Download presentation
Presentation is loading. Please wait.

2
Anaphylaxis in the E.D. Emergency Medicine Grand Rounds May 20, 2004 Bruce MacLeod Stu Turner

3
Objectives To examine local experience with anaphylaxis and hymenoptera sting. To review the evidence for management of anaphylaxis and hymenoptera sting: Pharmacological therapy Immunotherapy Attention to biphasic reactions To review related conditions such as exercise induced anaphylaxis and angioedema.

4
Anaphylaxis No universally accepted definition exists Canadian Pediatric Surveillance Program “a severe allergic reaction to any stimulus, having sudden onset and generally lasting less than 24 hours, involving one or more body systems and producing one or more symptoms such as hives, flushing, itching, angioedema, stridor, wheezing, shortness of breath, vomiting, diarrhea, or shock” Other definitions require more than one body system involved.

5
Anaphylaxis Clinical Features Symptom onset generally in less than 1 hour.

6
Anaphylaxis Clinical Features Cutaneous Urticaria, angioedema, flushing, pruritus Respiratory Tachypnea, hoarseness, laryngeal edema, bronchospasm, dyspnea Cardiovascular Tachycardia, hypotension, angina, arrhythmia Gastrointestinal Dysphagia, heartburn, abdominal cramps, diarrhea, nausea, emesis Other Conjunctivitis, rhinitis, dizziness, headache

7
Anaphylaxis Shock Organs Guinea Pig Bronchial smooth muscle constriction Death by bronchospasm Rabbits Pulmonary artery vasoconstriction Death by right ventricular failure Dog Hepatic venoconstriction Severe hepatic congestion

8
Anaphylaxis Human Shock Organs Cardiovascular H1 Receptors Coronary artery vasoconstriction Generalized vascular permeability H2 Receptors Atrial and ventricular contractile forces Atrial Rate Coronary artery vasodilatation

9
Anaphylaxis Cardiovascular Effects Primary Cardiac Myocardial Depression Decreased Coronary Blood Flow, Ischemia, Plaque disruption Atrial and Ventricular Arrhythmias Vascular Permeability 50% of intravascular fluid can third space within 10 minutes

10
Anaphylaxis Respiratory Effects Upper Airway Laryngeal Edema Observed in 60% of fatalities (post mortem finding) Lower Airway Bronchial Obstruction Bronchospasm and Bronchiolar edema Observed in 50% of fatalities (post mortem finding)
 Lower Airway Bronchial Obstruction Bronchospasm and Bronchiolar edema Observed in 50% of fatalities (post mortem finding)")
11
Human Anaphylaxis Mortality Cause of Death Respiratory Obstruction, Cardiovascular Collapse or Both. Risk factors for death (weakly predictive) Immediacy of onset History of Asthma Delay in Epinephrine Administration
 Immediacy of onset History of Asthma Delay in Epinephrine Administration.")
12
Fatal Human Anaphylaxis Pathological Findings Pumphrey R, Roberts I:Postmortem findings after fatal anaphylactic reactions. J Clin Pathol 53:273-6,2000 Reviewed 56 of the 130 reported cases in the United Kingdom 1992 – 1998 19 insect stings 16 food reactions 21 drugs and radiocontrast media Death in < 60 minutes in 39/56 Pathology findings Mucus plugging and hyperinflated lungs – 15/56 Petechial hemorrhages – 10/56 Pharyngeal/laryngeal edema – 23/56 Nothing to Indicate Allergic Response – 23/56 Attributed to sudden death from shock

13
Prevalence of Anaphylaxis

14
Hypothesized USA Annual Mortality by Anaphylaxis

15
Alberta Fatalities Due to Anaphylaxis 1984-2004 Total = 11

16
Emergency Department Experience Brown A, McKinnon D, Chu K:Emergency department anaphylaxis A review of 142 patients in a single year. J All and Clin Imunol,108:861-6,2001 62,000 visit per year Emergency Department in Australia 142 anaphylaxis visits (1998-99) 60 coded as severe anaphylaxis BP 25, Laryngeal edema, Hypoxemia Outcomes 1 death 33% discharged 61% admitted to Observation unit then discharged 3% ward admission 3% ICU admission
 60 coded as severe anaphylaxis BP 25, Laryngeal edema, Hypoxemia Outcomes 1 death 33% discharged 61% admitted to Observation unit then discharged 3% ward admission 3% ICU admission.")
17
Emergency Department Experience Brown A, McKinnon D, Chu K:Emergency department anaphylaxis A review of 142 patients in a single year. J All and Clin Imunol,108:861-6,2001 Symptoms in all patients Cutaneous-94% Symptoms in those with severe anaphylaxis Dizziness/syncope-35% Laryngeal edema-25% Hypotension (<90)-21% Causative Agent Identified73% Drugs 28% (antibiotics 17, NSAIDS 10,ACE inhibitors 6, IV contrast 4) Insect 17% Food 17% (seafood 13, nuts 4, mango 3, other 3)
-21% Causative Agent Identified73% Drugs 28% (antibiotics 17, NSAIDS 10,ACE inhibitors 6, IV contrast 4) Insect 17% Food 17% (seafood 13, nuts 4, mango 3, other 3).")
18
Anaphylaxis Experience Foothills Emergency 2003

