Download presentation
Presentation is loading. Please wait.

1
BONE DENSITOMETRY

2
Bone Densitometry NOMENCLATURE:
DXA NOT DEXA Dual-energy X-ray Absorptiometry BMD bone mineral density VFA vertebral fracture analysis (not DVA, LVA, IVA, RVA, etc.)
")
3
Bone Densitometry T-score number of standard deviations the patient’s BMD is above or below average peak BMD of young adult reference population. Z-score number of standard deviation the patient’s BMD is above or below age- and sex-matched mean reference value. Z-score should be population specific where adequate reference data exist, including ethnicity.

4
T-score WHO CLASSIFICATION Normal T-score ≥ -1.0
Low bone mass (osteopenia) T-score between -1.0 and -2.5 Osteoporosis T-score ≤ -2.5 Severe osteoporosis T-score ≤ -2.5 with history of fragility fracture
 T-score between -1.0 and Osteoporosis T-score ≤ Severe osteoporosis. T-score ≤ -2.5 with history of fragility fracture.")
5
Z-score Z-scores are used instead of T-scores for children, pre-menopausal women and men younger than age 50! A Z-score ≤ -2.0 is defined as "below the expected range for age." A Z-score > -2.0 is "within the expected range for age."

6
Z-score Pediatric patients (ages 5-19) Require dedicated software package and need to scan lumbar spine and total body minus head. NOT hip. Do not use T-scores. A Z-score ≤ -2.0 is defined as "below the expected range for age." A Z-score > -2.0 is "within the expected range for age."
 Require dedicated software package and need to scan lumbar spine and total body minus head. NOT hip. Do not use T-scores. A Z-score ≤ -2.0 is defined as below the expected range for age. A Z-score > -2.0 is within the expected range for age.")
7
Bone Cortical or compact = dense cortex Trabecular or cancellous = marrow area

8
Bone Spine: about 2/3 trabecular/cancellous bone on PA view, remainder cortical/compact bone. Hip: 25% trabecular bone at neck and 50% trabecular bone at trochanter Forearm: almost entirely cortical bone and only 1% trabecular bone

9
Osteoporosis Skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture. Bone strength reflects the integration of two main features: bone density and bone quality. There are no symptoms from low bone mass unless fracture occurs.

10
Why do we care? Fractures painful Debilitating Decrease mobility
Decrease independence Expensive

11
Why do we care? 2/3 of vertebral fractures are clinically silent –i.e. morphometric, discovered by X-ray or imaging! Only 25-30% of fractures seen on X-ray are diagnosed clinically.

12
Why do we care? Complications of hip fractures --especially nursing home patients: 24-30% excess mortality within 1 year 50% of survivors are permanently incapacitated 20% of survivors require long-term nursing home care

13
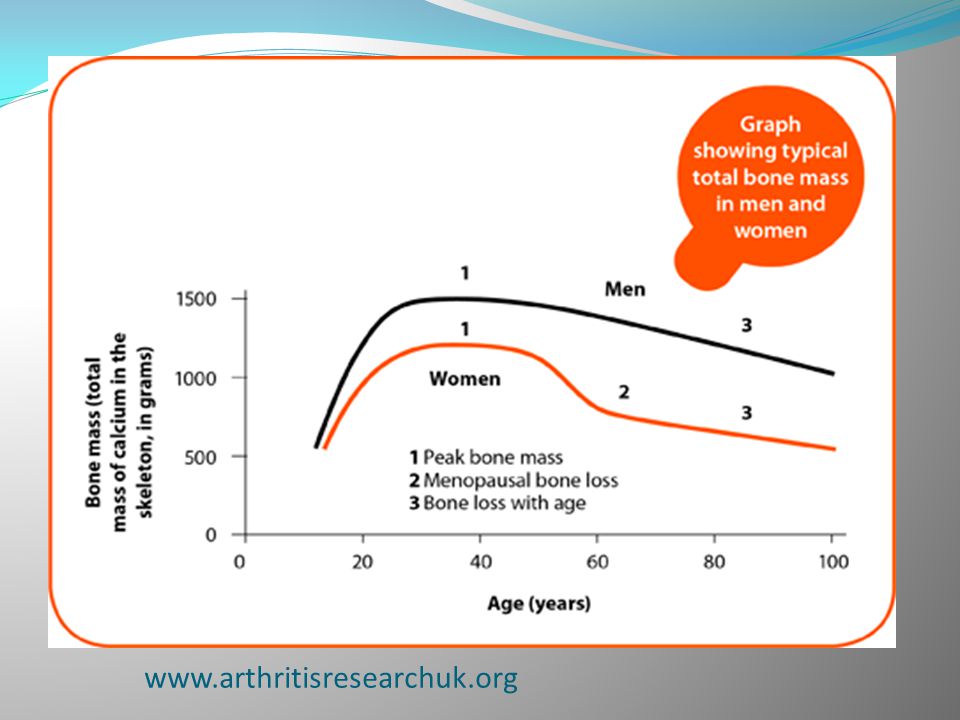
Bone density on average:
Males > Females Blacks > Whites Peak bone mass achieved in teens or early 20's. Then relative plateau until 35 years old.

