Download presentation
Presentation is loading. Please wait.

1
THE AUTONOMIC NERVOUS SYSTEM
PHARMACOLOGY THE AUTONOMIC NERVOUS SYSTEM

2
WHAT IS THE AUTONOMIC NERVOUS SYSTEM?
RECAP WHAT IS THE AUTONOMIC NERVOUS SYSTEM?

3
AUTONOMIC NERVOUS SYSTEM
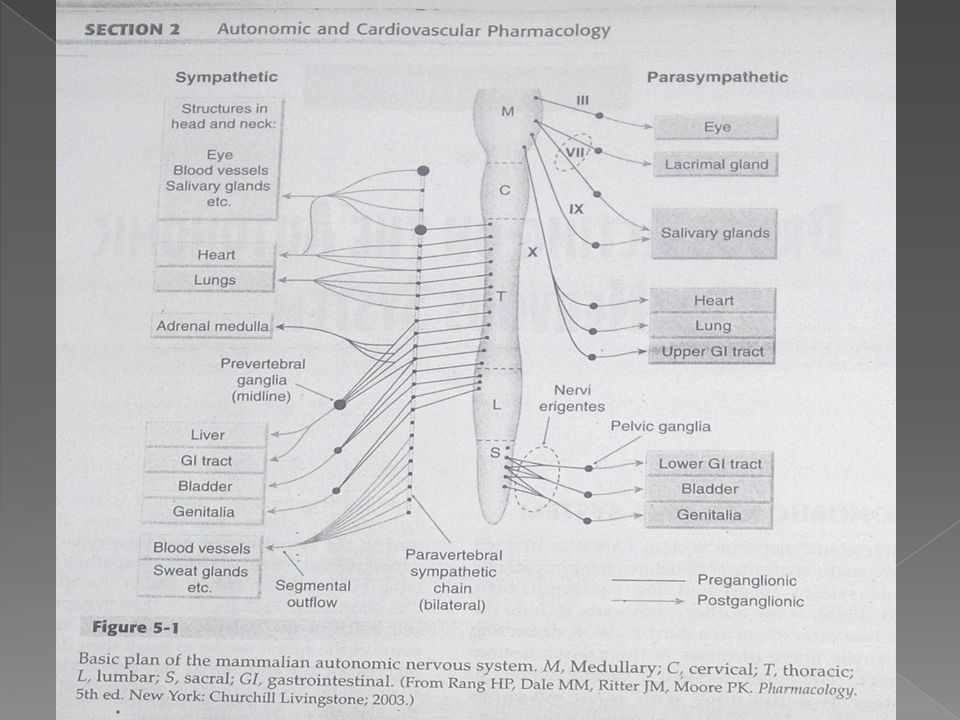
The autonomic nervous system (ANS) is divided into two main anatomical divisions, the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). The ANS is responsible for many involuntary functions such as contraction and relaxation of smooth muscles, exocrine and some endocrine secretions, heart rate and contractility, blood pressure and digestion. The enteric system is closely aligned to the other two divisions with interconnections between them.
 is divided into two main anatomical divisions, the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). The ANS is responsible for many involuntary functions such as contraction and relaxation of smooth muscles, exocrine and some endocrine secretions, heart rate and contractility, blood pressure and digestion. The enteric system is closely aligned to the other two divisions with interconnections between them.")
4
ANATOMY & PHYSIOLOGY OF THE ANS
The most significant anatomical difference between the ANS and the somatic system is that the ANS requires two neurons in sequence, whereas the somatic system uses a single motor neuron to relay information from the CNS to the skeletal muscles. The two neurons comprising the autonomic pathway are known as the preganglionic and postganglionic neurons. The preganglionic sympathetic fibers originate with their cell bodies in the lateral born of the gray matter of the thoracic and lumbar segments (from T1 to L12). In the SNS the preganglionic neuron is long, extending to the glands and viscera, but the opposite is true for the PNS. The preganglionic fibers originate in the cranial area of the spinal cord and travel a long distance to synapse in ganglia on or near their effector organs. The postganglionic fibers for the PNS are rather sort compared with the postganglionic fibers for the SNS.
. In the SNS the preganglionic neuron is long, extending to the glands and viscera, but the opposite is true for the PNS. The preganglionic fibers originate in the cranial area of the spinal cord and travel a long distance to synapse in ganglia on or near their effector organs. The postganglionic fibers for the PNS are rather sort compared with the postganglionic fibers for the SNS.")
5
The adrenal medulla is a part of the SNS but provides an exception to the two-neuron rule. It receives preganglionic fibers but lacks postganglionic neurons. Instead, it influences the target organs by secreting epinephrine, also known as adrenaline, directly into the blood.