19
Angioedema Foothills Emergency 2003 Total = 30

20
Admission Rates Anaphylaxis 4 of 72 Admitted 2 intubated Latex Idiopathic 1 Scoped and normal ? Psychogenic 1 Ward Admit Chinese food Angioedema 1 of 30 Admitted ACE Inhibitor then bit tongue Fiberoptic Intubation and I and D for Ludwig's Angina required

21
Allergist Referral Rate Anaphylaxis 15 of 72 3 hymenoptera 2 foods 1 medication 1 latex 1 exercise induced 7 idiopathic Angioedema 12 of 30 1 identified C1 esterase deficiency

22
Hymenoptera Experience Foothills Hospital - 2003

23
FMC Experience with Hymenoptera Sting Dec 2002-Nov 2003

24
Discharge Recommendations Hymenoptera Sting

25
Infection With Local Reactions Hymenoptera Stings

26
HYMENOPTERA BEES, WASPS and FIRE ANTS

27
OBJECTIVES 1. IDENTIFICATION 1. IDENTIFICATION 2. STING REACTIONS: 2. STING REACTIONS: VENOM VENOM TYPES TYPES TREATMENT TREATMENT PITFALLS IN TREATMENT PITFALLS IN TREATMENT IMMUNOTHERAPY IMMUNOTHERAPY