14
Bone density on average:
Then age-related bone loss occurs at a rate of 0.5%-1.0%/year. Bone loss accelerates with menopause ( %/year) and accelerated phase lasts 5-10 years. Age-related bone loss continues, with bone loss eventually going back down to pre-adolescent levels. That’s why screening is so linked to menopause.
 and accelerated phase lasts 5-10 years. Age-related bone loss continues, with bone loss eventually going back down to pre-adolescent levels. That’s why screening is so linked to menopause.")
16
Central DXA Current gold standard for DIAGNOSTIC classification of BMD and osteoporosis. However, multiple other techniques are well-validated for fracture risk assessment but not diagnosis of osteoporosis.

17
Central DXA Excellent reproducibility (but it’s up to us!) Low radiation dose (1-10 µSv) or 1/10 the dose of a CXR, about one day’s worth of natural daily background exposure. Most epidemiologic studies and clinical pharmaceutical trials backing it up.
 Low radiation dose (1-10 µSv) or 1/10 the dose of a CXR, about one day’s worth of natural daily background exposure. Most epidemiologic studies and clinical pharmaceutical trials backing it up.")
18
Indications for BMD Testing
Women ≥ 65 y/o. Postmenopausal women (natural or surgical) < 65 y/o with risk factors for fx Women during the menopausal transition (perimenopausal) with clinical risk factors for fx, e.g. low body weight, prior fx, or high-risk medication use. Men ≥ 70 y/o. Men < 70 y/o with clinical risk factors for fracture. Adults with a fragility fracture*.
 < 65 y/o with risk factors for fx. Women during the menopausal transition (perimenopausal) with clinical risk factors for fx, e.g. low body weight, prior fx, or high-risk medication use. Men ≥ 70 y/o. Men < 70 y/o with clinical risk factors for fracture. Adults with a fragility fracture*.")
19
Indications for BMD Testing
Adults with a disease or condition associated with low bone mass or bone loss. Adults taking medications associated with low bone mass or bone loss. Anyone being considered for pharmacologic therapy. Anyone being treated, to monitor treatment effect. Anyone not receiving therapy in whom evidence of bone loss would lead to treatment.

20
FRAGILITY FRACTURE Fracture from falling from standing height or lower, at walking speed or slower, often vertebral, hip or wrist. Fracture occurring in the absence of obvious trauma or minimal trauma not usually expected to cause a fracture. Excludes pathologic fractures (underlying abnormal bone, e.g. bone metastasis), and fractures of digits, hands, ankles & feet & skull fractures.
, and fractures of digits, hands, ankles & feet & skull fractures.")
21
FRAGILITY FRACTURE Although not part of the WHO classification, the presence of a fragility fracture -regardless of T-score– should be considered diagnostic of osteoporosis ! (provided other causes for the fracture have been excluded)
")
23
Spine Use positioning block to straighten lordosis. Centered
Straight and not tilted or leaning If scoliotic, try to center curvature in the middle, off set pelvis if necessary Centering minimizes parallax effect, especially for Hologic.

24
Spine Both iliac crests visible Mid T12 to mid L5 included
12th rib (optional) L3 usually has the longest transverse processes
 L3 usually has the longest transverse processes.")
25
Spine Example GE

26
Spine Example Hologic

27
Spine Look at raw data and histograms to confirm disk levels. Angle as appropriate. Check ROI and bone margins -excluding large osteophytes? -too narrow and excluding bone?

