months
Very Severe Pneumonia Severe Pneumonia Improvement after 48 hours? Improvement after 48 hours? No Yes Yes No Look for complications like Effusion/empysema Look for complications Oral amoxicillin for 5 days Change to ceftriaxone 50-100mg/kg BID for 10 days Consider cloxacillin (50mg/kg IV QID) After 5 days if the child has responded well change to oral amoxicillin and oral chloramphenical for a further 5 days Treat complications if found Complications include: Empyaema* Pleural effusion* Lung abscess* *May need surgical intervention If the child improves on cloxacillin continue cloxacillin orally 4 times a day for a total course of 3 weeks Antibiotic treatment can be changed by a doctor when blood culture results are available
 After 5 days if the child has responded well change to oral amoxicillin and oral chloramphenical for a further 5 days. Treat complications if found. Complications include: Empyaema* Pleural effusion* Lung abscess* *May need surgical intervention. If the child improves on cloxacillin continue cloxacillin orally 4 times a day for a total course of 3 weeks. Antibiotic treatment can be changed by a doctor when blood culture results are available.")
8
Peak flow if child older than 7 years
Asthma Treatment Protocol Assess Severity Peak flow if child older than 7 years Mild / Moderate No respiratory distress RR normal No / minimal chest indrawing Peak flow >70% predicted Saturations >92% in air Severe Unable to talk in sentences Fast respiratory rate Chest indrawing Nasal flaring Peak flow 33-50% predicted Saturations <92% in air Life Threatening Pale or cyanosis Poor respiratory effort Exhausted Confusion Silent chest Peak flow <33% 5-10 puffs salbutamol via spacer (infants with facemask) Nebulized salbutamol 5mg every 20 minutes for 1 hour Prednisolone 1mg/kg (max 40mg) Oxygen to keep O2 Saturations >92% Nebulized salbutamol 5mg every 20 minutes for 1 hour Prednisolone 1mg/kg (max 40mg) or IV hydrocortisone (see emergency drug chart for dose) Oxygen to keep O2 Saturations >92% Reassess after one hour No Improvement Improvement Call the Doctor Yes No Yes Start IV aminophylline 5mg/kg (max 500mg) over 1 hour every 6 hours STOP if the child starts to vomit, PR> 180, develops a headache or has a convulsion Chest X-ray (rule out pneumothorax) Discharge Ask to return if becomes worse Ensure good inhaler technique and adequate drug supply Admit 1 hourly observations until improvement maintained Salbutamol nebulizer every 2-4 hours Prednisolone for 3 days Close observation Salbutamol nebulizer every hour Prednisolone for 3 days Consider Antibiotics (as per ARI protocol) only if the child has a fever
 Nebulized salbutamol 5mg every 20 minutes for 1 hour. Prednisolone 1mg/kg (max 40mg) Oxygen to keep O2 Saturations >92% Nebulized salbutamol 5mg every 20 minutes for 1 hour. Prednisolone 1mg/kg (max 40mg) or IV hydrocortisone (see emergency drug chart for dose) Oxygen to keep O2 Saturations >92% Reassess after one hour. No. Improvement. Improvement. Call the Doctor. Yes. No. Yes. Start IV aminophylline 5mg/kg (max 500mg) over 1 hour every 6 hours. STOP if the child starts to vomit, PR> 180, develops a headache or has a convulsion. Chest X-ray (rule out pneumothorax) Discharge. Ask to return if becomes worse. Ensure good inhaler technique and adequate drug supply. Admit. 1 hourly observations until improvement maintained. Salbutamol nebulizer every 2-4 hours. Prednisolone for 3 days. Close observation. Salbutamol nebulizer every hour. Prednisolone for 3 days. Consider Antibiotics (as per ARI protocol) only if the child has a fever.")