29
HYMENOPTERA APOIDEAVESPOIDEAFORMICIDEA

30
APOIDEA APIDAE APIS HONEYBEES BOMBUS BUMBLEBEES SPHECIDIAE DIGGER WASPS

31
HONEYBEE

32
HONEY BEE

33
BUMBLEBEE

34
BUMBLE BEE

35
VESPOIDEA VESPIDAE VESPA HORNETS VESPULA YELLOW JACKETS POLISTES WASPS EUMENINAE MUD WASPS

36
WESTERN YELLOW JACKET

37
YELLOW JACKET

38
BALD FACED HORNET

39
HORNET

40
HORNET

41
GIANT HORNET

42
PAPER WASP

43
POLISTE WASP

46
WASP

47
CICADAKILLER WASP

48
WASP

49
POTTER WASP

50
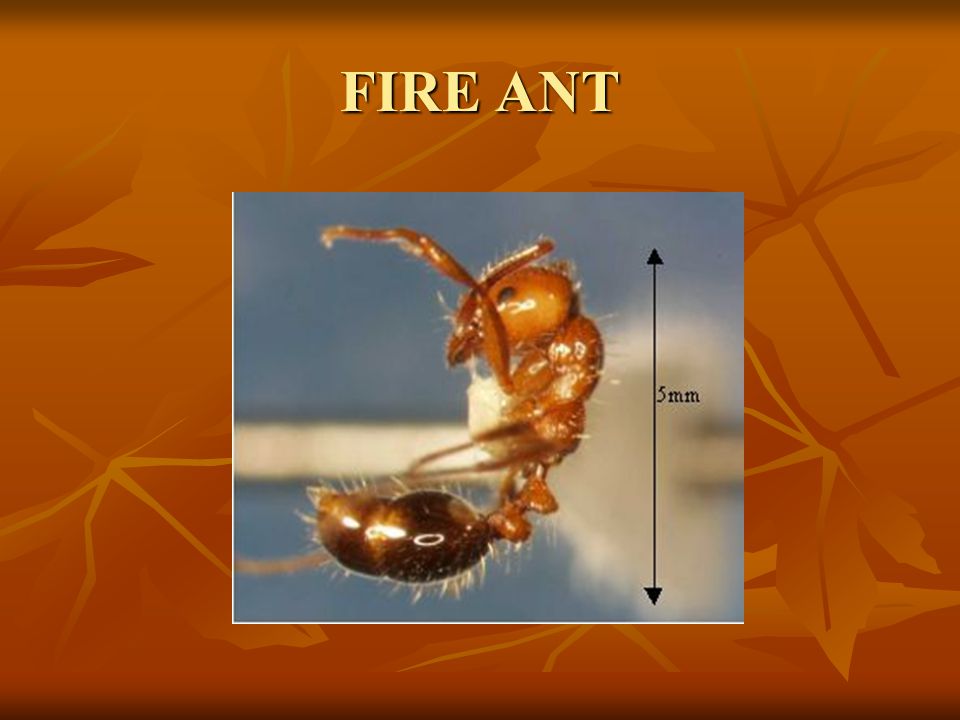
FORMICIDEA FORMICIDAE MYRIMICINAE FIRE ANTS HARVESTER ANTS

51
FIRE ANT

53
BEE STINGING

54
STINGERS

55
Venoms 1. Proteins – make up most of the dry weight 1. Proteins – make up most of the dry weight 2. Carbohydrates, peptides, amino acids, lipids, other low-molecular-weight substances 2. Carbohydrates, peptides, amino acids, lipids, other low-molecular-weight substances 3. Enzymes - phospholipase A, B - hyaluronidase 3. Enzymes - phospholipase A, B - hyaluronidase - acid phosphatase - acid phosphatase

56
Venoms -Toxicity Majority of the toxicity due to LMW substances: Majority of the toxicity due to LMW substances: kinins kinins acetylcholine acetylcholine dopamine dopamine histamine histamine Serotonin Serotonin Antigenic substances: induce hypersensitivity Antigenic substances: induce hypersensitivity

57
Signs and Symptoms of a Sting Vary depending on: Vary depending on: Site Site Species of insect Species of insect Number of stings: pheromone attraction Number of stings: pheromone attraction Size of victim Size of victim Previous health of victim Previous health of victim Previous sensitization Previous sensitization

58
STING REACTIONS USUAL USUAL LARGE LOCAL LARGE LOCAL ANAPHYLACTIC ANAPHYLACTIC TOXIC TOXIC

59
Signs and Symptoms: Usual/Large Local Immediate Pain and Burning Immediate Pain and Burning Local Swelling –can be large and extensive Local Swelling –can be large and extensive Erythema Erythema Itching Itching Fire ant: biphasic Fire ant: biphasic * May persist or increase up to 2-3 days * * May persist or increase up to 2-3 days * * May last for several days* * May last for several days*

60
USUAL REACTION

61
LARGE LOCAL REACTION

62
FIRE ANT STING

64
Signs and Symptoms: Anaphylactic Less than.5-1.5% of all stings IgE mediated Most serious within first 30 minutes Mild (urticaria,angioedema) to life threatening * some have no previous history of systemic reactions or even past stings * * some have no previous history of systemic reactions or even past stings *
 to life threatening * some have no previous history of systemic reactions or even past stings * * some have no previous history of systemic reactions or even past stings *")
65
Allergic Reactions Yellow Jacket – most common Yellow Jacket – most common Followed by the Bee Followed by the Bee Wasp Wasp Hornet Hornet

66
Signs and Symptoms: Toxic and Unusual Reactions Nausea, vomiting, diarrhea – large amounts venom Nausea, vomiting, diarrhea – large amounts venom Delayed hypersensitivity: 7-10 days Delayed hypersensitivity: 7-10 days Acute glomerulonephritis Acute glomerulonephritis Serum Sickness – multiple stings Serum Sickness – multiple stings Guillain-Barre Guillain-Barre Neuritis Neuritis Encephalopathy Encephalopathy Purpura: Thrombocytopenia, H-S Purpura: Thrombocytopenia, H-S Cardiac: MI, dysrhythmias Cardiac: MI, dysrhythmias *Can occur several days to a week after and can be progressive over long periods of time* *Can occur several days to a week after and can be progressive over long periods of time* Non-IgE mediated Non-IgE mediated

67
Incidence of Systemic Reaction.4 - 4% incidence systemic reactions:.4 - 4% incidence systemic reactions: 30-40% with history of atopic disease 30-40% with history of atopic disease 2:1 males to females 2:1 males to females 17% incidence of large local reactions 17% incidence of large local reactions Up to 5% on to systemic reaction Up to 5% on to systemic reaction Deaths: rare, usually adults Deaths: rare, usually adults

68
Subsequent Reactions Studies have found anywhere between 9.0%and 40% of children with a history of dermal anaphylaxis had a systemic reaction with a subsequent sting, and none of those reactions were more severe than the initial reaction. Studies have found anywhere between 9.0%and 40% of children with a history of dermal anaphylaxis had a systemic reaction with a subsequent sting, and none of those reactions were more severe than the initial reaction. Most were milder than the reaction to the first sting Most were milder than the reaction to the first sting