7
NEUROTRANSMITTERS FOR THE ANS
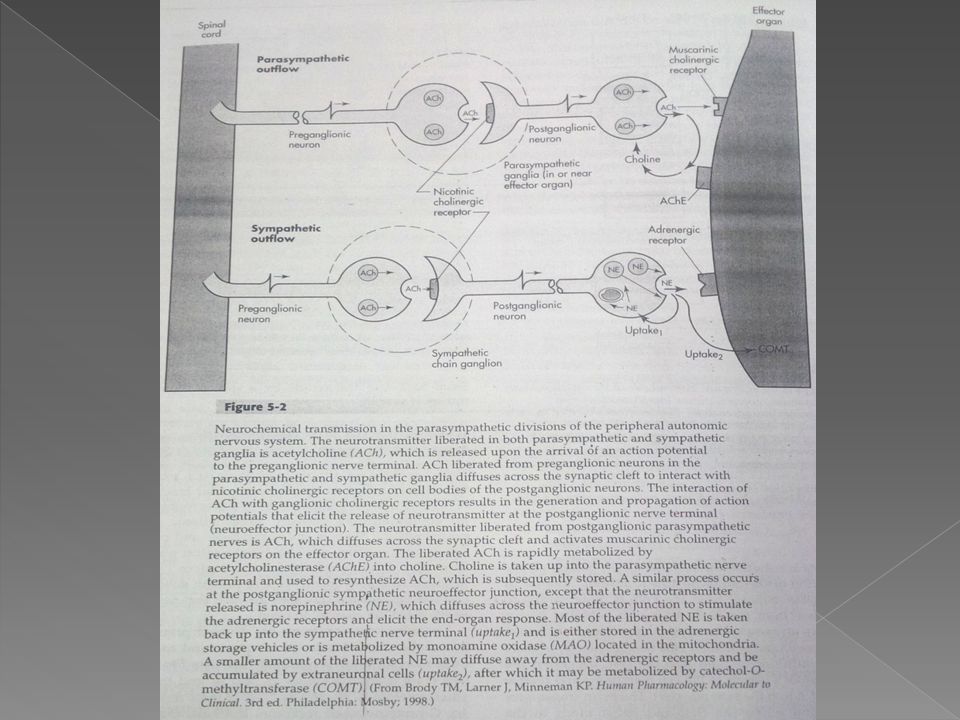
The preganglionic neurotransmitter for both the sympathetic and parasympathetic systems is acetylcholine (ACh). When releases, Ach binds to nicotinic receptors on the postganglionic cell. However, the neurotransmitter for the postganglionic neuron for each system is different.
. When releases, Ach binds to nicotinic receptors on the postganglionic cell. However, the neurotransmitter for the postganglionic neuron for each system is different.")
9
RECEPTORS FOR THE ANS There are three main types of nicotinic ACh receptors: those located on the neuromuscular junction of the skeletal muscle ganglionic receptors responsible for communication between preganglionic and postganglionic fibers of the sympathetic and parasympathetic systems CNS-type receptors widely dispersed throughout the neural system. All nicotinic receptors consist of five protein subunits and contain two binding sites for ACh that need to be filled for the channel to open. The adrenergic receptors are divided primarily into alpha (α) and beta (β) receptors, and each of these receptor types is subdivided further. All of these receptors are G-protein-linked receptors but have different second messengers.
 and beta (β) receptors, and each of these receptor types is subdivided further. All of these receptors are G-protein-linked receptors but have different second messengers.")
10
α1 α2 β1, β2 & β3 D1 D2 SUB RECEPTOR TYPES SECOND MESSENGERS
Receptors increase phospholipase C, which stimulates the release of intracellular calcium. These receptors function to produce constriction of blood vessels and bronchi and to relax the GI tract and the genitourinary tract α2 Receptors decrease cyclic adenosine monophosphate formation and inhibit calcium release, which reduces sympathetic activity by acting as an auto receptor β1, β2 & β3 Receptors stimulate cyclic adenosine monophosphate formation and produce increases in cardiac rate and contractility, bronchodilation, and lipolysis. D1 Receptors are located on renal vascular smooth muscles and mediate vasodilation of the renal artery. D2 Receptors are found on presynaptic nerve terminals.

11
FUNCTIONS OF THE ANS & SPECIFIC INNERVATIONS
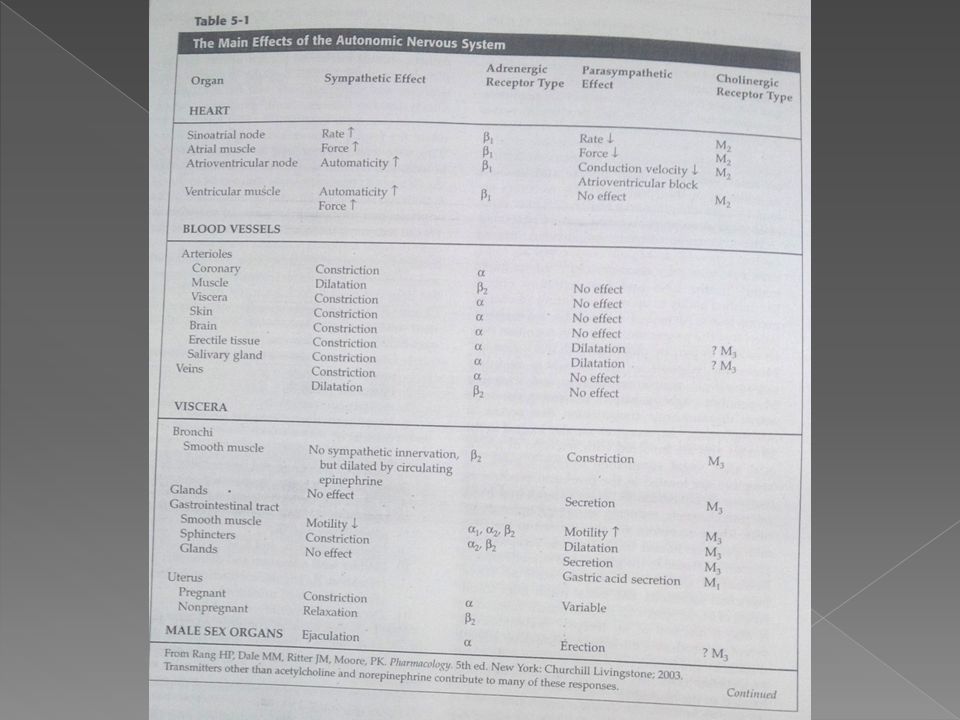
The SNS mediates a fight or flight response, and the PNS tends to place the body in a more calm state. The SNS response is triggered by direct sympathetic stimulation of the effector organs and by stimulation of the adrenal medulla to release epinephrine and norepinephrine into the circulation. This system functions as a “unit” producing a set of reactions that occur together. The SNS functions to dilute the pupils, increase heart rate and contractility, raise serum glucose level for energy, dilute the bronchioles, increase skeletal blood flow, and relax the GI and GU tracts. Some specific innervations and their receptors associated with the sympathetic system include the following:

12
THE EYES Ciliary epithelium produces aqueous humor through 1 receptors. This fluid keeps the anterior chamber of the eye at the proper pressure to focus light onto the lens and to the retina. Sympathetic activity stimulates the alpha receptors on the iris to contract longitudinally to pull the iris towards itself, concentrically opening the sphincter. The ciliary muscle and sphincter are stimulated by parasympathetic neurons releasing acetylcholine (Ach), binding muscarinic (M) receptors. These muscles work by: a) ciliary muscle pulls on the trabecular meshwork to open the canal of schlemm and drain the fluid. b) ciliary muscle contracts the entire machinery to accommodate lens by relaxing its pull on the lens. c) The sphincter contracts to constrict the pupil. So under high stress, sympathetics release NE. NE (, ) increases aqueous humor production, and dilates the pupil. Once the stress is gone, the parasympathetics constrict the pupil and drain the anterior chamber.
, binding muscarinic (M) receptors. These muscles work by: a) ciliary muscle pulls on the trabecular meshwork to open the canal of schlemm. and drain the fluid. b) ciliary muscle contracts the entire machinery to accommodate lens by relaxing its pull on the lens. c) The sphincter contracts to constrict the pupil. So under high stress, sympathetics release NE. NE (, ) increases aqueous humor production, and dilates the pupil. Once the stress is gone, the parasympathetics constrict the pupil and drain the anterior chamber.")
13
THE LUNGS Sympathetic activity- 2 receptor stimulation bronchodilates the airways and decreases airway secretions Parasympathetic activity- Ach stimulates M receptors, bronchoconstrict the airways and also to incrrease airway secrretions In the lungs there are many other receptors and mediators affecting lung function, but these are not directly involved in the SNS/PNS system.

14
THE HEART 1. Sympathetic activity- 1 receptor stimulation increases heart rate, contractility, AV nodal conduction and cardiac output. 2. Parasympathetic activity- muscarinic (M) receptor stimulation decreases SA nodal firing, decrease AV node conduction and decrease CO.
 receptor stimulation decreases SA nodal firing, decrease AV node conduction and decrease CO.")
15
BLOOD VESSELS The blood vessels express , , dopamine (DA), histamine and M receptors. Sympathetic- NE (, 1), and epinephrine(1, 2, 1, 2) and dopamine (DA) are released: 1 vasoconstricts vessels, mainly at the arterioles, to increase pressure/ cut off blood flow to unnecessary organs and shunt it to organs that need it. 2 vasodilates skeletal vessel beds to increase blood flow to needed muscles. Also lowers vascular resistance overall, and therefore blood pressure.
, and epinephrine(1, 2, 1, 2) and dopamine (DA) are released: 1 vasoconstricts vessels, mainly at the arterioles, to increase pressure/ cut off blood flow to unnecessary organs and shunt it to organs that need it. 2 vasodilates skeletal vessel beds to increase blood flow to needed muscles. Also lowers vascular resistance overall, and therefore blood pressure.")
16
BLOOD VESSELS DA- three different mechanisms, concentration-dependent.
a.) Low dose DA- dilates renal artery, increasing kidney perfusion. b.) Mid-dose DA- stimulates 2 receptors as well, resulting in dilation of skeletal bed BV’s to decrease systemic resistance. c.) High Dose DA- stimulate 1 receptors and blood vessels constrict, resulting in an overall increased blood pressure (At all three doses, low medium or high, the renal artery is dilated to increase perfusion of the kidney.)
 Low dose DA- dilates renal artery, increasing kidney perfusion. b.) Mid-dose DA- stimulates 2 receptors as well, resulting in dilation of skeletal bed BV’s to decrease systemic resistance. c.) High Dose DA- stimulate 1 receptors and blood vessels constrict, resulting in an overall increased blood pressure. (At all three doses, low medium or high, the renal artery is dilated to increase perfusion of the kidney.)")
17
GASTRO INTESTINAL TRACT
Parasympathetic activity (M) stimulates GI motility, allows sphincters to open, and increase secretions. Sympathetic activity (, ) slows GI motility, increases sphincter tone, and decreases GI secretions. DA receptor activation causes increased GI motility, stimulates secretion, and decreases sphincter tone. Opioids- also must be considered in the GI function, as opioids will promptly decrease GI motility, decrease secretions and increase sphincter tone, inducing constipation.s
 stimulates GI motility, allows sphincters to open, and increase secretions. Sympathetic activity (, ) slows GI motility, increases sphincter tone, and decreases GI secretions. DA receptor activation causes increased GI motility, stimulates secretion, and decreases sphincter tone. Opioids- also must be considered in the GI function, as opioids will promptly decrease GI motility, decrease secretions and increase sphincter tone, inducing constipation.s.")
18
BLADDER 1. Sympathetic: The receptors prevent bladder contraction by relaxing the bladder, and contracting the internal sphincter. 2. Parasympathetic: Muscarinic receptors in the bladder stimulate bladder contraction and relax the internal sphincter. (Micturition Reflex)
")
21
ENTERIC NERVOUS SYSTEM
The ENS controls exocrine and endocrine functions of the GI tract and motility, microcirculation, and immune and inflammatory processes. It can function independently from the CNS, although it maintains connections to the brain via the SNS and PNS. It contains two major plexuses: The myenteric plexus – innervates the two muscle layers of the entire gut and the secretory portion of the mucosa with extensions to the gallbladder and pancreas The submucosa plexus in the small intestine – innervates the muscularis blood vessels. A similar plexus is also found in the gallbladder, pancreas, cystic duct, and common bile duct.