9
Symptomatic treatment Treat using the Pneumonia Protocol
Bronchiolitis Treatment Protocol Common cold Runny nose Blocked nose Wet sounding cough Bilateral crepitations Wheeze Mild Infant feeding well No signs of respiratory distress Moderate Feeding for shorter time Mild chest indrawing No cyanosis RR not increased Severe Not feeding well RR increased Signs of respiratory distress Discharge home Symptomatic treatment Ask the mother to return if the baby develops respiratory distress or cannot feed Feeding compromised < 3 months Born premature Other medical conditions Mother not coping No Nebulized salbutamol 5mg every 20 minutes for 1 hour, if Improvement every 1 hour prn. If No improvement can d/c. if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. Yes Admit for observation of feeding (child might need NGT fluids) and respiratory rate If wheeze is present give 5 puffs of salbutamol via a spacer, if there is an improvement in the child’s condition give 5 puffs via a spacer QID Treat using the Pneumonia Protocol
 nebulized. Yes. Admit for observation of feeding (child might need NGT fluids) and respiratory rate. If wheeze is present give 5 puffs of salbutamol via a spacer, if there is an improvement in the child’s condition give 5 puffs via a spacer QID. Treat using the Pneumonia Protocol.")
10
Choking Child Protocol
Stridor Treatment Protocol Stridor Definition: harsh breathing noise (DURING INSPIRATION) produced by obstruction to breathing in the larynx or trachea. It is one of the common features of upper airway obstruction with hoarseness and barking cough Leave the child in a comfortable position DO NOT distress the child Croup Epiglottitis Foreign body inhalation Anaphylaxis Symptoms Coryzal onset No drooling Barking cough Able to drink Harsh stridor Hoarse voice Symptoms Rapid onset Toxic appearance Drooling Temp >38.5°c Symptoms Choking Sudden onset Symptoms Skin rash (urticaria) Itching Oedema Treatment IM adrenaline/epinephrine: 0.05ml <6months 0.012ml 6 mths – 5 years 0.25ml 6 years – 11 years 0.5ml 12 years+ Hydrocortisone 25mg TID <1year 50mg TID 1yr – 5 years 100mg TID 6 years – 11 years 250mg TID 12 years+ If wheeze 5mg nebulized salbutamol Chlorpheniramine 2.5mg QID <1year 5mg QID 1yr – 5 years 10mg QID 6 years – 11 years 20mg QID 12 years+ Treatment Moderate respiratory distress – prednisolone 2mg/kg (max 40mg) Severe respiratory distress – Prednisolone and 5ml 1:1000 adrenaline (epinephrine) nebulized Treatment Contact Surgery Prednisolone 2mg/kg (max 40mg) 5ml 1:1000 adrenaline nebulized Ceftriaxone 50mg/kg IM Treatment Choking Child Protocol
 produced by obstruction to breathing in the larynx or trachea. It is one of the common features of upper airway obstruction with hoarseness and barking cough. Leave the child in a comfortable position. DO NOT distress the child. Croup. Epiglottitis. Foreign body inhalation. Anaphylaxis. Symptoms. Coryzal onset. No drooling. Barking cough. Able to drink. Harsh stridor. Hoarse voice. Symptoms. Rapid onset. Toxic appearance. Drooling. Temp >38.5°c. Symptoms. Choking. Sudden onset. Symptoms. Skin rash (urticaria) Itching. Oedema. Treatment. IM adrenaline/epinephrine: 0.05ml <6months ml 6 mths – 5 years. 0.25ml 6 years – 11 years. 0.5ml 12 years+ Hydrocortisone. 25mg TID <1year. 50mg TID 1yr – 5 years. 100mg TID 6 years – 11 years. 250mg TID 12 years+ If wheeze 5mg nebulized salbutamol. Chlorpheniramine. 2.5mg QID <1year. 5mg QID 1yr – 5 years. 10mg QID 6 years – 11 years. 20mg QID 12 years+ Treatment. Moderate respiratory distress – prednisolone 2mg/kg (max 40mg) Severe respiratory distress – Prednisolone and 5ml 1:1000 adrenaline (epinephrine) nebulized. Treatment. Contact Surgery. Prednisolone 2mg/kg (max 40mg) 5ml 1:1000 adrenaline nebulized. Ceftriaxone 50mg/kg IM. Treatment. Choking Child Protocol.")
11
Case 1 4 year old with cc of cough, shortness of breath two days
No fevers Examination RR 72, O2 sats 88%, chest in-drawing Bilateral wheezes throughout Able to talk only in 1 and 2 word sentences What do you want to do?