69
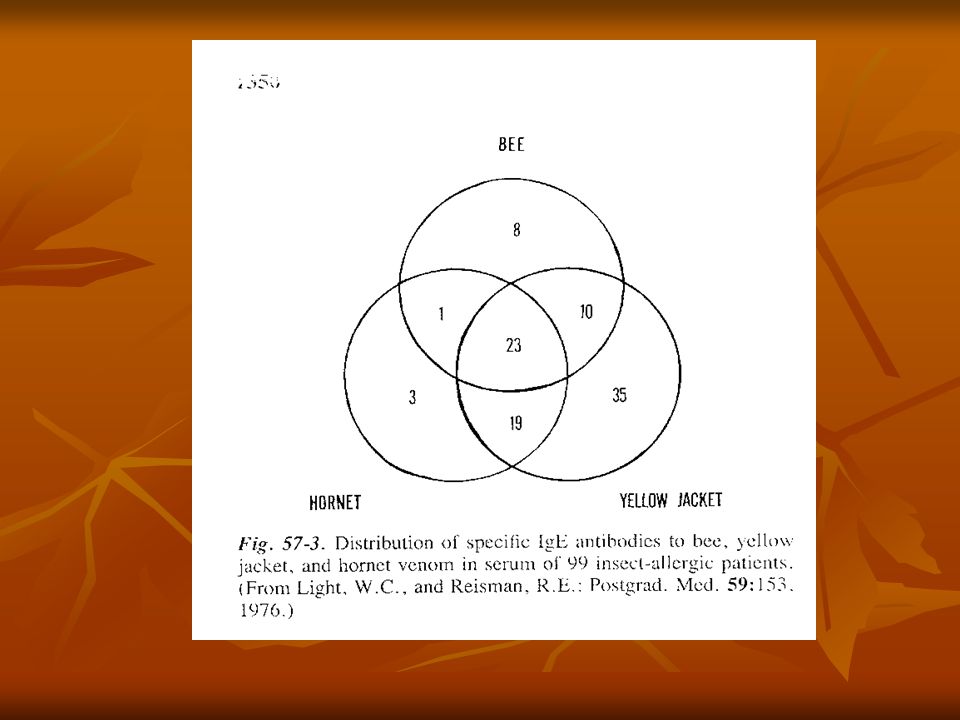
Cross-sensitivity Within the Hymenoptera Within the Hymenoptera Hornets and Yellow jackets (Vespids)- extensive Hornets and Yellow jackets (Vespids)- extensive Wasps and other Vespids - limited Wasps and other Vespids - limited Bees (Apoidea) and Vespids – limited Bees (Apoidea) and Vespids – limited Within the vespid family and within the different species of: Within the vespid family and within the different species of: Yellow jacket (Vespula) – cross-reacting antigens in larger quantities of venom Yellow jacket (Vespula) – cross-reacting antigens in larger quantities of venom Hornet (Vespula) Hornet (Vespula) Wasp (Polistes) – more limited cross-sensitivity Wasp (Polistes) – more limited cross-sensitivity
- extensive Hornets and Yellow jackets (Vespids)- extensive Wasps and other Vespids - limited Wasps and other Vespids - limited Bees (Apoidea) and Vespids – limited Bees (Apoidea) and Vespids – limited Within the vespid family and within the different species of: Within the vespid family and within the different species of: Yellow jacket (Vespula) – cross-reacting antigens in larger quantities of venom Yellow jacket (Vespula) – cross-reacting antigens in larger quantities of venom Hornet (Vespula) Hornet (Vespula) Wasp (Polistes) – more limited cross-sensitivity Wasp (Polistes) – more limited cross-sensitivity")
71
Treatment Local: Local: Inspect for venom apparatus (bees) and remove (scrape) Inspect for venom apparatus (bees) and remove (scrape) Cleanse wound with water and soap Cleanse wound with water and soap Ice – most only need this Ice – most only need this Oral antihistamine: diphenhydramine or hydroxyzine Oral antihistamine: diphenhydramine or hydroxyzine Baking soda paste Baking soda paste Steroids for extremely large and painful reactions Steroids for extremely large and painful reactions Systemic: Systemic: Adrenaline Adrenaline IV diphenhydramine IV diphenhydramine Steroids Steroids Inhaled B2 agonists Inhaled B2 agonists
 and remove (scrape) Inspect for venom apparatus (bees) and remove (scrape) Cleanse wound with water and soap Cleanse wound with water and soap Ice – most only need this Ice – most only need this Oral antihistamine: diphenhydramine or hydroxyzine Oral antihistamine: diphenhydramine or hydroxyzine Baking soda paste Baking soda paste Steroids for extremely large and painful reactions Steroids for extremely large and painful reactions Systemic: Systemic: Adrenaline Adrenaline IV diphenhydramine IV diphenhydramine Steroids Steroids Inhaled B2 agonists Inhaled B2 agonists")
72
REMOVAL BEE STINGER

