Download presentation
Presentation is loading. Please wait.

1
Hypertension What to do when you don’t know what to do! Fiona Stewart Auckland Heart Group Auckland City Hospital 2 nd Sept 2011

2
Essential HypertensionBP < 140/85 Hypertension with Diabetes BP < 130/80 Renal diseaseBP < 130/80 Proteinuria > 1g/dBP < 125/75 Age > 80BP < 150/

3
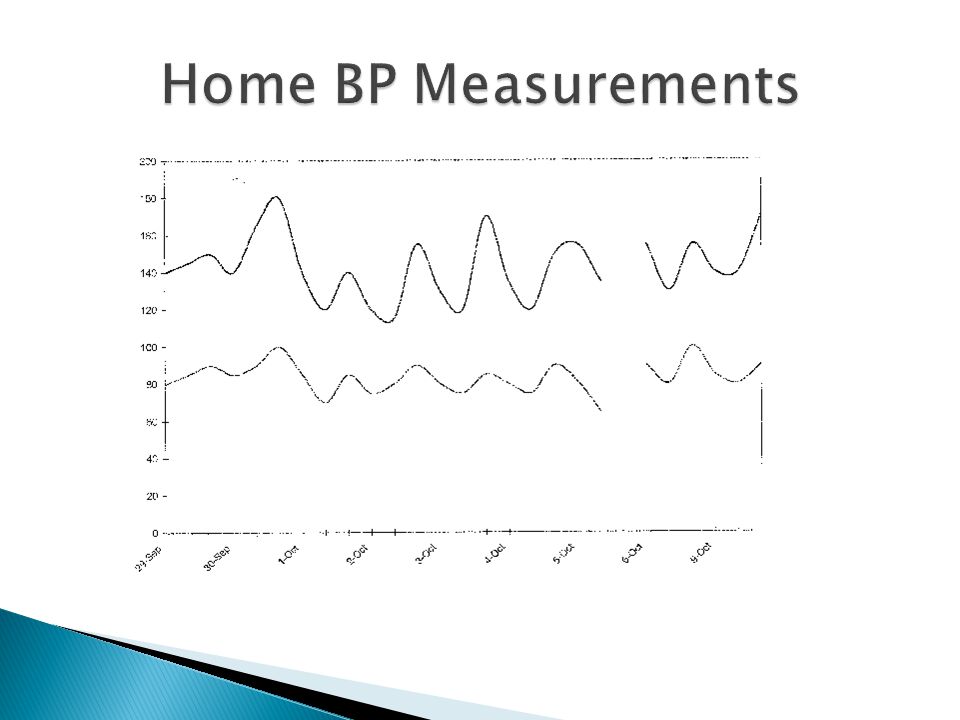
Correct cuff size Sitting x2 at 2 minute intervals Standing BUT in patients with borderline BPs Single recordings are unreliable Multiple clinic recordings correlate poorly with ABU Home BP monitoring is not much better Consider Repeat visit Nurse check (“white coat hypertension”) Home BP monitoring Ambulatory 24hr BP monitoring
 Home BP monitoring Ambulatory 24hr BP monitoring")
6
History ◦ Other illnesses (cardiovascular disease, diabetes, renal disease, gout) ◦ Family history Lifestyle assessment ◦ Smoking, alcohol (max 1-2/d) salt intake, liquorice ingestion, weight, exercise, stress Basic tests ◦ FBC, U + E, urate, creat, eGFR, gluc, lipids, MSU ◦ ECG
 ◦ Family history Lifestyle assessment ◦ Smoking, alcohol (max 1-2/d) salt intake, liquorice ingestion, weight, exercise, stress Basic tests ◦ FBC, U + E, urate, creat, eGFR, gluc, lipids, MSU ◦ ECG")
7
Indication ◦ Abnormal screening tests ◦ Young ◦ BP severe or hard to control Renin, aldosterone, cortisol 24h U metanephrines Renal scan and doppler study Echocardiogram – LVH, ascending aorta

8
Linear increase in risk from BP 115/75 ↑20mmHg SBP or ↑10mmHg DBP doubles mortality from cardiovascular disease BP 120-139/80-89 “prehypertension”

9
Weight Salt intake (including soya sauce) Liquorice ingestion Alcohol Stress Exercise Contributing drugs (NSAIDs)
 Liquorice ingestion Alcohol Stress Exercise Contributing drugs (NSAIDs)")
10
Systolic BP better predictor of adverse cardiovascular events especially in elderly Persistent BP > 140/85 → treat Over 80 years – aim for SBP<150 ◦ Always check standing BP