12
Unwell child or infant older than 2 months
Exclude malaria Take a full history and perform an examination using unwell child and infant history and examination form What is the child’s main complaint/symptom? Difficulty in breathing and cough Diarrhoea Fever (not malaria) Irritability, neck stiffness or bulging fontanelle Acute Respiratory Distress Protocol Gastroenteritis Treatment Protocol Septic Child Protocol Meningitis Treatment Protocol
 Irritability, neck stiffness or bulging fontanelle. Acute Respiratory Distress. Protocol. Gastroenteritis Treatment Protocol. Septic Child Protocol. Meningitis Treatment Protocol.")
13
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardia and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
14
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardia and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
15
Peak flow if child older than 7 years
Asthma Treatment Protocol Assess Severity Peak flow if child older than 7 years Mild / Moderate No respiratory distress RR normal No / minimal chest indrawing Peak flow >70% predicted Saturations >92% in air Severe Unable to talk in sentences Fast respiratory rate Chest indrawing Nasal flaring Peak flow 33-50% predicted Saturations <92% in air Life Threatening Pale or cyanosis Poor respiratory effort Exhausted Confusion Silent chest Peak flow <33% Nebulized salbutamol 5mg every 20 minutes for 1 hour Prednisolone 1mg/kg (max 40mg) Oxygen to keep O2 Saturations >92% Improvement Yes Admit 1 hourly observations until improvement maintained Salbutamol nebulizer every 2-4 hours Prednisolone for 3 days Consider Antibiotics (as per ARI protocol) only if the child has a fever
 Oxygen to keep O2 Saturations >92% Improvement. Yes. Admit. 1 hourly observations until improvement maintained. Salbutamol nebulizer every 2-4 hours. Prednisolone for 3 days. Consider Antibiotics (as per ARI protocol) only if the child has a fever.")
16
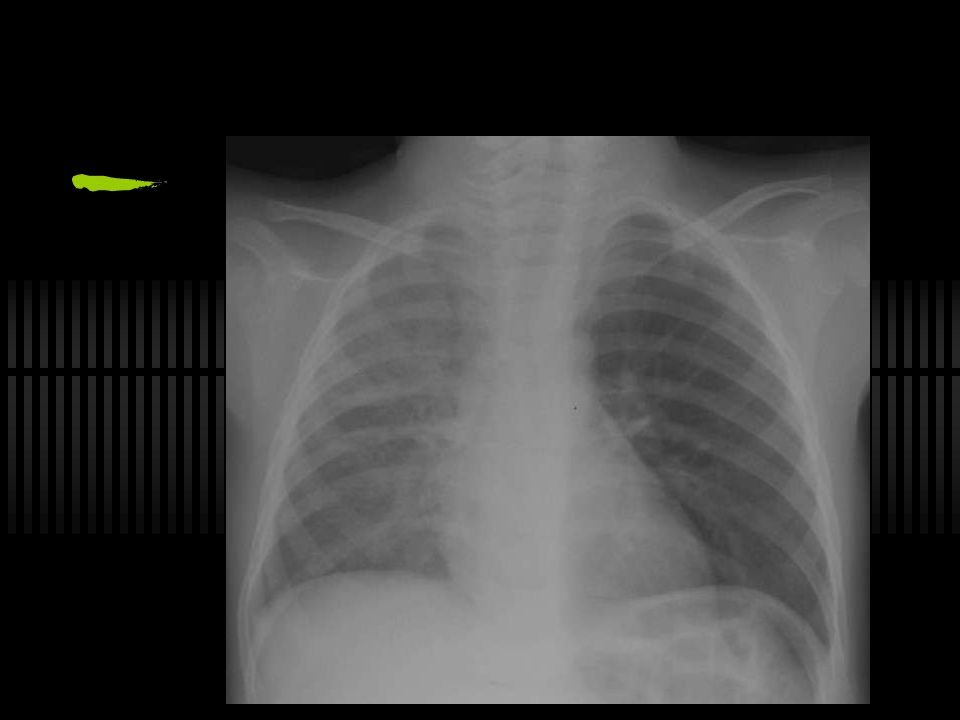
Case 2 22 month old, health, sudden onset of cough 10 days ago, fever 5 days ago, on antibiotics for 4 days, still fever. Temp 38.8C, RR 72, O2 sats 91% General: tachypnic, mild chest in-drawing Resp: reduced air entry on L hemithorax, no other abnormalities

17
Unwell child or infant older than 2 months
Exclude malaria Take a full history and perform an examination using unwell child and infant history and examination form What is the child’s main complaint/symptom? Difficulty in breathing and cough Diarrhoea Fever (not malaria) Irritability, neck stiffness or bulging fontanelle Acute Respiratory Distress Protocol Gastroenteritis Treatment Protocol Septic Child Protocol Meningitis Treatment Protocol
 Irritability, neck stiffness or bulging fontanelle. Acute Respiratory Distress. Protocol. Gastroenteritis Treatment Protocol. Septic Child Protocol. Meningitis Treatment Protocol.")