22
The neurotransmitters involved in the ENS were originally thought to include only ACh and serotonin. However, adenosine triphosphate, γ-aminobutyric acid, substance P, vasoactive intestinal polypeptide, nitric oxide and a variety of other peptides are and have been seen to be active in this system. Problems with the ENS have been implicated in a number of GI disorders. Severe vomiting with chemotherapy has been linked to excessive serotonin release by damaged mucosal enterochromaffin cells. High levels of serotonin activate receptors on the vagal primary afferents that extend to the vomiting center in the brainstem. Defective enteric neurons can cause a slowing of intestinal propulsion, leading to bowel obstruction.

23
DRUGS THAT MIMIC THE PNS
Drugs that affect the PNS are divided into two categories those that are directly on the cholinergic (muscarinic) receptors and those that act indirectly by inhibiting the enzyne AChE. AChE rapidly hydrolyzes ACh in the synpatic cleft by cleaving ACh to acetate and choline. Inhibitors of AChE stimulate cholinergic action by prolonging the lifetime of Ach.
 receptors and those that act indirectly by inhibiting the enzyne AChE. AChE rapidly hydrolyzes ACh in the synpatic cleft by cleaving ACh to acetate and choline. Inhibitors of AChE stimulate cholinergic action by prolonging the lifetime of Ach.")
24
CLINICAL APPLICATIONS FOR MUSCARINIC AGONISTS
Drugs that mimic the actions of the PNS are used: to reduce intraocular pressure in glaucoma to increase the motility of the GI tract in paralytic ileus to increase tone of the detrusor muscle for the treatment of urinary retention to improve cognition in Alzheimer’s disease. EFFECTS ON THE EYE Parasympathetic input to the eye contracts both the constrictor pupillae and the ciliary muscles. Constricts of this muscle allows the lens to accommodate for near vision. Aqueous humor is normally secreted slowly and continuously from ciliary body. The fluid drains through the canal of Schlemm. However, in acute glucoma, the canal of Schlemm becomes blocked by a dilated pupil, and the fluid cannot drain. The intraocular pressure is raised, which damages the eye and

25
can lead to blindness. Pupil constriction under these circumstances can improve drainage by moving the pupil away from the pathway for aqueous humor allowing the fluid to drain into the canal. EFFECTS ON MYASTHENIA GRAVIS Myasthenia gravis is an autoimmune disorder caused by antibodies specific for nicotinic ACh receptor at the neuromuscular junction. Patients demonstrate muscle weakness and easy fatigability, being unable to sustain muscular contractions. Areas of involvement may include the eyelids, extraocular muscles, extremities, diaphragm and neck extensor muscles. EFFECTS ON THE NEUROMUSCULAR FUNCTION In addition to improving strength in some neuromuscular junction disorders, muscarinic agonists can be used to reverse muscle paralysis during surgical procedures blocking the neuromuscular junction is often used along with anesthesia in delicate procedures in which movement is contraindicated. Drugs that inhibit AChE can be used to terminate the action of these neuromuscular blockers. They may also be used to reverse an anticholinergic overdose.

