Download presentation
Presentation is loading. Please wait.

1
The Management of AMI and ACS Patients in the Emergency Department

2
Part 2: AMI/ACS Treatment

3
Acute Myocardial Infraction Part II: Reperfusion Therapies for UA, NSTEMI, and STEMI

4
Edward P. Sloan, MD, MPH, FACEP
Professor Department of Emergency Medicine, University of Illinois at Chicago Chicago, IL

5
Attending Physician Emergency Medicine
University of Illinois Hospital Our Lady of the Resurrection Medical Center

6
Global Objectives Learn more about AMI and ACS
Increase awareness of Rx options Enhance our ED management Improve patient care & outcomes Maximize staff & patient satisfaction Be prepared for the EM board exam

7
Session Objectives Provide AMI, ACS overview
Ask clinically relevant questions

8
AMI/ACS Rx: Global Objectives

9
AMI/ACS Rx: Objectives
What are the global objectives of AMI Rx in the ED?

10
AMI/ACS Rx: Objectives
Maximize coronary dilatation and myocardial O2 delivery Minimize myocardium O2 demand Achieve TIMI-III coronary flow Minimize myocardium damage Minimize chronic LV dysfunction Prevent dysrhythmias, sudden death

11
AMI/ACS Rx: Pharmacological Interventions

12
Pharmacotherapy of AMI/ACS
ASA NTG Morphine Heparin, LMW Thrombolytics Antidysrhythmics Fluid & pressure therapies

13
AMI/ACS Rx: Oxygen AMI/ACS Limited O2 delivery
Increased myocardial O2 use IV, O2, monitor NC at 4 L/min Quick, easy, cheap

14
AMI Rx: ASA, Platelet Meds
When are ASA and other platelet meds indicated?

15
AMI/ACS Rx: Aspirin ISIS 2: as good as streptokinase
Decreased platelet aggregation (Tbx A2) mg ASAP High dose: prostacyclin production decreases, with decreased benefits
 mg ASAP. High dose: prostacyclin production decreases, with decreased benefits.")
16
AMI/ACS Rx: Aspirin All AMI/ACS pts should get ASA
Dose of 162 mg reduces mortality by 23% reinfarction by 49% stroke by 46% 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
17
AMI/ACS Rx: Platelet Rx
Dipyridamole Ticlopidine Clopidogrel Consider when ASA allergic Caution in acute setting!

18
AMI/ACS Rx: Nitrates When are nitrates indicated?
What is the appropriate dose of NTG in AMI/ACS patients?

19
AMI/ACS Rx: Nitrates Coronary dilation Increased collateral flow
Decrease preload, myocardial O2 use SL 1/150, 1/400 Spray, paste, IV SL rarely causes critical hypotension

20
AMI/ACS Rx: Nitrates SL NTG 1/150 400 ucg q 5 minutes
80 ucg per minute Good bioavailability NTG drip: can start at > 10 ucg/min Critical hypotension reversible

21
AMI/ACS Rx: Nitrates Expect SBP to drop with NTG
SBP drop 10% with normal BP SBP drop 30% with elevated BP

22
AMI/ACS Rx: Nitrates Caution with RV infarction!
Reduces preload & LV filling Reduces cardiac output Hypotension can occur Must still maximize O2 delivery Can reduce mortality by 35%

23
AMI/ACS Rx: Morphine What are the indications for morphine in AMI/ACS patients?

24
AMI/ACS Rx: Morphine Provides analgesia
Reduces central sympathetic output May myocardial O2 consumption May mask ongoing ischemia?? Risk/benefit favors use Use with marked pain and anxiety 2-5 mg IVP 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
25
AMI/ACS: Antidysrhythmics
What are the indications for antidysrhythmics in AMI/ACS patients?