18
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardic and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
21
Case 3 13 month old with cough, runny nose, wet cough for 2 days. Not eating or drinking well. Examination T 38.1 C, RR 87, O2 sats 83%, weight 12 Kg. General: lethargic HEENT: coryza Resp: nasal flaring, super-clavicular and chest in-drawing, abdominal breathing, bilateral wheeze/rhonchi throughout with some scattered crepitations.

22
Unwell child or infant older than 2 months
Exclude malaria Take a full history and perform an examination using unwell child and infant history and examination form What is the child’s main complaint/symptom? Difficulty in breathing and cough Diarrhoea Fever (not malaria) Irritability, neck stiffness or bulging fontanelle Acute Respiratory Distress Protocol Gastroenteritis Treatment Protocol Septic Child Protocol Meningitis Treatment Protocol
 Irritability, neck stiffness or bulging fontanelle. Acute Respiratory Distress. Protocol. Gastroenteritis Treatment Protocol. Septic Child Protocol. Meningitis Treatment Protocol.")
23
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardic and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
24
Treat using the Pneumonia Protocol
Bronchiolitis Treatment Protocol Common cold Runny nose Blocked nose Wet sounding cough Bilateral crepitations Wheeze Mild Infant feeding well No signs of respiratory distress Moderate Feeding for shorter time Mild chest indrawing No cyanosis RR not increased Severe Not feeding well RR increased Signs of respiratory distress Nebulized salbutamol 5mg every 20 minutes for 1 hour, if Improvement every 1 hour prn. If No improvement can d/c. if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. Treat using the Pneumonia Protocol
 nebulized. Treat using the Pneumonia Protocol.")
25
Pneumonia Protocol: Infants and Children > 2 months
Does the infant have indrawing of the chest wall? Yes No Does the infant have any of the following? Central cyanosis off oxygen Severe respiratory distress Inability to drink Yes No Very Severe Pneumonia Severe Pneumonia Pneumonia Ceftriaxone Ampicillin plus Chloramphenicol Amoxicillin or Ampicillin Worsens or fails to respond in hours

26
Pneumonia Protocol: Infants and Children > 2 months
Very Severe Pneumonia Severe Pneumonia Pneumonia Ceftriaxone ( mg/kg IV divided Bid (may give IM if no IV access) Give ampicillin (100 mg/kg IV/IM every 6 hours) and chloramphenical (50 mg/kg every 8 hours) for at least 48 hours Give oral amoxicillin (or IV ampicillin) Give the first dose in the clinic The child MUST be discussed with a doctor and reviewed as soon as possible *IV flush 10-20 mls/kg of NS Child should be checked by a nurse every 6 hours and by a doctor or medic every day **Maintenance fluid (D5NS) Obtain a chest x-ray Weight Fluid ml/hour 2kg 8 4kg 16 6kg 25 8kg 33 10kg 42 12kg 46 14kg 50 16kg 54 18kg 58 20kg 63 22kg 65 24kg 67 26kg 69 Monitor and ensure oxygen saturations >90% Ensure that the child is receiving adequate fluid Encourage breastfeeding and oral fluids If child cannot drink: For Severe Pneumonia: pass a nasogastric tube and give maintenance fluid in one hourly amounts, or, For Very Severe Pneumonia give IV flush* if dehydrated and start on D5NS maintenance, the doctor and all medics on duty must be aware of this child, especially overnight Give paracetamol (15mg/kg as needed up to 4 times a day) for fever
 Give ampicillin (100 mg/kg IV/IM every 6 hours) and chloramphenical (50 mg/kg every 8 hours) for at least 48 hours. Give oral amoxicillin (or IV ampicillin) Give the first dose in the clinic. The child MUST be discussed with a doctor and reviewed as soon as possible. *IV flush mls/kg of NS. Child should be checked by a nurse every 6 hours and by a doctor or medic every day. **Maintenance fluid (D5NS) Obtain a chest x-ray. Weight. Fluid ml/hour. 2kg. 8. 4kg kg kg kg kg kg kg kg kg kg kg kg. 69. Monitor and ensure oxygen saturations >90% Ensure that the child is receiving adequate fluid. Encourage breastfeeding and oral fluids. If child cannot drink: For Severe Pneumonia: pass a nasogastric tube and give maintenance fluid in one hourly amounts, or, For Very Severe Pneumonia give IV flush* if dehydrated and start on D5NS maintenance, the doctor and all medics on duty must be aware of this child, especially overnight. Give paracetamol (15mg/kg as needed up to 4 times a day) for fever.")