73
Treatment Epi-pen Epi-pen Medic Alert bracelet Medic Alert bracelet

74
Pitfalls in Treatment Treating as cellulitis – mimics Treating as cellulitis – mimics Infection very rare in immunocompetent hosts Infection very rare in immunocompetent hosts Antibacterial properties of insect venom Antibacterial properties of insect venom Think of the pathophysiology of a sting Think of the pathophysiology of a sting Not prescribing an Epi-pen Not prescribing an Epi-pen Not referring to an allergist for consideration of immunotherapy Not referring to an allergist for consideration of immunotherapy Compartment Syndrome – beware: large local Compartment Syndrome – beware: large local

75
Multiple Stings Large dose of venom being delivered to the victim Large dose of venom being delivered to the victim Recruiting pheromone is secreted eliciting further attacks from nearby bees Recruiting pheromone is secreted eliciting further attacks from nearby bees Mass stings can cause hemolysis, rhabdomyolysis, and thrombocytopenia. Mass stings can cause hemolysis, rhabdomyolysis, and thrombocytopenia. Deaths usually result from renal failure or cardiac arrest. Deaths usually result from renal failure or cardiac arrest. Renal failure and death may result from 20 to 200 wasp stings or 150 to 1,000 bee stings Renal failure and death may result from 20 to 200 wasp stings or 150 to 1,000 bee stings

76
Immunotherapy - desensitization Whole insect body extracts: not effective and not recommended. Lack detectable venom content. Whole insect body extracts: not effective and not recommended. Lack detectable venom content. Venom immunotherapy to produce venom specific IgG Venom immunotherapy to produce venom specific IgG Some people develop substantial IgG titers in response to a single sting reaction Some people develop substantial IgG titers in response to a single sting reaction Venom immunotherapy may reduce the risk of a systemic reaction after a subsequent sting from 60% in untreated patients to less than 3%. Venom immunotherapy may reduce the risk of a systemic reaction after a subsequent sting from 60% in untreated patients to less than 3%.

77
Immunotherapy 40-60% pts with prior systemic reactions and positive IgE serum have systemic reactions following subsequent stings 40-60% pts with prior systemic reactions and positive IgE serum have systemic reactions following subsequent stings Re-sting reaction rate and intensity diminishes as the period between sting and re-exposure increases Re-sting reaction rate and intensity diminishes as the period between sting and re-exposure increases

78
Immunotherapy Who should be referred: Who should be referred: Pts who experience anaphylaxis Pts who experience anaphylaxis Controversial: Adults with exclusively dermal allergic reactions (urticaria and angioedema) Controversial: Adults with exclusively dermal allergic reactions (urticaria and angioedema) Who doesn’t need to be referred: Who doesn’t need to be referred: Local reactions, including large Local reactions, including large Children under 16 with exclusively dermal reactions (urticaria and angioedema) Children under 16 with exclusively dermal reactions (urticaria and angioedema)
 Controversial: Adults with exclusively dermal allergic reactions (urticaria and angioedema) Who doesn’t need to be referred: Who doesn’t need to be referred: Local reactions, including large Local reactions, including large Children under 16 with exclusively dermal reactions (urticaria and angioedema) Children under 16 with exclusively dermal reactions (urticaria and angioedema)")
79
Venoms Available Honeybee Honeybee Yellow jacket Yellow jacket Yellow hornet Yellow hornet Bald-faced hornet Bald-faced hornet Polistes (wasp) Polistes (wasp) Mixed Mixed
 Polistes (wasp) Mixed Mixed")
80
Principles of Avoidance Cover food and garbage Cover food and garbage Appropriate clothing – avoid bright, white and floral prints. Use dark and drab-colored clothing Appropriate clothing – avoid bright, white and floral prints. Use dark and drab-colored clothing Scented cosmetics, hair spray attract insects Scented cosmetics, hair spray attract insects Insecticides available Insecticides available Carry Epi-pen Carry Epi-pen