28
Spine If have difficulty numbering due to rib variability and transitional vertebrae, count from below, with L4-L5 considered at the iliac crests if possible. Usually L4-5 is at the iliac crests or slightly lower. 1 in 6 patients have variants! 4,5 or 6 lumbar vertebrae and lowest ribs T11, T12, or L1. 83.5% have 5 lumbar vertebrae with lowest ribs on T12, 7.5% have 4 lumbar vertebrae with lowest ribs on T11 or T12, 7.2% have 5 lumbar vertebrae with lowest ribs on T11, 1.9% have 6 lumbar vertebrae with lowests ribs on T12 or L1

29
Spine Exclude vertebrae with fracture --check VFA, X-rays too!
Exclude if hardware, vertebroplasty or kyphoplasty (=vertebral augmentation) or laminectomy. Check for artifact, stent grafts, surgical clips, barium, calcification, foreign bodies, bra hooks and underwires, external to patient? If external to patient, remove and repeat!
 or laminectomy. Check for artifact, stent grafts, surgical clips, barium, calcification, foreign bodies, bra hooks and underwires, external to patient If external to patient, remove and repeat!")
30
Spine Careful because DXA does subtract soft tissue! So even if outside the spine ROI it can affect the measurement, especially if within global ROI. Remove, remove, remove if possible and repeat scan. If not then neutralize it. Hologic ignores everything outside of global ROI. GE I don’t know.

31
Spine QA QA IMPORTANT!!! Look at BMDs and T-scores! L1 usually lowest BMD. BMC and area progressively increase from L1 to L4. BMD tends to increase from L1 to L3. BMD of L4 similar or less than L3.

32
Spine QA Exclude vertebrae if clearly abnormal and non-assessable within resolution of the system. Exclude vertebra if there is > 1.0 T-score difference between the vertebra in question and adjacent vertebrae. Assess for cause, often increased T-score due to subtle fracture or increased degenerative change & sclerosis (so usually drop high T-score vertebra)
")
33
Spine QA Occasionally see spurious decrease in T-score due to interval surgery or laminectomy –drop low T-score. Sometimes T-scores change > 1.0 between every vertebrae. "Art of medicine" may be invoked on challenging cases. e.g. if dropping a vertebra doesn't change diagnosis may not want to drop it.

34
Spine QA Use all evaluable vertebrae and only exclude vertebrae that are affected by structural change or artifact.

35
Spine QA Use all evaluable vertebrae and only exclude vertebrae that are affected by structural change or artifact. However, if only one evaluable vertebra remains, then must use other skeletal sites and exclude spine. Must have ≥ 2 vertebrae to use spine BMD.

36
Spine QA Use all evaluable vertebrae and only exclude vertebrae that are affected by structural change or artifact. However, if only one evaluable vertebra remains, then must use other skeletal sites and exclude spine. Must have ≥ 2 vertebrae to use spine BMD. If lots of variation between vertebral bodies, likely will need additional imaging of hips/dominant forearm in the future or now!

37
Spine QA COMPARISON QA Check and see if positioning and numbering is the same.

38
Spine QA COMPARISON QA Check and see if positioning and numbering is the same. If numbering is questionable, keep consistent with prior study unless prior study clearly mislabeled.

39
Spine QA COMPARISON QA Check and see if positioning and numbering is the same. If numbering is questionable, keep consistent with prior study unless prior study clearly mislabeled. Some DXA units will let you correct and reanalyze prior data.

40
Spine QA COMPARISON QA Are ROIs similar? Check edges.

41
Spine QA COMPARISON QA Are ROIs similar? Check edges. Compare prior BMDs and T-scores at EVERY level.

42
Spine QA COMPARISON QA Are ROIs similar? Check edges. Compare prior BMDs and T-scores at EVERY level. Is one level or two significantly different?

43
Spine QA COMPARISON QA Are ROIs similar? Check edges. Compare prior BMDs and T-scores at EVERY level. Is one level or two significantly different? Review images for cause. e.g. interval fracture, procedure, overlying artifact, etc..

44
Spine QA COMPARISON QA --we depend on YOU!! Consistency and precision are critical! --Spine BMD has the best precision and is the most responsive to therapy. Patient care is impacted. --Significant BMD changes affect therapy decisions. “Significant” is often just a few or several percent difference.

45
Spine QA COMPARISON QA --we depend on YOU!! Consistency and precision are critical! Precision errors affect health care costs, may result in unnecessary change in treatment (more expensive or more side effects) or lack of treatment or unnecessary specialist referral or additional diagnostic work-up to assess for secondary osteoporosis, patient anxiety, etc..
 or lack of treatment or unnecessary specialist referral or additional diagnostic work-up to assess for secondary osteoporosis, patient anxiety, etc..")
46
Spine QA COMPARISON QA A national bone metabolism and bone health expert reported : #1 reason for referral for significant bone loss, despite appropriate medical therapy… ???