27
Case 3 You give three salbutamol nebs over one hour, no improvement.
Started on oxygen and Ceftriaxone. Chest x-ray pending You need to give fluids, what are you going to give?

28
Pneumonia Protocol: Infants and Children > 2 months
Very Severe Pneumonia Severe Pneumonia Pneumonia Ceftriaxone ( mg/kg IV divided Bid (may give IM if no IV access) Give ampicillin (100 mg/kg IV/IM every 6 hours) and chloramphenical (50 mg/kg every 8 hours) for at least 48 hours Give oral amoxicillin (or IV ampicillin) Give the first dose in the clinic The child MUST be discussed with a doctor and reviewed as soon as possible *IV flush 10-20 mls/kg of NS Child should be checked by a nurse every 6 hours and by a doctor or medic every day **Maintenance fluid (D5NS) Obtain a chest x-ray Weight Fluid ml/hour 2kg 8 4kg 16 6kg 25 8kg 33 10kg 42 12kg 46 14kg 50 16kg 54 18kg 58 20kg 63 22kg 65 24kg 67 26kg 69 Monitor and ensure oxygen saturations >90% Ensure that the child is receiving adequate fluid Encourage breastfeeding and oral fluids If child cannot drink: For Severe Pneumonia: pass a nasogastric tube and give maintenance fluid in one hourly amounts, or, For Very Severe Pneumonia give IV flush* if dehydrated and start on D5NS maintenance, the doctor and all medics on duty must be aware of this child, especially overnight Give paracetamol (15mg/kg as needed up to 4 times a day) for fever
 Give ampicillin (100 mg/kg IV/IM every 6 hours) and chloramphenical (50 mg/kg every 8 hours) for at least 48 hours. Give oral amoxicillin (or IV ampicillin) Give the first dose in the clinic. The child MUST be discussed with a doctor and reviewed as soon as possible. *IV flush mls/kg of NS. Child should be checked by a nurse every 6 hours and by a doctor or medic every day. **Maintenance fluid (D5NS) Obtain a chest x-ray. Weight. Fluid ml/hour. 2kg. 8. 4kg kg kg kg kg kg kg kg kg kg kg kg. 69. Monitor and ensure oxygen saturations >90% Ensure that the child is receiving adequate fluid. Encourage breastfeeding and oral fluids. If child cannot drink: For Severe Pneumonia: pass a nasogastric tube and give maintenance fluid in one hourly amounts, or, For Very Severe Pneumonia give IV flush* if dehydrated and start on D5NS maintenance, the doctor and all medics on duty must be aware of this child, especially overnight. Give paracetamol (15mg/kg as needed up to 4 times a day) for fever.")
29
Weight was 12 Kilograms: Flush: 12 X 20 ml/kg = 240 mls. NS
*IV flush 10-20 mls/kg of NS Weight was 12 Kilograms: Flush: 12 X 20 ml/kg = 240 mls. NS Maintenance: 12 Kg. = 46 D5NS **Maintenance fluid (D5NS) Weight Fluid ml/hour 2kg 8 4kg 16 6kg 25 8kg 33 10kg 42 12kg 46 14kg 50 16kg 54 18kg 58 20kg 63 22kg 65 24kg 67 26kg 69
 Weight. Fluid ml/hour. 2kg. 8. 4kg kg kg kg kg kg kg kg kg kg kg kg. 69.")