81
Immunotherapy

82
Of proven benefit in anaphylaxis secondary to hymenoptera venom. Recurrence anaphylaxis risk after systemic reaction to sting is reported at 50-70% Includes urticaria in adults, however recurrence risk with isolated urticaria in children is very low IgE mediated response Recurrence anaphylaxis risk after large local reaction is reported at <5%. Delayed hypersensitivity reaction (non IgE mediated)
.")
83
IMMUNOTHERAPY Hymenoptera Sting 80 – 99% of patients afforded complete protection after course of immunotherapy. Covered by Alberta Blue Cross or other Insurance Plans Otherwise serum costs about $125.00 per year Numerous protocols exist Weekly for 3 weeks then monthly for three years

84
IMMUNOTHERAPY Hymenoptera Sting Risks and Contraindications: Patients on Beta Blockers Poorly controlled asthma Don’t initiate during pregnancy Maintenance injections are safe Quoted mortality from Immunotherapy 1 in 2,000,000 injections Patients were high risk Hymenoptera injections appear safer than other allergens

85
IMMUNOTHERAPY Hymenoptera Sting Cost/Benefit Risk of death from sting is low 50/year in USA 5 in 20 years in Alberta Risk of therapy is virtually nil Improved Quality of life in treated patients is significant Oude Elberink JNG et al. Venom immunotherapy improves health- related quality of life in patients allergic to yellow jacket venom.J Allergy Clin Immunol 2002:110:174-82

86
Immunotherapy Who may benefit?

87
Allergist Referral Who may benefit? Hymenoptera Sting with systemic reaction Includes urticaria in Adults but not Children Does not include large local reaction Idiopathic Anaphylaxis Idiopathic Angioedema

88
Biphasic Anaphylaxis Does it really occur?

89
Kemp S, Lockey M, Wolf B, Lieberman P. Anaphylaxis: a review of 266 cases. Arch Intern Med 1995; 155:1749-54. No cases seen in retrospective study Stark B, Sullivan T. Biphasic and protracted anaphylaxis. J Allergy Clin Immunol 1986:78:76-83 5/25 patients developed hypotension or laryngeal edema after being asymptomatic 1-8 hours. 3 of 5 had initial glucocorticoid therapy. Brazil E, MacNamara A. Not so immediate hypersensitivity – the danger of biphasic anaphylactic reactions. J Accid Emerg Med 1998 252-53. 6/34 patients admitted post epinephrine for observation had biphasic reactions. This group required significantly more epinephrine to ameliorate initial symptoms.(1.2mg vrs 0.6 mg p=.03)
.")
90
Biphasic Anaphylaxis Does it really occur? Brady W, Luber S, et.al. Multiphasic anaphylaxis: an uncommon event in the emergency department. Academic Emergency Medicine 1997; 4:193-7 2 of 67 showed recurrent symptoms (solely urticaria) Protracted reaction occurred in 5/67 (3 on beta blockers) Ellis A, Day J. Biphasic anaphylaxis: a prospective evaluation of incidence, characteristics and predictors (abstract). Proceedings of the Fifth Annual Meeting for Basic Clinical Research Trainees;2002 May 29: Kingston (ON) 1/3 milder, 1/3 equal, and 1/3 more severe than initial reaction Mean time to onset is 10 hours (may be up to 38 hours)
 Protracted reaction occurred in 5/67 (3 on beta blockers) Ellis A, Day J. Biphasic anaphylaxis: a prospective evaluation of incidence, characteristics and predictors (abstract). Proceedings of the Fifth Annual Meeting for Basic Clinical Research Trainees;2002 May 29: Kingston (ON) 1/3 milder, 1/3 equal, and 1/3 more severe than initial reaction Mean time to onset is 10 hours (may be up to 38 hours).")
91
Biphasic Anaphylaxis What do the review articles say? Incidence may be up to 20% It is unclear whether many were actually protracted anaphylaxis Onset may be up to 36 hours (mean 10) Hard to predict which patients are at risk ? Those requiring aggressive initial epinephrine for resolution Some secondary reactions may be more severe than initial reaction. Corticosteroids may be partly protective.
 Hard to predict which patients are at risk . Those requiring aggressive initial epinephrine for resolution Some secondary reactions may be more severe than initial reaction. Corticosteroids may be partly protective..")
93
Biphasic anaphylaxis MacLeod Approach Decisions based on judgment not science Observation Period Observe those with serious initial symptoms in ED Extra caution with asthmatic patients Advise not to leave city for 24 hours Reliable companion is desirable Discharge Medications Epi Pen (absolute) Corticosteroids – 24 hours coverage is standard of care No clinical trials to support Many case reports where it didn’t help Theoretical advantage
 Corticosteroids – 24 hours coverage is standard of care No clinical trials to support Many case reports where it didn’t help Theoretical advantage")
94
Treatment of Anaphylaxis