47
Spine QA COMPARISON QA A national bone metabolism and bone health expert reported : #1 reason for referral for significant bone loss, despite appropriate medical therapy… POOR COMPARISON TECHNIQUE!!

48
HIP Positioning -remove shoes and foot in positioning device
Shoes can vary year to year, depending on the season, etc. Shoes can vary year to year, depending on season, etc.

49
HIP Positioning -remove shoes and foot in positioning device
-femoral neck centered in the image .

50
HIP Positioning -remove shoes and foot in positioning device
-femoral neck centered in the image -minimal lesser trochanter apparent (internally rotated)
")
51
HIP Positioning -vertical orientation of diaphysis/shaft

52
HIP Positioning -vertical orientation of diaphysis/shaft
-total hip includes ischium and greater trochanter

53
HIP Positioning -vertical orientation of diaphysis/shaft
-total hip includes ischium and greater trochanter -verify bone margins!

54
HIP Positioning Rule of thumb for outer margins:
5 mm superior to femoral head 5 mm medial to femoral head 5 mm lateral to the greater trochanter 10 mm inferior to lesser trochanter

55
HIP Positioning appropriate ROI box placement--slightly different by manufacturer e.g. femoral neck rectangular ROI should not include ischium if possible (usually can auto-subtract "neutralize" ischium vs. 2nd option narrow the box or 3rd option, move the box)
")
56
HIP Femoral Neck ROI GE Lunar: finds narrowest point of femoral neck and all 4 corners in soft tissue

57
HIP -GE example

58
HIP -GE example

59
HIP Femoral Neck ROI Hologic Discovery: anchors it to the edge of greater trochanter with 3 corners in soft tissue, one corner in bone, touches superomedial margin of greater trochanter 15 mm DO NOT change

60
HIP -Hologic example 3 corners of hip box in soft tissue and 4th corner anchored on bone of greater trochanter. Little lesser trochanter showing. Straight shaft, image centered on femoral neck.

61
HIP Femoral Neck ROI Neither femoral neck box should include greater trochanter or ischium --neutralize ischium if necessary.

62
HIP Lower inferior margin
GE auto selects it based on greater trochanter triangle Hologic supposed to find inferior margin of lesser trochanter and go 1 cm inferior.

63
HIP If foreign body or object external to patient, remove and rescan!
Check for artifacts, surgical clips, metal, calcification, keys, coins, buttons, snaps, zippers, objects external to patient. Exclude hip if prior fracture or surgery. If foreign body or object external to patient, remove and rescan!

64
HIP For diagnosis, use femoral neck or total proximal femur, whichever is lowest. Either hip or bilateral mean hip may be used.

65
HIP COMPARISON QA Total hip is preferred for monitoring and follow-up because of better precision than femoral neck. Mean total hip may be used. Femoral neck only as a final alternative site for follow-up.

66
HIP COMPARISON QA We depend on you!

67
HIP COMPARISON QA We depend on you! Check for similar positioning.

68
HIP COMPARISON QA We depend on you! Check for similar positioning.
Are ROIs similar? Check edges.

69
HIP COMPARISON QA We depend on you!
Compare prior BMDs and T-scores at total hip and femoral neck.

70
HIP COMPARISON QA We depend on you!
Compare prior BMDs and T-scores at total hip and femoral neck. Is one significantly different? Review images for cause. e.g. interval fracture, procedure, overlying artifact, etc..

71
FOREARM Alternate site and not primary preferred site as it does not respond well to therapy Use if another site is not evaluable (e.g. hip replacements, spinal surgery, significant degenerative change/scoliosis, obesity exceeding table weight limit, etc.)
")
72
FOREARM = 1/3 radius BMD (Hologic) Use only 33% radius (GE)
Dominant forearm tends to have higher BMD and we are looking for low BMD. Fractured bone may have higher BMD/sclerosis.

73
FOREARM Non-dominant forearm is recommended for diagnosis.
Use only 33% radius = 1/3 radius BMD Non-dominant forearm is recommended for diagnosis. Dominant forearm tends to have higher BMD and we are looking for low BMD. Fractured bone may have higher BMD/sclerosis.