26
AMI/ACS Rx: VT, VF Rx VF: Shock at 200j, 300j, 360j, unsynch
VT (Polymorphic, unstable): same VT (Monomorphic, unstable): 100j, synch VT (Monomorphic, stable): Amiodarone: slow IVP Lidocaine: mg/kg bolus injection Procainamide: mg/kg, 20-30/min Synch cardioversion, 50j, 100j
: same. VT (Monomorphic, unstable): 100j, synch. VT (Monomorphic, stable): Amiodarone: slow IVP. Lidocaine: mg/kg bolus injection. Procainamide: mg/kg, 20-30/min. Synch cardioversion, 50j, 100j.")
27
Monomorphic VTach

28
Polymorphic VTach

29
AMI/ACS Rx: AFib Rx Cardioversion: unstable patients
Rapid digitalization IV Beta blockers Diltiazem or verapamil Heparin

30
Atrial Fibrillation

31
AMI/ACS Rx: Adenosine Slow conduction thru AV node
Interrupts reentrant pathways Used in PSVT 6 mg IVP, then 12 mg IVP

32
Paroxysmal SVT

33
AMI/ACS Rx: Amiodarone
Class III agent Treats supraventricular and ventricular dysrhythmias Prolongs refractory period Sustained monomorphic VT VF and unstable VT

34
AMI/ACS Rx: Atropine Sinus brady, poor perfusion, PVCs
Sinus brady, low SBP after NTG Inferior AMI with high grade block Inferior AMI, symptomatic brady N/V after morphine EMD, with epinephrine

35
AMI/ACS Rx: Beta-blockade
What are the indications for beta-blockade in AMI/ACS patients?

36
AMI/ACS Rx: Beta-blockade
Ischemic penumbra preserved Decreased catecholamines Decreased dysrhythmias Decreased HR and BP Decreased infarct size

37
AMI/ACS Rx: Beta-blockade
Consider in all AMI and ACS pts Continued, recurrent ischemic pain Tachyarrhythmias: rapid AFib, Flutter May even be useful in patients with relative contraindications Metoprolol 5mg IV q5mx3 Within 12 hours of presentation

38
AMI/ACS Rx: Beta-blockade
Contraindications Moderate to severe CHF COPD/asthma Bradycardia Hypotension 2nd or 3rd degree A-V blocks

39
AMI/ACS Rx: Beta-blockade
Not consistently achieved in AMI Why do clinicians defer this Rx? May be optimal with HTN, tachycardia With HR < 80, normal BP, less use Not mandated in the ED, prior to PCI

40
AMI/ACS Rx: Ca++ Channel
Rate control in atrial fib, flutter If unable to provide beta blockade Not viewed in same way a use of metoprolol in AMI

41
AMI/ACS Rx: Digitalis Rapid load in rapid atrial fibrillation
Provided before beta blocker use Not used for its inotropic effects

42
AMI/ACS Rx: Lidocaine Limited use New, symptomatic VT
Malignant dysrhythmias, VF 1-1.5 mg/kg, 2-4 mg/min drip Caution in ventricular escape rhythm Can cause asystole No real prophylactic use

43
AMI/ACS Rx: Magnesium 1-2 gram bolus over 5 minutes
Documented Mg deficit with diuretics Prolonged QT, torsade de pointes VT 1-2 gram bolus over 5 minutes Empiric therapy in refractory VF?

44
Torsade de Pointes

45
AMI/ACS: BP/Fluid Rx How should BP and fluids be managed in AMI/ACS patients?

46
AMI/ACS Rx: IV Fluids What are the indications for an acute fluid bolus? When should large volumes of IVF be infused in a hypotensive AMI/ACS patient?