26
DIRECT-ACTING MUSCARINIC AGONIST
Direct-acting agonists bind directly to the muscarinic receptors, functioning just like ACh, to mimic the actions of the PNS. Pilocarpine is applied topically to the cornea to produce miosis in acute glaucoma. The duration of action is 24hours. It is also used for the treatment of xerostomia (dry mouth) in Sjögren's Syndrome and after radiation therapy for head and neck cancers. Bethanechols stimulates the PNS with a particular selectivity for the detrusor muscle in the bladder and smooth muscles of the GI tract. It is to treat urinary retention or to reduce urethral resistance in detrusor-trigone dyssynergia. It is particularly useful for postpartum or postoperative urine retention. It may also be used in the treatment of reflux esophagitis. With the oral formation, onset of action is within 30-90mins and duration of action may last up to 6 hours.
 in Sjögren s Syndrome and after radiation therapy for head and neck cancers. Bethanechols stimulates the PNS with a particular selectivity for the detrusor muscle in the bladder and smooth muscles of the GI tract. It is to treat urinary retention or to reduce urethral resistance in detrusor-trigone dyssynergia. It is particularly useful for postpartum or postoperative urine retention. It may also be used in the treatment of reflux esophagitis. With the oral formation, onset of action is within 30-90mins and duration of action may last up to 6 hours.")
27
INDIRECT-ACTING MUSCARINIC STIMULANTS
Indirect-acting muscarinic stimulants act by inhibiting AChE to prolong the action of ACh. There are actually two types of cholinesterases that are seen in the body, AChE and butyrylcholinesterase. Both of these enzymes produce a very rapid breakdown of Ach. The drugs appear to inhibit both forms of the enzyme with equal potency. In general, the indirect-acting agents both fall into three categories: Short-acting anticholinesterases: e.g. Edrophonium is used to help diagnose myasthenia gravis Medium-duration anticholinesterase: e.g. Neostigmine and pyridostigmine – pyridostigmine is a treatment of choice for patients with mild myasthenia gravis because it has greater bioavailability and a half-life of 4 hours.

28
Irreversible anticholinesterase/organophosphate compounds: these are agents that have been developed into war gases (sarin) and insecticide (malathion). These bind to AChE irreversibly, producing weakness and sensory loss. These agents are higly lipid soluble and are rapidly absorbed through the mucous membranes and even through intact skin. Because these compounds are absorbed rapidly through the cuticles of insects, they are used in agriculture.

29
THERAPEUTIC CONCERNS WITH DIRECT-ACTING & INDIRECT-ACTINGMUSCARINIC AGENTS
Direct-acting and indirect-acting muscarinic agents can produce significant cardiovascular effects, including bradycardia and decreased cardiac output. The reduction of cardiac output results from a decrease in contractility, particularly in the atria, cause by relative denseness of the muscarinic receptors in this area. Another adverse effect that may occur is generalised vasodilation, producing a marked decrease in blood pressure. Nitric oxide and endothelial-derived relaxing factor mediate this effect. Smooth muscle in the lungs and the GI tract are also affected by excess mascarinic activity. This produces abdominal pain, diarrhea, vomiting, frequent urination, bronchoconstriction, and increased secretions.

34
MUSCRINIC ANTAGONISTS
Drugs that block the muscrinic receptors are often labeled as parasympatholytic because they block the action of the parasympathetic nerve activity. They all function as competitive anatongists of ACh. CLINICAL APPLICATION FOR ANTIMUSCARINIC (ANTICHOLINERGIC) DRUGS Antimuscarinic drugs are used to treat motion sickness, relieve symptoms of Parkinson’s disease, dilate pupils for an ocular exam, reduce motility of the GI and GU tracts, and dilate the airways. Because they reduce secretion, they are used preoperatively to prevent excessive salivation and reduce bronchiole tract secretions associated with anesthesia.
 DRUGS. Antimuscarinic drugs are used to treat motion sickness, relieve symptoms of Parkinson’s disease, dilate pupils for an ocular exam, reduce motility of the GI and GU tracts, and dilate the airways. Because they reduce secretion, they are used preoperatively to prevent excessive salivation and reduce bronchiole tract secretions associated with anesthesia.")
35
ANTICHOLINERGIC DRUGS
Atropine is the prototypic anticholinergic agent. It is both the a central and a peripheral cholinergic antagonist, although it appears to have little effect at the nicotinic receptor sites, so the autonomic ganglia are not usually affected unless high dosages are given. Atropine is primarily used to produce mydriasis in the eye for an ocular exam and as an adjunct for anesthesia to reduce respiratory secretions. Scopolamine is another anticholinergic drug that has a similar effect to that of atropine but produces greater CNS depressions causing drowsiness, memory loss and sleep. Its primary use is to prevent motion sickness and vertigo caused by depression of vestibular function. Synthetic anticholinergics such as dicyclomine and glycopyrrolate, have been formulates to act more selectively in the GI tract and thus have been used for the treatment of irritable bowel syndrome. Ipratropium is an inhaled anticholinergic agent, available alone or in combination with albuterol, for the treatment of bronchospasm related to asthma and other chronic obstructive lung diseases. Dry mouth and pharyngeal irriation are the major compliants with ipratropium, but it can also increase intraocular pressure in patients with glaucome.