74
FOREARM Non-dominant forearm is recommended for diagnosis.
Use only 33% radius = 1/3 radius BMD Non-dominant forearm is recommended for diagnosis. If history of fracture of nondominant wrist or forearm as an adult, then use dominant forearm. Dominant forearm tends to have higher BMD and we are looking for low BMD. Fractured bone may have higher BMD/sclerosis.

75
FOREARM However, if patient has hyperparathyroidism always do forearm. Hyperparathyroidism targets cortical bone and remember forearm is 99% cortical bone, so more sensitive.

76
FOREARM QA Nondominant forearm Centered
Radius & ulna straight, parallel to long axis of table Distal cortex of radius & ulna and proximal carpal row visible Evaluate for artifacts , jewelry, watch, buttons, etc. Evaluate margins and edges

77
FOREARM GE example

78
FOREARM Hologic example

79
FOREARM COMPARISON QA --we depend on you! Compare positioning

80
FOREARM COMPARISON QA --we depend on you! Compare positioning
Compare ROIs and edges for consistency

81
FOREARM COMPARISON QA --we depend on you! Compare positioning
Compare ROIs and edges for consistency Check old and new BMDs and T-scores

82
Comparison Cannot accurately compare between different machines due to different: -dual energy methods -calibration and least significant change -detectors -edge detection software -data bases -ROI techniques, maintenance, etc.

83
Comparison Cannot accurately compare between different machines—even if the same model. So generalize… If prior study showed normal BMD and today low bone mass, then trend is worsening. If low bone mass on prior study and today shows low bone mass as well, relatively stable.

84
Comparison So that is why it is so important to be imaged at the same site, same exact DXA unit each year. And why it is so important to be conscientious and careful about positioning and critically reviewing your work! Aim for high precision!

85
Comparison Write notes and document in the patient’s chart about special modifications or positioning tricks that worked to assist the technologist next time and to improve consistency and precision. e.g. had the patient hold up panniculus during scanning of the hip. or tilted pelvis to better center and straighten spine. Reminders about doing forearm or bilateral hips.

86
Comparison The manufacture’s provided precision error and least significant change (LSC) are unrealistic--calculated under optimal conditions, using ideal patients and experienced expert technologists. Very low error and small LSC. So using their precision error and LSC overestimates change! Which means, we may diagnosis significant change even when there really is not! Affects Rx decisions!
 are unrealistic--calculated under optimal conditions, using ideal patients and experienced expert technologists. Very low error and small LSC. So using their precision error and LSC overestimates change! Which means, we may diagnosis significant change even when there really is not! Affects Rx decisions!")
87
Calculating Precision Error and LSC
Please strongly consider measuring and calculating your site’s precision error and least significant change so you know your precision and what change is significant for your specific site. Must calculate the precision error for lumbar spine and total hip separately.

88
Calculating Precision Error and LSC
Measure both spine and hip on 30 patients twice. e.g. first patient or two of the day over several weeks or every patient until get to 30, extremely low radiation. Measure hip and spine and then it is critical that you get the patient up and off the table completely before rescanning. You do a separate second scan and, as always, try to perform the scan exactly the same way. Best to use real patients, not healthy volunteers so get a good representative sampling. Which one of two measurements to submit to be interpreted? Hopefully they are similar so it doesn’t matter or use the lower of the two. But if one happens to be in a lower diagnostic category (osteoporosis vs. osteopenia), definitely submit the lower of the two.
, definitely submit the lower of the two.")
89
Calculating Precision Error and LSC
Calculate the root mean square standard deviation for the group. Calculate least significant change at 95% confidence interval. ?? No big deal, you loved math in school, right?

90
Calculating Precision Error and LSC
It really is simple, just go to the internet! Precision Calculating Tool or Excel program free at