47
AMI/ACS Rx: IV Fluids Normal saline Bolus hypotensive pts
Starling curve supports use 200 cc even with CHF RV AMI: Repeated boluses

48
AMI/ACS Rx: IV Fluids

49
AMI/ACS Rx: Dopamine Dopamine useful in ED Enhanced vital organ flow
Supports nitrates with labile BP Increases HR, SVR, cardiac O2 use Increased inotropy Ischemia, dysrhythmias can occur

50
AMI/ACS Rx: Dobutamine
Dobutamine can also be used in ED Pulmonary edema, LV dysfunction No endogenous norepi release Less myocardial O2 use increase Improved inotropy Improved coronary artery flow Can be used with dopamine

51
AMI/ACS Rx: Norepinephrine
Used in refractory hypotension No response to other pressors Increased myocardial O2 use Improved inotropy, but no increase in cardiac output as SVR is increased Ectopy, dysrhythmias can occur

52
AMI/ACS Rx: Inotropes

53
AMI/ACS Rx: Diuretics Furosemide: NaCl clearance
Used in pulmonary edema & LV dysfunction Volume, Starling effects More optimal LV filling, stroke volume, and cardiac output

54
AMI/ACS Rx: ACE Inhibitors
Reduces LV dilatation and dysfunction, improves remodeling Slows development of CHF AMI/ACS patients, especially critically ill anterior wall MI patients with pulmonary edema show greatest benefit Captopril, enalapril, or lisinopril Early use may reduce mortality

55
AMI/ACS Rx: ACE Inhibitors
Not mandated to be ED Rx Contraindications Hypotension Bilateral renal artery stenosis Renal insufficiency/failure

56
AMI/ACS Rx: Clot Therapies
What are the indications for heparin, IIb/IIIa, and thrombolytic therapy?

57
AMI/ACS Rx: Heparin (LMW)
What are the indications for heparin and LMW heparin in AMI/ACS patients? How does LMW heparin work differently than un-fractionated heparin?

58
AMI/ACS Rx: Heparin (LMW)
Prevents late thrombus formation Maintains patent coronary artery Prevents mural thrombus from forming in anterior wall MI Prevents cerebral emboli with AMI Doesn’t Rx already formed thrombi Platelet Rx: White clot, ACS, NSTEMI Thrombolytic Rx: Red clot, STEMI

59
AMI/ACS Rx: Heparin (LMW)
Thrombin inhibition Prevents clot propagation, formation High embolism risk pts identified: Large or ant MI, Afib, previous embolus, known LV thrombus Complication reduction: Reinfarction reduced by 30% Mortality reduced by 21% 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
60
AMI/ACS Rx: Heparin (LMW)
Indicated in patients with PCI or surgical revascularization Also used in pts who get tPA and those with ACS, NSTEMI

61
AMI/ACS Rx: Heparin Over 1300u/hr associated with bleeding complications Attempt to achieve a PTT that is times normal (60-85 seconds) 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
62
AMI/ACS Rx: Heparin Bolus: 60 units/kg Infusion: 12 U/kg per hour
Max recommended dose 4000 units bolus 1000 units per hour infusion 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
63
AMI/ACS Rx: LMW Heparin
Similar indications to heparin 1 mg/kg SQ BID Prior suggestion that heparin preferred in highest risk pts Some prefer heparin prior to PCI No demonstrated difference between heparin and LMW in these patients 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
64
AMI/ACS Rx: IIb/IIIa Inhibitors
What are the indications for IIb/IIIa inhibitors in AMI/ACS patients? How do these drugs work?

65
AMI/ACS Rx: IIb/IIIa Inhibitors
Abciximab (ReoPro): long acting Ab Eptifibatide (Integrillin): peptide Tirofiban (Aggrastat): peptide Used in ACS, NSTEMI patients, especially those who undergo PCI High risk patients (positive troponin) Requires hrs of infusion to demonstrate benefits 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
: long acting Ab. Eptifibatide (Integrillin): peptide. Tirofiban (Aggrastat): peptide. Used in ACS, NSTEMI patients, especially those who undergo PCI. High risk patients (positive troponin) Requires hrs of infusion to demonstrate benefits. 15% Of seizures result in injury or death. Head contusions and lacerations common. Mortality rates. 1.2% of all seizures. 3 to 26% in SE. Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
66
AMI/ACS Rx: IIb/IIIa Inhibitors
Useful in treatment of pts with refractory unstable angina Treats white clot: ACS, NSTEMI Few head to head studies that compare IIb/IIIa inhibitors Rate of ICH lower than with fibrinolysis