95
Human Anaphylaxis Pathophysiology Secondary to degranulation of mast cells and basophils Anaphylactic = IgE dependent Anaphylactoid = IgE independent Chemical Mediators Histamine (H1, H2, ?H3) Tryptase, Chymase, Heparin Histamine-releasing factor Other cytokines Prostglandin D2, Leukotriene B4, platelet activating factor Leukotrienes C4, D4, E4
 Tryptase, Chymase, Heparin Histamine-releasing factor Other cytokines Prostglandin D2, Leukotriene B4, platelet activating factor Leukotrienes C4, D4, E4")
96
Treatment of Anaphylaxis Epinephrine The only proven medical therapy Several well done retrospective trials implicate delayed epinephrine with increased risk of death. Theoretic effect Antidote at all affected end-organs Mast cell stabilization through epinephrine receptors

97
Epinephrine Administration Simons F, et al. Epinephrine absorption in children with a history of anaphylaxis.J Allergy Clin Immunol 1998:101:33-7 Simons F, et al. Epinephrine absorption in adults: intramuscular versus subcutaneous injection. J Allergy Clin Immunol 2001:108:871-3 Observed SQ epinephrine resulted in skin blanching at injection site. Hypothesized that vasoconstriction interfered with absorption into the systemic circulation.

98
Epinephrine Administration Time to peak plasma epinephrine concentration Subcutaneous administration 34 +/- 14 minutes Intramuscular administration 8 +/- 2 minutes Ideal site of injection Peak Plasma concentrations significantly higher in vastis lateralis than deltoid muscle Simmons et al continued:

99
Pediatric Epinephrine Dose Dilemma EpiPen doses = 0.3 mg and 0.15 mg epinephrine Physician must choose to overdose or underdose a child between 15 and 30 kg.

100
Pediatric Epinephrine Dose Dilemma Simons et al.EpiPen Jr versus EpiPen in young children weighing 15-30 kg at risk for anaphylaxis.J Allergy Clin Immunol 2002:109:171-5 Children receiving.01-.014 mg/kg (Standard EpiPen) Significantly higher mean BP 30 minutes post injection Pallor, tremor, anxiety, palpitations in 100% of children Headache and nausea in some Prolonged QTc in one Children receiving < 0.01 mg/kg (EpiPen Jr.) No significant increase in mean BP Mild, transient side effects limited to pallor, tremor, or anxiety
 Significantly higher mean BP 30 minutes post injection Pallor, tremor, anxiety, palpitations in 100% of children Headache and nausea in some Prolonged QTc in one Children receiving < 0.01 mg/kg (EpiPen Jr.) No significant increase in mean BP Mild, transient side effects limited to pallor, tremor, or anxiety")
101
Treatment of Anaphylaxis The other lifesaving interventions Emergency Airway Management Rapid Volume Resuscitation 50% of circulating volume can third space in the first 10 minutes with severe anaphylaxis

102
Treatment of Anaphylaxis Antihistamines Cardiovascular H1 Receptors Coronary artery vasoconstriction Generalized vascular permeability H2 Receptors Atrial and ventricular contractile forces Atrial Rate Coronary artery vasodilatation

103
Treatment of Anaphylaxis Antihistamines Cutaneous Action: H1 Receptors Whealing, erythema, itching H2 Receptors Whealing, erythema

104
Treatment of Anaphylaxis Antihistamines Limitations Once histamine receptors are saturated, receptor blockade has minimal impact. In fasting individuals, onset of activity of orally ingested H1-antihistamines does not occur until 40-60 minutes, and maximal activity is not achieved for at least 4 hours. No good studies indicate benefit in non- cutaneous symptoms of anaphylaxis.