91
Here’s what the calculating tool looks like, you simply enter in your total hip (or spine) BMD measurements on the left, first and second scan, for thirty patients and the calculator does the rest!
 BMD measurements on the left, first and second scan, for thirty patients and the calculator does the rest!")
92
Calculating Precision Error and LSC
The least significant change (LSC) is calculated separately for spine and total hip. LSC of your site is used to calculate whether the interval change in the patient’s BMD is significant or nonsignificant. e.g. the change in BMD must exceed the least significant change of your facility, otherwise it is simply normal variation in precision.
 is calculated separately for spine and total hip. LSC of your site is used to calculate whether the interval change in the patient’s BMD is significant or nonsignificant. e.g. the change in BMD must exceed the least significant change of your facility, otherwise it is simply normal variation in precision.")
93
Calculating Precision Error and LSC
For example Most recent prior total hip BMD gm/cm² Today’s follow-up total hip BMD gm/cm² Difference (decrease) between two gm/cm² Calculated least significant change (LSC) for our site is gm/cm² or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² change is significant!
 between two gm/cm². Calculated least significant change (LSC) for our site is gm/cm². or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² change is significant!")
94
Calculating Precision Error and LSC
For example Most recent prior total hip BMD gm/cm² Today’s follow-up total hip BMD gm/cm² Difference between two gm/cm² Calculated least significant change (LSC) for our site is 0.022 gm/cm² or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² change is significant!
 for our site is gm/cm². or. expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² change is significant!")
95
Calculating Precision Error and LSC
For example Most recent prior total hip BMD gm/cm² Today’s follow-up total hip BMD gm/cm² Difference between two gm/cm² Calculated least significant change (LSC) for our site is gm/cm² or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² decrease since the prior exam is significant!
 for our site is gm/cm². or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² decrease since the prior exam is significant!")
96
Calculating Precision Error and LSC
For example: Most recent prior total hip BMD gm/cm² Today’s follow-up total hip BMD gm/cm² Difference between two gm/cm² Calculated least significant change (LSC) for our site is gm/cm² or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² change (decrease) is significant! If there is not a significant change, then you are done.
 for our site is gm/cm². or expressed as a percentage x 100 = 2.2% The difference between the 2 studies is greater than the LSC, so the gm/cm² change (decrease) is significant! If there is not a significant change, then you are done.")
97
Calculating Precision Error and LSC
If there is a significant change, then the change can also be reported as percentage change ± LSC. Here you do have to use your math skills. Example: (change in BMD ÷ prior BMD ) x = significant percentage change. Change in BMD Prior BMD x = significant percentage change Then ± LSC expressed as a percentage. 0.034 gm/cm² 0.866 gm/cm² x = % significant decrease since prior exam. or % ± 2.2 %
 x 100 = significant percentage change. Change in BMD. Prior BMD x 100 = significant percentage change. Then ± LSC expressed as a percentage gm/cm² gm/cm² x 100 = 3.9 % significant decrease since prior exam. or 3.9 % ± 2.2 %")
98
Calculating Precision Error and LSC
If there is a significant change, then the change can also be reported as percentage change ± LSC. Here you do have to use your math skills. Example: (change in BMD ÷ prior BMD ) x = significant percentage change. Then ± least significant change expressed as a percentage. For example: 0.034 gm/cm² 0.866 gm/cm² x = % significant decrease since prior exam. or % ± LSC or % ± 2.2%
 x 100 = significant percentage change. Then ± least significant change expressed as a percentage. For example: gm/cm² gm/cm² x 100 = 3.9 % significant decrease since prior exam. or 3.9 % ± LSC or 3.9 % ± 2.2%")
99
Calculating Precision Error and LSC
If there is a significant change, then the change can also be reported as percentage change ± LSC. Here you do have to use your math skills. Example: (change in BMD ÷ prior BMD ) x 100 = significant percentage change. Then ± LSC expressed as a percentage. For example gm/cm² gm/cm² x 100 = 3.9 % significant decrease since prior exam. or 3.9 % ± 2.2 %
 x 100 = significant percentage change. Then ± LSC expressed as a percentage. For example gm/cm² gm/cm² x 100 = 3.9 % significant decrease since prior exam. or 3.9 % ± 2.2 %")
100
Calculating Precision Error and LSC
The minimum acceptable precision for an individual technologist is: Lumbar Spine: 1.9 % LSC = 5.3% Total Hip: 1.8% LSC = 5.0% Femoral Neck: 2.5% LSC = 6.9%

101
DXA References and Sources:
International Society for Clinical Densitometry (ICSD) 2007 Official Positions and Pediatric Official Positions ICSD Bone Densitometry Course for Clinicians 2012 Osteoporosis Essentials: Densitometry, Diagnosis and Management (ISCD and IOF) Bone Densitometry in Clinical Practice: Application and Interpretation 3rd Ed by Sydney Lou Bonnick, MD
 2007 Official Positions and Pediatric Official Positions. ICSD Bone Densitometry Course for Clinicians Osteoporosis Essentials: Densitometry, Diagnosis and Management 2013 (ISCD and IOF) Bone Densitometry in Clinical Practice: Application and Interpretation 3rd Ed by Sydney Lou Bonnick, MD.")
102
FRAX®