36
THERAPEUTIC CONCERNS WITH ANTICHOLINERGIC DRUGS
At low doses, atropine affects the salivary glands, producing dry mouth; larger doses block accommodation of the eyes, causing blurred vision. Vagal effects become blocked as the drug level increases, producing tachycardia and diminished bronchial secretions and sweating. Parasympathetic tone to the gut and the urinary tract is blocked, producing constipation and urinary retention. Most patients seen in rehabilitation will not be receiving anticholinergic drugs, at least not on a long term basis. However, most patients complain about sedation and fatigue, which reducees exercise capacity. Two other concerns include increased heart rate and the inability to cool oneself. Vital sign, including the patients temperature, should be monitored frequently particularly if there is a history of cardiac issues.

37
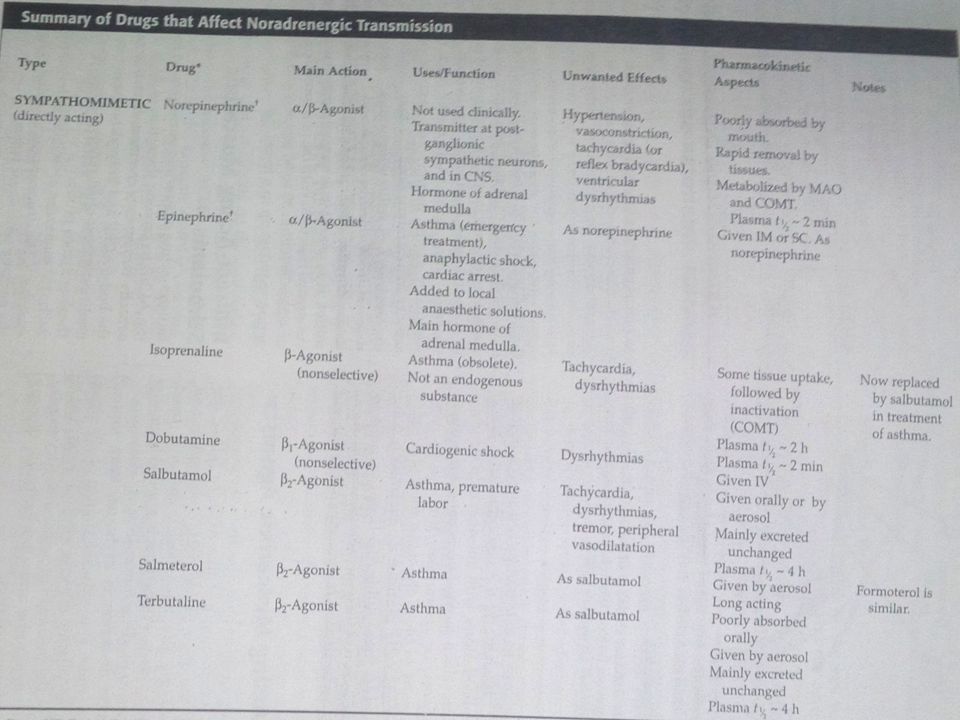
DRUGS AFFECTING THE SNS (ADRENERGIC)
Drugs that mimic the SNS are labeled sympathomimetic. They are designed to either facilitate norepinephrine and epinephrine release or to activate the adrenergic receptors. Specifically, sympathomimetic drugs constrict arterioles to reduce bleeding, slow diffusion of local anesthetics, decongest mucous membranes and raise blood pressure in shock and hypotensive states.

38
PHARMACOLOGIC EFFECTS OF CATECHOLAMINES
CARDIAC EFFECTS: catecholamines produce a significant increase in myocardial contractility and a significant increase in heart rate. The increase in contractility results from an increase in calcium influx into cardiac fibers. The increase in heart rate is produces by increasing the rate of membrane depolarization in sinus node. Catecholamines also hastens cardiac conduction. VASCULAR EFFECTS: with these drugs vary because the net effect depends on the dosage given. At lose doses, epinephrine with decrease peripheral vascular resistance via β2 receptor-mediated dilation of skeletal muscle blood vessels. At higher doses, α1 receptor influence balances the β2 receptor influence, and at even higher doses, α1 receptor influence predominates, producing vasoconstriction and hypertension.

39
CNS EFFECTS: the natural catecholamines are relatively polar, and therefore they do not enter the CNS easily. However, in larger doses they are still capable of producing anxiety, tremors and headaches. The noncatecholamine adrenergic agonists such as phenylephrine, ephedrine and amphetamine have greater lipid solubility and produce more CNS effects. NONVASCULAR SMOOTH MUSCLE EFFECTS: catecholamines are capable of relaxing the smooth muscles of the GI tract, reducing the strength of intestinal peristalsis. In the bladder, epinephrine will cause urinary retention by trigone sphincter constriction and detrusor relaxation. In the lungs, bronchial smooth muscle dilates in response to catecholamines acting on β2 receptors. EFFECTS ON NERVE TERMINALS: α2 receptors are present presynaptically on cholinergic and adrenergic nerve terminals. These are autoreceptors that act to inhibit neurotransmitter release. Clinically, they have primarily been used to reduce sympathetic outflow as a treatment for hypertension but are also being used as analgesics and for reducing spasticity.

40
METABOLIC EFFECTS: epinephrine acts to increase blood glucose and fatty acid level to supply the needed energy for activity. Insulin secretion is inhibited, and glycogenolysis and gluconeogenesis are enhanced.