30
Case 3 Respiratory rate increases to 90 over the next 12 hours despite previous therapy. Oxygen sats, originally over 92% on oxygen now 78%. Child has increased nasal flaring, chest in-drawing, and poor capillary refill. What do you want to do?

31
Treat using the Pneumonia Protocol
Bronchiolitis Treatment Protocol Common cold Runny nose Blocked nose Wet sounding cough Bilateral crepitations Wheeze Mild Infant feeding well No signs of respiratory distress Moderate Feeding for shorter time Mild chest indrawing No cyanosis RR not increased Severe Not feeding well RR increased Signs of respiratory distress Nebulized salbutamol 5mg every 20 minutes for 1 hour, if Improvement every 1 hour prn. If No improvement can d/c. if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. Treat using the Pneumonia Protocol
 nebulized. Treat using the Pneumonia Protocol.")
32
Case 4 4 y.o. with cc of fever and cough for two days Examination
Worse at night Examination T 39 C, rr 25, o2 sats 95% General: Barky cough Resp: CTA B except upper airways sounds.

33
Unwell child or infant older than 2 months
Exclude malaria--POSITIVE Take a full history and perform an examination using unwell child and infant history and examination form What is the child’s main complaint/symptom? Difficulty in breathing and cough Diarrhoea Fever (not malaria) Irritability, neck stiffness or bulging fontanelle Acute Respiratory Distress Protocol Gastroenteritis Treatment Protocol Septic Child Protocol Meningitis Treatment Protocol
 Irritability, neck stiffness or bulging fontanelle. Acute Respiratory Distress. Protocol. Gastroenteritis Treatment Protocol. Septic Child Protocol. Meningitis Treatment Protocol.")
34
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardic and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
35
Choking Child Protocol
Stridor Treatment Protocol Stridor Definition: harsh breathing noise (DURING INSPIRATION) produced by obstruction to breathing in the larynx or trachea. It is one of the common features of upper airway obstruction with hoarseness and barking cough Leave the child in a comfortable position DO NOT distress the child Croup Epiglottitis Foreign body inhalation Anaphylaxis Symptoms Coryzal onset No drooling Barking cough Able to drink Harsh stridor Hoarse voice Symptoms Rapid onset Toxic appearance Drooling Temp >38.5°c Symptoms Choking Sudden onset Symptoms Skin rash (urticaria) Itching Oedema Treatment IM adrenaline/epinephrine: 0.05ml <6months 0.012ml 6 mths – 5 years 0.25ml 6 years – 11 years 0.5ml 12 years+ Hydrocortisone 25mg TID <1year 50mg TID 1yr – 5 years 100mg TID 6 years – 11 years 250mg TID 12 years+ If wheeze 5mg nebulized salbutamol Chlorpheniramine 2.5mg QID <1year 5mg QID 1yr – 5 years 10mg QID 6 years – 11 years 20mg QID 12 years+ Treatment Moderate respiratory distress – prednisolone 2mg/kg (max 40mg) Severe respiratory distress – Prednisolone and 5ml 1:1000 adrenaline (epinephrine) nebulized Treatment Contact Surgery Prednisolone 2mg/kg (max 40mg) 5ml 1:1000 adrenaline nebulized Ceftriaxone 50mg/kg IM Treatment Choking Child Protocol
 produced by obstruction to breathing in the larynx or trachea. It is one of the common features of upper airway obstruction with hoarseness and barking cough. Leave the child in a comfortable position. DO NOT distress the child. Croup. Epiglottitis. Foreign body inhalation. Anaphylaxis. Symptoms. Coryzal onset. No drooling. Barking cough. Able to drink. Harsh stridor. Hoarse voice. Symptoms. Rapid onset. Toxic appearance. Drooling. Temp >38.5°c. Symptoms. Choking. Sudden onset. Symptoms. Skin rash (urticaria) Itching. Oedema. Treatment. IM adrenaline/epinephrine: 0.05ml <6months ml 6 mths – 5 years. 0.25ml 6 years – 11 years. 0.5ml 12 years+ Hydrocortisone. 25mg TID <1year. 50mg TID 1yr – 5 years. 100mg TID 6 years – 11 years. 250mg TID 12 years+ If wheeze 5mg nebulized salbutamol. Chlorpheniramine. 2.5mg QID <1year. 5mg QID 1yr – 5 years. 10mg QID 6 years – 11 years. 20mg QID 12 years+ Treatment. Moderate respiratory distress – prednisolone 2mg/kg (max 40mg) Severe respiratory distress – Prednisolone and 5ml 1:1000 adrenaline (epinephrine) nebulized. Treatment. Contact Surgery. Prednisolone 2mg/kg (max 40mg) 5ml 1:1000 adrenaline nebulized. Ceftriaxone 50mg/kg IM. Treatment. Choking Child Protocol.")