103
The FRAX® tool has been developed by WHO to evaluate fracture risk of patients. It is based on individual patient models that integrate the risks associated with clinical risk factors as well as bone mineral density (BMD) at the femoral neck.
 at the femoral neck..")
104
FRAX® can help classify risk especially in osteopenic patients and determine need for treatment.
NOT to be used if patient is already diagnosed as osteoporotic. Not to be used if patient is ALREADY on prescription treatment but Vitamin D or calcium supplements-- okay to use FRAX®.

105
FRAX® 1. Age: used for ages 40-90
2. Race: Caucasian / Black / Hispanic / Asian 3. Gender: Female / Male 4. Weight: kg! 5. Height: cm!

106
6. Previous fracture i.e. previous fracture after age 40 occurring spontaneously, or a fracture arising from trauma which, in a healthy individual, would not have resulted in a fracture (such as a ground level fall.) Do NOT include fractures of the skull, hands and ankles/feet. However, DO include vertebral/spine fractures detected by x-ray alone. Patient may be unaware!

107
FRAX® 7. Mother or father fractured hip: Y or N
8. Current smoking: Y or N

108
FRAX® 9. Glucocorticoids/STEROIDS/prednisone, etc. i.e. currently using oral glucocorticoids/steroids or has been exposed to oral glucocorticoids for more than 3 months at a dose of prednisolone/prednisone of 5 mg daily or more (or equivalent doses of other glucocorticoids): Y or N
: Y or N.")
109
FRAX® 10. Rheumatoid arthritis (confirmed diagnosis): Y or N
: Y or N")
110
FRAX® 11. Secondary Osteoporosis (Answer "yes" if the patient has Type I diabetes (insulin dependent), osteogenesis imperfecta as an adult, untreated long-standing hyperthyroidism, hypogonadism or premature menopause (<45 years old), chronic malnutrition, malabsorption or chronic liver disease)
, osteogenesis imperfecta as an adult, untreated long-standing hyperthyroidism, hypogonadism or premature menopause (<45 years old), chronic malnutrition, malabsorption or chronic liver disease)")
111
FRAX® 12. Alcohol 3 or more units per day (e.g. 1 unit = 1 glass of beer, 1 medium-sized glass of wine, 1 shot/1 oz of liquor): Y or N
: Y or N.")
112
FRAX® REMEMBER: GE LUNAR vs. HOLOGIC AND FEMORAL NECK BMD!!
REMEMBER: North America-->US Database and select proper Race. IF NOT CERTAIN OF AN ANSWER, SELECT "NO."

113
Consider FDA-approved medical therapies in postmenopausal women and men aged 50 years and older, based on the following: A hip or vertebral (clinical or morphometric) fracture T-score ≤ -2.5 at the femoral neck or spine after appropriate evaluation to exclude secondary causes
 fracture. T-score ≤ -2.5 at the femoral neck or spine after appropriate evaluation to exclude secondary causes.")
114
Consider FDA-approved medical therapies in postmenopausal women and men aged 50 years and older, based on the following: Low bone mass (T-score between -1.0 and -2.5 at the femoral neck or spine) and a 10-year probability of a hip fracture ≥ 3% or a 10-year probability of a major osteoporosis-related fracture ≥ 20% based on the US-adapted WHO algorithm Clinicians judgment and/or patient preferences may indicate treatment for people with 10-year fracture probabilities above or below these levels
 and a 10-year probability of a hip fracture ≥ 3% or a 10-year probability of a major osteoporosis-related fracture ≥ 20% based on the US-adapted WHO algorithm. Clinicians judgment and/or patient preferences may indicate treatment for people with 10-year fracture probabilities above or below these levels.")
115
THANK YOU so much for your attention! But wait, there’s more.
BONE DENSITOMETRY THANK YOU so much for your attention! But wait, there’s more.

Similar presentations



 Translate into A Compression Fracture? S.L.>")
, confirmed after.>")
, Fellowship Diabetes/Endocrinology (AKUH), PG Dip Diab (UK) Consultant Endocrinologist.>")


 4.Update on the ESAP In Training Examination (ESAP-ITE) 5.APDEM.>")
>")









 Dr Malith Kumarasinghe MBBS (Colombo)>")