105
Treatment of Anaphylaxis Antihistamines Lin RY et al. Improved outcomes in patients with acute allergic syndromes who are treated with combined H1 and H2 antagonists.Ann Emerg Med 2000;36:462-8. 91 patients treated with diphenhydramine/saline or diphenhydramine/ranitidine. Significantly more urticaria free patients in experimental group (70.5%) at two hours than control group (46.5%) No significant difference in non-cutaneous symptoms. No difference in angioedema at 2 hours. Very few patients had non-cutaneous symptoms. Although it appears that H2 blockers added to H1 antihistamines improve cutaneous manifestations in acute allergic syndromes, their added benefit in reversing hypotension and bronchospasm associated with anaphylaxis remains unproven.
 at two hours than control group (46.5%) No significant difference in non-cutaneous symptoms. No difference in angioedema at 2 hours. Very few patients had non-cutaneous symptoms. Although it appears that H2 blockers added to H1 antihistamines improve cutaneous manifestations in acute allergic syndromes, their added benefit in reversing hypotension and bronchospasm associated with anaphylaxis remains unproven..")
106
Treatment of Anaphylaxis Corticosteroids Proven benefit in asthma. Theoretical benefit in anaphylaxis in preventing biphasic anaphylaxis. No controlled or uncontrolled studies to support Case reports exist of patients experiencing biphasic anaphylaxis post steroids Appear to be standard of care in many practice guidelines.

107
Treatment of Anaphylaxis Glucagon Anaphylaxis often doesn’t respond to epinephrine in patients taking beta blockers Glucagon directly activates adenyl cyclase and completely bypasses the beta-adrenergic receptor. May reverse refractory hypotension and bronchospasm. Dose 1-5 mg (20-30 mcg/kg in children) IV over 5 minutes then infusion of 5-15 mcg/minute titrated to response. Often causes vomiting – Beware of airway
 IV over 5 minutes then infusion of 5-15 mcg/minute titrated to response. Often causes vomiting – Beware of airway.")
108
Treatment of Peanut Anaphylaxis Activated Charcoal Vadas P,Perelman B. Activated charcoal forms non-IgE binding complexes with peanut proteins.J Allergy Clin Immunol 2003:112:175-9. In Vitro Study AC removed both IgE-binding and IgG-binding peanut proteins from solution rapidly at neutral and acidic pH. Complete loss of skin test reactivity in sensitive patients occurred when test serum was co incubated with activated charcoal. Results were maintained when peanut solution was held in chocolate or ice cream solutions.

109
Treatment of Peanut Anaphylaxis Activated Charcoal Risks as First Aid Treatment Delayed administration of epinephrine Difficulties in airway management with severe anaphylaxis.

110
Angioedema

111
Definition Urticarial lesions that form in deeper layers of the skin(deep dermis, or subcutaneous and submucosal layers), commonly in the region of the head and neck. May be IgE mediated Allergic May be bradykinin mediated ACE Inhibitors NSAIDS

112
Angioedema Zirkle M, Bhattacharyya N. Predictors of Airway Intervention in Angiodema of the Head and Neck.Otolaryngol Head Neck Surg.2000:123:240-45 Predictors of need for airway intervention Age Each 10 year increase in age increased likelihood ratio by 1.58 Angioedema involving oral cavity or oropharynx ACE inhibitors

113
Angioedema Ishoo E et al.Predicting Airway Risk in Angioedema:Staging System based on Presentation.Otolaryngol Head Neck Surg.1999:121:263-68 Predictors of ICU Stay or Airway Intervention Voice Change Hoarseness Stridor Dyspnea ACE Inhibitors

114
Exercise-Induced Anaphylaxis

115
Generalized pruritus, flushing, warmth and urticaria with vigorous physical activity. Occurs sporadically Can involve respiratory symptoms (59%) and GI symptoms (30%) Loss of consciousness, vascular collapse possible Severe headache up to 3 days is common
 and GI symptoms (30%) Loss of consciousness, vascular collapse possible Severe headache up to 3 days is common.")
116
Exercise-Induced Anaphylaxis Associations Postprandial state prior to exercise Specific foods prior to exercise Shellfish (8%) Celery (6%) Cabbage (6%) NSAIDS or ASA in combination with postprandial state
 Celery (6%) Cabbage (6%) NSAIDS or ASA in combination with postprandial state")
117
Exercise-Induced Anaphylaxis Treatment Recognition of symptoms and cessation of exercise Treat anaphylaxis in standard fashion. Prevention Activity modification Prophylactic antihistamines may blunt skin symptoms making recognition more difficult No reliable prophylactic medications exist.

118
Take Home Messages Don’t delay IM epinephrine Don’t use SQ epinephrine Immunotherapy is proven for hymenoptera sting with systemic reaction. Biphasic anaphylaxis does occur, but is likely overrated. Beware of asthmatics and those on beta blockers and ACE inhibitors.

Similar presentations











 Admission criteria for.>")







 type I.>")






 Diagnosis, Treatment, and Management of Systemic Reactions by Deborah Wolff-Baker.>")