36
Stridor Treatment Protocol Stridor
Definition: harsh breathing noise (DURING INSPIRATION) produced by obstruction to breathing in the larynx or trachea. It is one of the common features of upper airway obstruction with hoarseness and barking cough Leave the child in a comfortable position DO NOT distress the child Croup Epiglottitis Foreign body inhalation Anaphylaxis Symptoms Coryzal onset No drooling Barking cough Able to drink Harsh stridor Hoarse voice Treatment Moderate respiratory distress – prednisolone 2mg/kg (max 40mg) Severe respiratory distress – Prednisolone and 5ml 1:1000 adrenaline (epinephrine) nebulized
 produced by obstruction to breathing in the larynx or trachea. It is one of the common features of upper airway obstruction with hoarseness and barking cough. Leave the child in a comfortable position. DO NOT distress the child. Croup. Epiglottitis. Foreign body inhalation. Anaphylaxis. Symptoms. Coryzal onset. No drooling. Barking cough. Able to drink. Harsh stridor. Hoarse voice. Treatment. Moderate respiratory distress – prednisolone 2mg/kg (max 40mg) Severe respiratory distress – Prednisolone and 5ml 1:1000 adrenaline (epinephrine) nebulized.")
37
Case 5 8 year old with known asthma, with cough for 3 days now acutely short of breath. Examination T 38 C, rr 48, 02 sats 91% Gen: tachypnic, unable to speak in full sentences Skin: crepitations in neck and supra-clavicular Resp: Bilateral wheezes throughout

38
Unwell child or infant older than 2 months
Exclude malaria Take a full history and perform an examination using unwell child and infant history and examination form What is the child’s main complaint/symptom? Difficulty in breathing and cough Diarrhoea Fever (not malaria) Irritability, neck stiffness or bulging fontanelle Acute Respiratory Distress Protocol Gastroenteritis Treatment Protocol Septic Child Protocol Meningitis Treatment Protocol
 Irritability, neck stiffness or bulging fontanelle. Acute Respiratory Distress. Protocol. Gastroenteritis Treatment Protocol. Septic Child Protocol. Meningitis Treatment Protocol.")
39
Acute Respiratory Distress Protocol
Count respiratory rate over 1 minute >50 breaths and child 2 – 11 months >40 breaths and child 1-5 years No Go to septic child protocol Yes Take oxygen saturations If < 90% start oxygen If the child is less than 2 years and has wet sounding crepitations on auscultation and no increase in RR consider Bronchioloitis as a diagnosis Bronchiolitis Protocol* Does the child have any of the following? Gallop rhythm Heart murmur Enlarged palpable liver Barking cough Stridor Hoarse voice On auscultation of the chest the predominant feature is wheeze? Sudden onset of symptoms Possible Cardiac Failure frequently aneamic Consider furosemide 1mg/kg Blood transfusion if tachycardic and hgb less then 5** Call the doctor Consider Foreign Body Aspiration (inspiratory/expiratory chest x-ray, in babies left and right lateral x-rays) Upper Airway Obstruction Go to Stridor Treatment Protocol Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma Protocol If no to all of the above move to the Pneumonia Protocol *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.
 Upper Airway Obstruction. Go to Stridor Treatment Protocol. Child > 2- 3 years previous wheeze or diagnosis of asthma: follow Acute Asthma. Protocol. If no to all of the above move to the Pneumonia Protocol. *if severe, may attempt 5ml 1:1000 adrenaline (epinephrine) nebulized. **discuss with physician if signs of heart failure but aneamia with a Hgb. more than 5.")