67
AMI/ACS Rx: IIb/IIIa Inhibitors
50,000 receptors per platelet Final common pathway Platelets bind with fibrinogen Forms hemostatic plug (white clot) IIb/IIIa glycoprotein prevents this binding and formation of white clot
 IIb/IIIa glycoprotein prevents this binding and formation of white clot.")
68
Platelet Activation

69
AMI/ACS Rx: IIb/IIIa Inhibitors
Inhibit 80% of receptors, then there is no platelet aggregation Prevents ongoing platelet deposition No effect on thrombin generation No effect on coagulation, inflammation Combo therapy with thrombin drugs Use with heparin is indicated

70
White Clot: ACS, NSTEMI Platelets, Fibrin, Red Cells
Myocardial Ischemia1,2 If unchecked, the clot may completely occlude the coronary artery, or severely limit the flow of blood to the heart. The clot shown above is a mass of platelets, red blood cells, and fibrin mesh, and is capable of preventing blood flow into the microvasculature. If this occurs, the lack of oxygen will result in myocardial ischemia, myocardial necrosis, or even sudden death. Fuster V, et al. N Eng J Med 1992;326: Photos courtesy of Boehringer Ingleheim International GmbH, by Lennart Nilsson.

71
AMI/ACS Rx: IIb/IIIa Inhibitors
Beneficial effects of platelet inhibition Decreased re-occlusion after thrombolysis and/or PCI Decreased re-infarction risk because of better coronary artery healing Minimizes extent of occlusion as a result of acute plaque disruption

72
AMI/ACS Rx: IIb/IIIa Inhibitors
Clinical use in ED is indicated in ACS Actual use is somewhat limited by availability of PCI for most critically ill ACS, NSTEMI patients Although use should begin in ED, many cardiologists begin infusion following PCI Still important prior to transfer for PCI

73
AMI/ACS Rx: Thrombolytics
What are the indications for thrombolytic therapy in AMI/ACS patients? How do thrombolytics work?

74
Red Thrombus in STEMI Thrombin, fibrin, clotting factors

75
AMI/ACS Rx: Thrombolytics
Time is muscle Restoration of TIMI-3 flow Myocardial salvage Reduced ventricular dysfunction Reduced ectopy Sudden death less likley

76
AMI/ACS Rx: Thrombolytics
Indications Classic history EKG with > 1mm ST in 2 limb leads or > 2mm ST in > 2 precordial leads New LBBB 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
77
AMI/ACS Rx: Thrombolytics
No contraindications No cardiogenic shock (??) Presentation within 12 hours of symptom onset 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 Presentation within 12 hours of symptom onset. 15% Of seizures result in injury or death. Head contusions and lacerations common. Mortality rates. 1.2% of all seizures. 3 to 26% in SE. Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
78
AMI/ACS Rx: Thrombolytics
Maximal benefit when given within first 2 hours of infarct Greater mortality benefit in patients with anterior wall AMI as opposed to those with inferior wall AMI 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
79
AMI/ACS Rx: Thrombolytics
Streptokinase APSAC tPA Retavase (rPA) TNK t-PA 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 TNK t-PA. 15% Of seizures result in injury or death. Head contusions and lacerations common. Mortality rates. 1.2% of all seizures. 3 to 26% in SE. Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
80
AMI/ACS Rx: Thrombolytics tPA
Clot specific Not antigenic Reduces mortality 28% ½ life only 5 minutes Higher risk of ICH than SK 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
81
AMI/ACS Rx: Thrombolytics tPA
Dosing: 15 mg IV over 2 min 0.75 mg/kg (max 50) over 30 min 0.50 mg/kg (max 35) over 60 min Start heparin, ASA concurrently 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 over 30 min mg/kg (max 35) over 60 min. Start heparin, ASA concurrently. 15% Of seizures result in injury or death. Head contusions and lacerations common. Mortality rates. 1.2% of all seizures. 3 to 26% in SE. Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
82
AMI/ACS Rx: Thrombolytics Retavase (rPA)
At least as effective as SK Comparable tPA mortality benefit Dosing: 10mg IV bolus at 0 min and 30 min 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
83
AMI/ACS Rx: Thrombolytics TNK t-PA
Genetic variant of tPA Slower plasma clearance Greater fibrin specificity 0.53 mg/kg bolus, 50mg max Heparin infusion, ASA use