11
Chlorthalidone 12.5 – 25mg Amlodipine Lisinopril Doxazosin

15
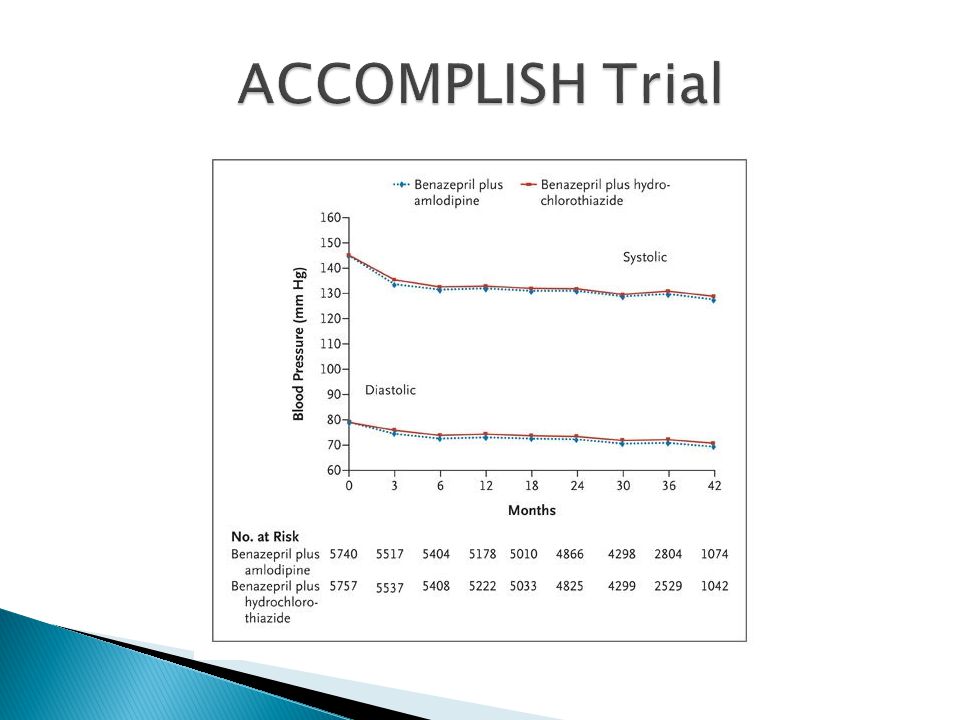
Target BP < 140/90 67% achieved target 2/3 were taking 2+ agents 1/4 were taking 3+ agents Expect to need multiple medications to control BP

17
ACEI + Amlodipine ACEI + Hydrochlorothiazide

20
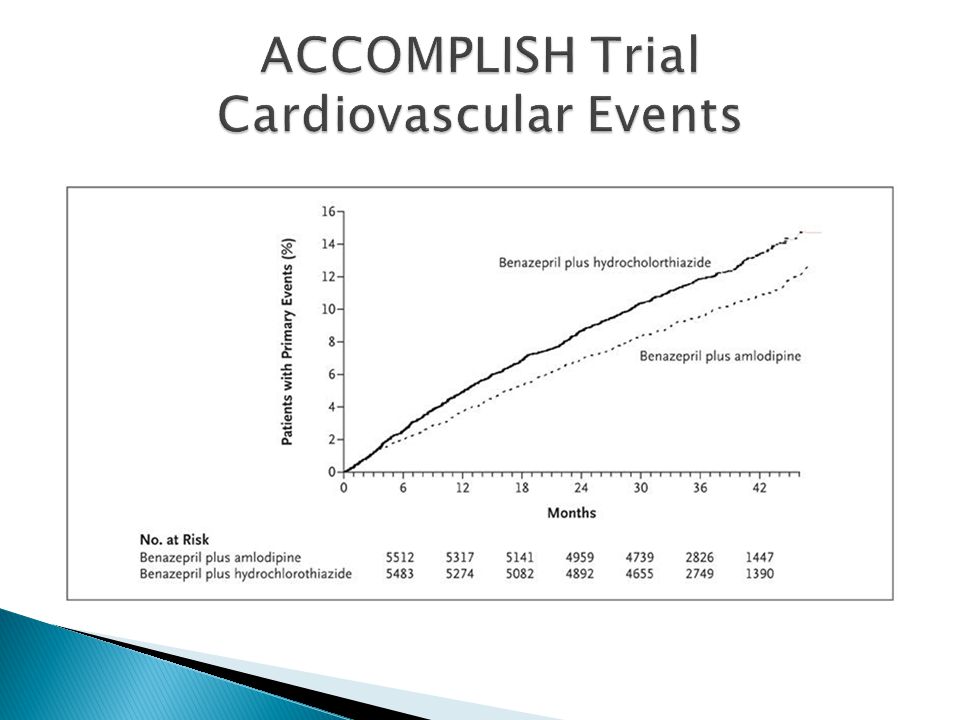
21% Reduction in CV death, MI, CVA over 3 years NNT to prevent one major event = 77 37% were taking > 3 agents

21
Assess comorbidity. Multiple drugs are usually necessary First Line ◦ Thiazides ◦ ACEI/ARB ◦ CCB Second Line -Beta blockers Third Line ◦ Spironolactone ◦ Alpha blockers ◦ Clonidine Fourth Line ◦ Ardian radiofrequency ablation of renal artery Statin