41
THE CARDIOVASCULAR SYSTEM
PHARMACOLOGY THE CARDIOVASCULAR SYSTEM

42
WHAT IS THE CARDIOVASCLAR SYSTEM?
RECAP WHAT IS THE CARDIOVASCLAR SYSTEM?

43
THE CARDIOVASCULAR SYSTEM
The system that circulates blood and lymph through the body, consisting of the heart, blood vessels, blood, lymph, and the lymphatic vessels and glands.

44
CARDIAC BLOOD FLOW The mammalian heart is a double pump in which the right side operates as a low-pressure system delivering de-oxygenated blood to the lungs, while the left side is a high pressure system delivering oxygenated blood to the rest of the body. The walls of the right ventricle are much thinner than those of the left, because the work load is lower for the right side of the heart. The ventricular muscle is relatively stiff, and it would take some time to fill with venous blood during diastole. The thin, flexible atria serve to buffer the incoming venous supply, and their initial contraction at the beginning of each cardiac cycle fills the ventricles efficiently in a short space of time

45
PHAMACOLOGY AND THE CARDIOVASCULAR SYSTEM
Antihypertensive Drugs

46
HYPERTENSION Hypertension is the leading causes of cardiovascular mortality and morbidity AKA high blood pressure, it is a common condition in which the force of the blood against your artery walls is high enough that it may eventually cause health problems. Some people may have dull headaches, dizzy spells or a few more nosebleeds than normal, these signs and symptoms usually don't occur until high blood pressure has reached a severe or life-threatening stage.

47
HYPERTENSION There are many pharmacological ways of controlling high blood pressure: Control through baro- and chemoreceptors Vascuar endothelium and intermediate control Renin- angiotensin system and long term control Classification of blood pressure Normal BP Prehypertension Stage 1 hypertension Hypertension

48
Nondrug treatment for hypertension is always the first choice and includes exercise, weight reduction, no smoking and restriction to salt intake and alcohol consumption. However if all previous attempts fail, the major categories of drugs that may be used to reduce blood pressure are diuretics, sympatholytic, direct acting vasodilators, calcium antagonists and renin-angiotensin inhibitors.

49
DIURETICS mainly cause increased sodium and water leaving kidney. There are three types Loop Diuretics- inhibit Na+/ K+ / 2Cl- co-transporter on the luminal membrane of the ascending loop of Henle, blocking reabsorption of these electrolytes from the tubular fluid. When the transporter is blocked the luminal fluid stays hypertonic facilitating water loss, hence leaving a high concentration of Na in the lumen which facilitates the loss of H and K which interns exchange with the Na in the distal portion of the nephron. Thiazide Diuretics- are the major diuretics for lowering blood pressure. These drugs inhibit Na+/Cl- co-transporter on the luminal membrane of the distal convoluted tubule and proximal collecting duct. Less Na+ intracellularly enhances the Na+/Ca2+ pump located on the basolateral cell membrane, facilitating calcium reabsorption. These drugs also enhance K+ excretion in the collecting duct. These drugs then promote Na+ and K+ excretion and reabsorption of Ca2+. Potassium-Sparing Diuretics- act in the collecting duct to inhibit Na+ reabsorption and K+ excretion. The Na+ channel in the principal cell depolarizes the cell, creating a positive charge the repels K+. Some of the K+-sparing agents block this depolarization so K+ is not excreted into the tubular fluid.

50
THERAPEUTIC CONCERNS FOR DIURETICS
They produce fluid depletion, which may lead to dehydration. If the K level is too low or too high it can trigger arrhythmia. They produce hyperglycemia and abnormally affected lipids. May cause frequent urination. May cause muscle weakness or cramping.