84
AMI/ACS Rx: Thrombolytics
Absolute contraindications Any active bleeding Recent GI bleed (within 10 days) Hemorrhagic CVA at any time Non-hemorrhagic CVA in last 6 months 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 Hemorrhagic CVA at any time. Non-hemorrhagic CVA in last 6 months. 15% Of seizures result in injury or death. Head contusions and lacerations common. Mortality rates. 1.2% of all seizures. 3 to 26% in SE. Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
85
AMI/ACS Rx: Thrombolytics
Absolute contraindications Aortic dissection Pericarditis Childbirth within 10 days HTN (SBP >200 or DBP>120) 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 15% Of seizures result in injury or death. Head contusions and lacerations common. Mortality rates. 1.2% of all seizures. 3 to 26% in SE. Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
86
AMI/ACS Rx: Thrombolytics
Absolute contraindications Intracranial/spinal mass lesion, aneurysm, AV malformation Surgery within 2 months Serious head trauma in last month Bleeding disorder Pregnancy

87
AMI/ACS Rx: Thrombolytics
Relative Contraindications Traumatic CPR PUD Current anticoagulant use Hx of HTN with DBP > 100

88
AMI/ACS Rx: Thrombolytics
Relative contraindications Diabetic/hemorrhagic retinopathy Non-compressible vein cannulation Over age 70

89
AMI/ACS Rx: Mechanical Interventions

90
AMI/ACS Rx: Cardiac Pacing
What are the indications for cardiac pacing in AMI/ACS patients?

91
AMI/ACS Rx: Cardiac Pacing
For large anterior STEMIs Not as an Rx for vagal reaction To Rx symptomatic bradycardia Overdrive suppression (+/-)
")
92
AMI/ACS Rx: Cardiac Pacing Transcutaneous Cardiac Pacing
Sinus brady, low BP, no Rx effect Mobitz type II second degree block Third degree block Bifascicular block LBBB RBBB or LBBB & first degree AV block Less so for stable bradycardia, RBBB

93
AMI/ACS Rx: Cardiac Pacing Transvenous Cardiac Pacing
Asystole Sinus brady, low BP, no Rx effect Mobitz type II second degree block Third degree block Bifascicular block RBBB & first degree AV block (+/-) Overdrive suppression for VT (+/-) 3 sec sinus pauses, no Rx effect (+/-)
 Overdrive suppression for VT (+/-) 3 sec sinus pauses, no Rx effect (+/-)")
94
AMI/ACS Rx: Cardiac Pacing Cardiac Pacing Approach
Establish rhythm disturbance Determine that rate, rhythm are effecting adequate perfusion Attempt to Rx BP Attempt to improve rate with atropine Attempt transcutaneous pacing Place sheath for transvenous pacer Insert transvenous pacer as needed

95
AMI/ACS Mechanical Interventions Mechanical Ventilation
Intubation, mechanical ventilation Decreased work of breathing Increases BP (hopefully) Decreases myocardial O2 use Increases O2 delivery (CHF) Critical in cardiogenic shock
 Decreases myocardial O2 use. Increases O2 delivery (CHF) Critical in cardiogenic shock.")
96
AMI/ACS Mechanical Interventions Intraaortic Balloon Pump
What are the indications for intraaortic balloon pump support in AMI/ACS patients? How does the intraaortic balloon pump work?