22
Patients aged > 80 SBP >160mmHg, DBP < 110mmHg Indapamide 1.5mg + Perindopril 2-4mg vs placebo Target BP 150/80

23
Blood pressure separation Median follow-up 1.8 years 15 mmHg 6 mmHg

24
All stroke (30% reduction) Placebo IndapamideSR ±perindopril Indapamide SR ±perindopril Placebo P=0.055
 Placebo IndapamideSR ±perindopril Indapamide SR ±perindopril Placebo P=0.055")
25
Total Mortality (21% reduction) Placebo Indapamide SR ±perindopril P=0.019 Placebo IndapamideSR ±perindopril
 Placebo Indapamide SR ±perindopril P=0.019 Placebo IndapamideSR ±perindopril")
26
Fatal Stroke (39% reduction) Indapamide SR ±perindopril Placebo P=0.046 Placebo IndapamideSR ±perindopril
 Indapamide SR ±perindopril Placebo P=0.046 Placebo IndapamideSR ±perindopril")
27
Heart Failure (64% reduction) P<0.0001 Placebo IndapamideSR ±perindopril Placebo IndapamideSR ±perindopril
 P< Placebo IndapamideSR ±perindopril Placebo IndapamideSR ±perindopril")
28
020.50.20.1 HR95% CI 0.70(0.49, 1.01) 0.61(0.38, 0.99) 0.79(0.65, 0.95) 0.81(0.62, 1.06) 0.77(0.60, 1.01) 0.71(0.42, 1.19) 0.36(0.22, 0.58) 0.66(0.53, 0.82) All Stroke Stroke Death All cause mortality NCV/Unknown death CV Death Cardiac Death Heart Failure CV events ITT – Summary
 0.61(0.38, 0.99) 0.79(0.65, 0.95) 0.81(0.62, 1.06) 0.77(0.60, 1.01) 0.71(0.42, 1.19) 0.36(0.22, 0.58) 0.66(0.53, 0.82) All Stroke Stroke Death All cause mortality NCV/Unknown death CV Death Cardiac Death Heart Failure CV events ITT – Summary")
29
Change only one medication at a time Arrange follow up BP measurements (L+S) Check electrolytes with diuretics Escalate early to a second agent Feedback results to the patient
 Check electrolytes with diuretics Escalate early to a second agent Feedback results to the patient")
30
Confirm hypertension with 24hr monitor Check for secondary causes ◦ Renal scan ? Renal artery stenosis ◦ Cortisol, renin, aldosterone, metanephrines Lifestyle adjustments – stress, salt Compliance Optimal medication dose and frequency

31
Thiazides ◦ Chlorthalidone more effective than HCZ ACEI ◦ Cilazapril and lisinopril – daily dose ◦ Enalapril and quinapril – bd dose Angiotensin II Blockers ◦ Titrate dose to 32mg candesartan, 100mg losartan CCBs ◦ Amlodipine and felodipine 10mg

32
Measurement ◦ Sitting ◦ DBP 4 th Korotkoff sound DBP <90mmHg from conception to 20/40 is strongly correlated with lower rates of pre-eclampsia ACEI and ARB are contraindicated from 6 weeks gestation. ACEI are safe with breast feeding. Metoprolol, oxprenolol and labetalol are associated with a better fetal outcome than other beta-blockers Methydopa has a long record of safety in pregnancy CCBs are well tolerated in pregnancy

33
Hypertrophy Arrhythmia Oxygen Consumption Vasoconstriction Atherosclerosis Insulin Resistance The kidney as origin of sympathetic drive carried centrally via renal afferent sympathetic nerves generating central sympathetic drive Renal Afferent Nerves ↑ Renin Release RAAS activation ↑ Sodium Retention ↓ Renal Blood Flow ↑ Renin Release RAAS activation ↑ Sodium Retention ↓ Renal Blood Flow Sleep Disturbances Renal Efferent Nerves

34
Radiofrequency energy can ablate the renal sympathetic nerves

35
First-in-man, non-randomized 45 patients with resistant HTN (SBP ≥160 mmHg on ≥3 anti-HTN drugs, including a diuretic) Expanded cohort of patients (n=153) 24-month follow-up Lancet. 2009;373:1275 35 Symplicity HTN-1

36
Significant, Sustained BP Reduction BP change (mmHg) 36
 36")
37
Primary Endpoint: 6-Month Office BP ∆ from Baseline to 6 Months (mmHg) 33/11 mmHg difference between RDN and Control (p<0.0001) 84% of RDN patients had ≥ 10 mmHg reduction in SBP 10% of RDN patients had no reduction in SBP 37 Systolic Diastolic SystolicDiastolic Symplicity HTN-2 Investigators. Lancet. 2010;376:1903.

38
Changes in Glucose Tolerance at 3 Months after Renal Denervation Mahfoud et al. European Society of Cardiology. 2010.

Similar presentations