51
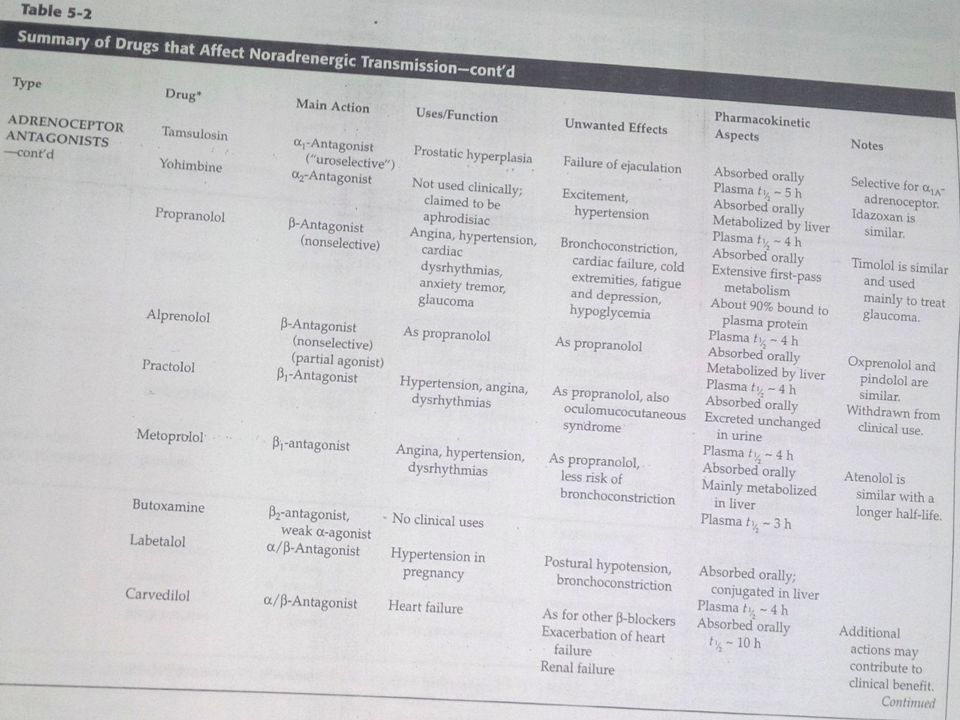
HYPERTENSION β Adrenoceptor Blockers- reduce heart rate and contractility, resulting in a reduction of cardiac output and blood pressure. β-Blockers are either selective or nonselective for β adrenoceptors. The nonselective antagonists will block β1 and β2 adrenoceptors. Propranolol is the prototypic non selective agent. The selective agents will block β1 receptors only, but this selectivity is only at high doses. Atenolol and metoprolol are selective β1 adrenoceptors. The main difference between them is that the nonselective agents will block the β2 receptors in the bronchioles and the β2 receptors in the skeletal muscle vasculature. α Adrenoceptor Blockers- decreases vascular resistance. Vascular resistance is the resistance to flow that must be overcome to push blood through the circulatory system. Prazosin, terazosin and doxazosin are selective α1–blockers primarily used to lower peripheral vascular resistance, thus lowering blood pressure. Dual α- and β-Blockers- are helpful to patients who experience increased peripheral resistance while taking pure β-blockers. Labetalol and carvedilol are nonselective α1- and β1- receptor antagonists.

52
HYPERTENSION Central Acting α2 –agonists- Clonidine is the prototypic α2 adrenoceptor antagonist primarily used to reduce blood pressure. Its action is particularly directed at the vasomotor centre in the brain. This leads to a reduction of arteriole tone, and with long-term use, a reduction in heart rate and cardiac output. Adverse effects include: dry mouth, orthostatic hypotension, impotence and galactorrhea.

53
Therapeutic concerns with α- and β-Blockers
Vasoconstriction Bronchoconstriction Bradycardia Depression, sexual dysfunction α- Postural hypotension Nasal stuffiness Angina α- and β- Adverse effects are similar to α-blockers and β-blockers

54
VASODILATORS Direct Vasodilators - hydralazine, minoxidil, nitro-prusside, and fenoldopam and the calcium channel blockers. Direct Vasodilators- dilate arterioles by acting directly on the vascular smooth muscles. Concerns: myocardial infarction, reflex tachycardia, nausea and sweating. Calcium Channel Blockers- block calcium influx into arterial smooth muscle, producing vasodilation and a decrease in peripheral resistance. There are three classes of calcium channel blockers. Dihyropyridines- include nifedipine, nicardipine and amlodipine. They reduce arteriole tone with less effect on the heart. Diphenyl alkylamine verapamil- primarily affects the heart Benzodiazepine diltiazem- affects both vasculature and the heart. Concerns: throbbing headach, dizziness, flushing, tremor and bradycardia

55
ACE INHIBITORS AND ACE RECEPTOR BLOCKERS
An ace inhibitor blocks the action of ACE, reducing angiotensin II synthesis. Angiotensin II contributes to the development of hypertension by constricting arterioles and stimulating aldosterone release ACE inhibitors are especially useful for patients with congestive heart failure because they do not suppress cardiac function

56
ACE receptor blockers interfere with the binding of angiotensin II to the angiotensin receptors. They are very effective at reducing blood pressure without producing a cough Similar to the ACE inhibitors they have been shown to be renal protective, delaying the development of diabetic nephropathy in patients with type II diabetes

57
THERAPEUTIC CONCERNS WITH ACE INHIBITORS AND ACE RECEPTOR BLOCKERS
Common side effects of ACE inhibitors include dry cough, rashes, hypotension and hyperkalemia The side effects of ARBs are similar to that of ACE inhibitors an includes angiodema

58
Cardiac Arrhythmia Abnormal rhythms of the heart that cause the heart to pump less effectively Arrhythmia occurs: – when the heart’s natural pacemaker develops an abnormal rate or rhythm – when the normal conduction path is interrupted – when another part of the heart takes over as pacemaker

59
THERAPEUTIC DRUGS FOR CARDIAC ARRYTHMIA
Class I - Sodium channel blockers - Block Na+ entry during depolarization phase Class II - β-blockers: For tachycardia – Propranolol Class III - Potassium channel blockers: Prolong repolarization phase by blocking outward potassium flux Class IV - Calcium channel blockers: Prolong repolarization phase by blocking inward calcium current

60
REFERENCES Pharmacology for Physical therapists, Barbara Gladison
Concise Pharmacology for Physiotherapy Students, Ebook, Dr. J. G. Buch

Similar presentations






 – brain and spinal cord. Peripheral Nervous System (PNS) – afferent and efferent.>")


 AUTONOMIC NERVOUS SYSTEM PHARMACOLOGY.>")







 - Brain and spinal cord n n Peripheral Nervous.>")


 Sensory.>")