97
AMI/ACS Mechanical Interventions Intraaortic Balloon Pump
Refractory cardiogenic shock Fluids, pressors without effect Persistent pain, shock Rapid systole balloon deflation Vacuum assists LV function Improves cardiac output

98
AMI/ACS Mechanical Interventions Intraaortic Balloon Pump
Refractory cardiogenic shock As a stabilizing measure prior to PCI Acute mitral regurgitation, VSD (STEMI mechanical complications) Intractable ventricular dysrhythmias Refractory post-MI ischemia, as bridge Unstable pts when LV is “at risk” (+/-)
 Intractable ventricular dysrhythmias. Refractory post-MI ischemia, as bridge. Unstable pts when LV is at risk (+/-)")
99
AMI/ACS Mechanical Interventions Percutaneous Coronary Interventions
What is PCI? What are the PCI indications? What is the goal of PCI? Over what time period should revascularization occur?

100
AMI/ACS Rx: Revascularization
Over what time period should revascularization occur? ACEP and AHA/ACC guidelines 120 minutes door to balloon time If not, consider tPA use in ED

101
AMI/ACS Mechanical Interventions Percutaneous Coronary Interventions
PCI optimal for single lesion, grafts May be able to treat multiple lesions May require multiple procedures Extensive small vessel disease precludes effective PCI Rx Multiple occluded vessels: CABG

102
AMI/ACS Mechanical Interventions Percutaneous Coronary Interventions
PCI is the industry standard Door to balloon time can be > 120 min When PCI is imminent: Front loaded tPA not often utilized IIb/IIIa inhibitors not often utilized Need to optimize ED process

103
AMI/ACS Rx: EMS Triage Is there evidence to support directed triage to “cardiac” centers?

104
AMI/ACS Rx: EMS Triage Is there evidence to support directed triage to “cardiac” centers? No. It is unclear that door to balloon time is significantly decreased, nor is patient outcome worsened if a transfer agreement is in place Caveat: cardiogenic shock patients probably would benefit from direct triage for immediate PCI

105
AMI/ACS Rx: Pre-hospital Rx
What out-of-hospital therapies have been demonstrated to improve outcome in AMI?

106
AMI/ACS Rx: Pre-hospital Rx
911 activation Early defibrillation, first responders 12 lead EKG, thrombolysis (+/-)
")
107
AMI/ACS: Specific Issues
Elderly and females associated with more atypical presentations Pts with symptoms of AMI/ACS after PCI should be assumed to have abrupt vessel closure

108
AMI/ACS: Hospital Admission
Pts at high risk for CAD, AMI, or death admit to ICU ED observation units and non-ICU monitored beds are safe for pts with normal ECGs and low to moderate risk Low risk patients: 2 hour rule out and outpatient stress testing 15% Of seizures result in injury or death Head contusions and lacerations common Mortality rates 1.2% of all seizures 3 to 26% in SE Mortality rate 10 times higher in adults (vs children) SE mortality highest with hypoxic or ischemic insult DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.
 SE mortality highest with hypoxic or ischemic insult. DeLorenzo et al. Neurology 1996;46:1029; J Clin Neurophysiol 1995;12:316; Epilepsia 1992;33(Suppl 4):S15. Hauser. Neurology 1990;40(Suppl 2):9. Kirby and. Sadler. Epilepsia 1995;36:25. Terrence et al. Ann Neurol 1981;9:458.")
109
History Case #1 58 year old male Chest pain, sub-sternal, severe
Onset less than one hour prior Nausea, diaphoresis No known cardiac history Smoker, ?cholesterol

110
Px Case #1 98.8 100/60 110 24 Gen: Screaming in pain, diaphoretic
/ Gen: Screaming in pain, diaphoretic Chest: BS equal CV: Reg rhythm without