40
Peak flow if child older than 7 years
Asthma Treatment Protocol Assess Severity Peak flow if child older than 7 years Mild / Moderate No respiratory distress RR normal No / minimal chest indrawing Peak flow >70% predicted Saturations >92% in air Severe Unable to talk in sentences Fast respiratory rate Chest indrawing Nasal flaring Peak flow 33-50% predicted Saturations <92% in air Life Threatening Pale or cyanosis Poor respiratory effort Exhausted Confusion Silent chest Peak flow <33% Nebulized salbutamol 5mg every 20 minutes for 1 hour Prednisolone 1mg/kg (max 40mg) Oxygen to keep O2 Saturations >92% Improvement Yes Admit 1 hourly observations until improvement maintained Salbutamol nebulizer every 2-4 hours Prednisolone for 3 days Consider Antibiotics (as per ARI protocol) only if the child has a fever
 Oxygen to keep O2 Saturations >92% Improvement. Yes. Admit. 1 hourly observations until improvement maintained. Salbutamol nebulizer every 2-4 hours. Prednisolone for 3 days. Consider Antibiotics (as per ARI protocol) only if the child has a fever.")
41
Case 5 No improvement with therapy, now what?

44
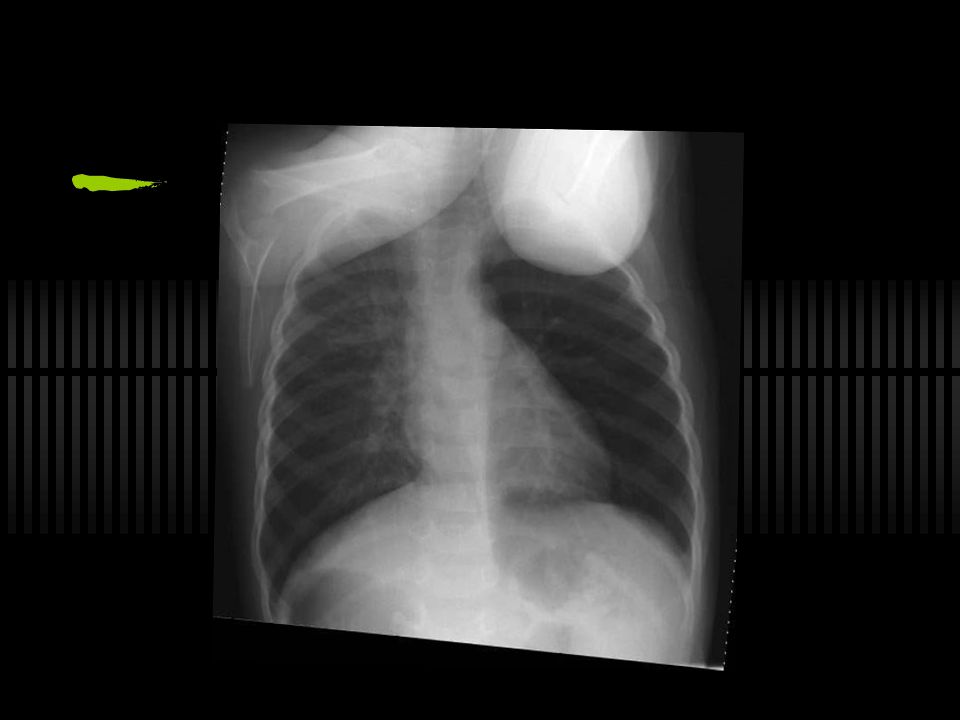
Case 6 3 year old with cough for three days, drooling. No other symptoms. Examination: T 37.8 C, rr 21, O2 sats 98% General NAD Respiratory: CTA B

47
...with a vision for the children of the world: that every one
of them - without exception - lives a full and healthy life, with rights secured and protected, freed from poverty, violence and discrimination --UNICEF State of the World’s Children, 2000

Similar presentations












: Jeff Holmes MD, Maine Medical Center License:>")








: i1-i92.>")