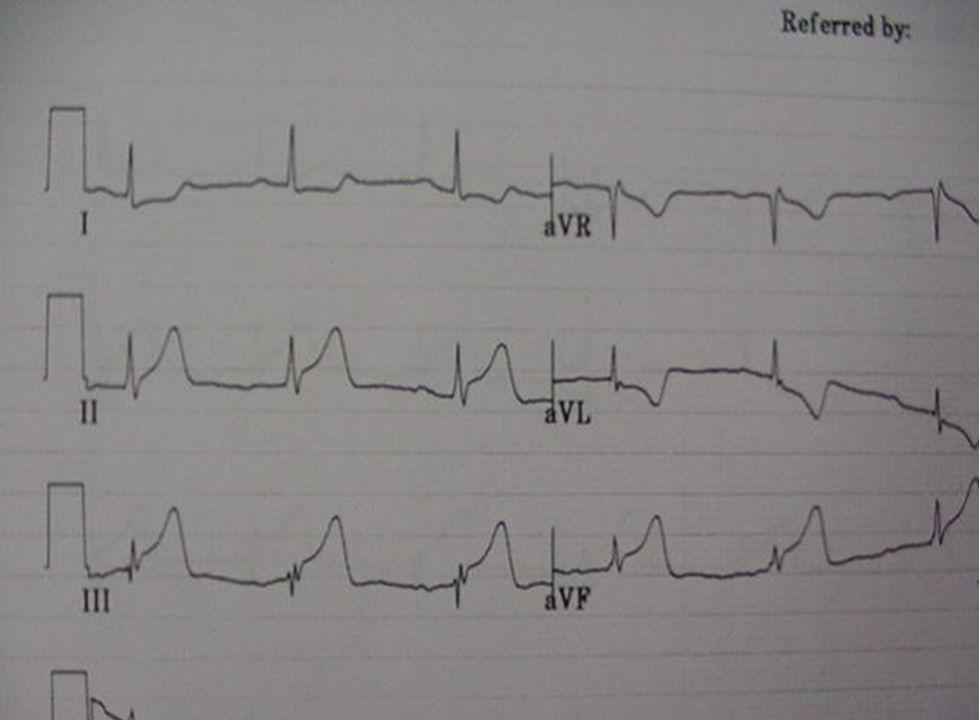
113
Diagnosis Case #1 Having the big one. Acute anterior wall MI Complete occlusion of the left main coronary artery

114
Treatment Case #1 IV NTG ASA, Oxygen Morphine Heparin
Cardioversion (200j) (VTach) Rapid transfer for PTCA
 (VTach) Rapid transfer for PTCA.")
115
History Case #2 48 year old male Sudden onset of chest pain
SOB, nausea ? Cardiac hx, on ASA

116
Px Case #2 98.6 160/90 116 24 Gen: Diaphoretic, pale, anxious
/ Gen: Diaphoretic, pale, anxious Chest: Clear BSBE CV: Reg without Exam otherwise normal

121
Diagnosis Case #2 Inferior wall MI Likely R coronary artery occlusion

122
Treatment Case #2 IV NTG ASA, Oxygen Morphine Heparin
Rapid transfer for PTCA

123
Conclusions AMI/ACS Rx in the E.D.
Common problem ED staff has an important role Many therapies are available Chance to make a difference Good guidelines exist Interested consultants

124
Conclusions AMI/ACS: Relevant Questions
Is there an acute plaque rupture? Is this ACS (white clot) req platelet Rx? Is this STEMI (red clot) req TT, PCI? What Rx must be provided in the ED? How can revascularization best be achieved given the ED processes?
 req platelet Rx Is this STEMI (red clot) req TT, PCI What Rx must be provided in the ED How can revascularization best be achieved given the ED processes")
125
AMI/ACS Diagnosis Questions?
2002, 2004 ACC/AHA guidelines or 2000 ACEP guidelines PDF file allows for optimal printing (312)
")
Similar presentations




















 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")



