Download presentation
Presentation is loading. Please wait.

1
Environmental Gerontology: Implications for healthy ageing Bernadette Bartlam

2
Context: geriatric medicine and gerontology at Keele – Tackling poverty and exclusion – Arguing for a stronger focus on social determinants in health research Environments of ageing – Creating conditions for healthy ageing Outline

3
Geriatric medicine and gerontology

4
Complexities of ageing "Man is born, grows up, and dies, according to certain laws which have never been properly investigated, either as a whole or in the mode of the mutual reactions" Lambert Quetelet (1796–1874), writing in 1835 Belgian mathematician, statistician, and astronomer
, writing in 1835 Belgian mathematician, statistician, and astronomer")
5
Quality of life: – more than absence of ill-health Related to four items: – health and functioning – the existence of relationships and social support – material circumstances – opportunities for personal growth and development Health as a means to an end… Higgs, P., Hyde, M., Wiggins, R. & Blane, D. (2003). Researching quality of life in early old age: the importance of the sociological dimension. Social Policy and Administration, 37, 239–252.
. Researching quality of life in early old age: the importance of the sociological dimension. Social Policy and Administration, 37, 239–252..")
6
The comprehensive study of ageing: physically psychologically socially Gerontology

7
UK Demographics Two thirds of the working population are taxpayers; only two in five pensioners have enough income to pay tax In 2006-7 the average income of the richest fifth of single pensioners was 279% that of the poorest fifth 45% of people aged 60+ in deprived urban neighbourhoods are in poverty, with 67% Pakistani and 77% Somali older people in poverty Scharf, 2009:25

8
Health inequalities cont The poorest older people are: –5 times more likely to have poor general health –5 times more likely to have difficulty walking –Twice as likely to have diabetes –Twice as likely as people under 50 to die Coote, 2009: 53

9
(Some) policy issues
 policy issues")
10
Older people as users of health services Older people are an important client group for health services, and they tend to use health services more than younger people…. The duration of the period when older people are heavy users of healthcare (period immediately preceding death) has not been increasing, but has instead been delayed as healthy life expectancy has increased.. the unnecessarily high costs that can arise from overly medicalized care solutions could be reduced with the use of more appropriate (and less expensive) forms of care. Timonen, 2008: 61
 has not been increasing, but has instead been delayed as healthy life expectancy has increased.. the unnecessarily high costs that can arise from overly medicalized care solutions could be reduced with the use of more appropriate (and less expensive) forms of care. Timonen, 2008: 61.")
11
Major challenges How to promote health and wellbeing across all sectors of society and societies –Create conditions for optimal ageing –Tackle poverty and exclusion, and the inequitable distribution of wealth –A stronger focus on social determinants in public health research WHO 2008

12
Health and social services Moving away from dependency and deficit to independence and wellbeing (BGOP; Audit Commission; DoH)
")
13
From this…. Park Hospital, Manchester: The birth of the NHS – opened by Health Secretary Aneurin Bevan, 5 th July 1948

14
To this… www.channel4.com/news/the-nhs-reforms-and-you

15
© Peter Crome

17
Geriatric Medicine & Gerontology at Keele

18
Environments of Ageing: New Lifestyles in Old Age?

19
Living in a Purpose-Built Retirement Community Background What we know What we don ’ t know: the challenges

20
Background: demography People aged 60 years + – 2005 = 673m – 2050 = 2 billion Every aspect of life is being affected Increasing numbers of older people living alone

21
Background: policy WHO (2002) Active Ageing Policy Framework (www.who.int/ageing/active_ageing) aim ofwww.who.int/ageing/active_ageing – ‘optimizing opportunities for health, participation and security in order to enhance quality of life as people age’. – emphasizes the need to create policies and environments which support individuals in realizing their potential, and in actively participating and contributing to their communities throughout their lives. – 2002 the Second World Assembly on Ageing in Madrid highlighted three priority directions, one of which was ‘ ensuring enabling and supportive environments ’. UK: Ageing in place as central to policy.

22
Background: Policy drivers – Positive alternative to residential and nursing home care. – Suitable for both ‘fit’ and ‘frail’ older people. – Encapsulated in initiatives such as: National Strategy for Housing in an Ageing Society Building our futures: meeting the housing needs of an ageing population

23
Why is home important? Home as micro-environment that: – enables us to experience autonomy, control, satisfaction and pleasure – source of safety and security – opportunity to (re)create positive life stories – supporting networks Key to healthy ageing: “ health is a state of complete physical, mental and social well-being and not merely the absence of disease ” (WHO, 1948: 100) Preamble to the Constitution of the World Health Organisation, signed into force 1948.
create positive life stories – supporting networks Key to healthy ageing: health is a state of complete physical, mental and social well-being and not merely the absence of disease (WHO, 1948: 100) Preamble to the Constitution of the World Health Organisation, signed into force")
24
Background RCs Retirement communities go back to Roman times – Religious affiliation – Victorian philanthropy Dramatic increase in 20 th century – In US purpose-built retirement communities now account for approximately 11% of all new housing. – No UK statistics! Elderly Accommodation Counsel (www.eac.org.uk) includes information on 937 schemes for rent or purchasewww.eac.org.uk

26
Background RCs Not-for-profit Housing Associations Private sector Differing models of ownership Range of accommodation options Varying degrees of support

27
The U.S Experience FORCs – formally occurring retirement communities NORCs – naturally occurring retirement communities LORCs – leisure oriented retirement communities CCRCs – continuing care retirement communities

28
Characteristics of RC residents in US Higher socio-economic groups Owner occupiers Better educated White collar occupations White Early retired/young elderly ‘ Childless ’ married couples Mobile earlier in life ie. an elite group?

29
Developments in the UK Spa towns Coastal resorts Estates, villages,towns Retirement hotels Mobile home parks Extra care housing schemes Continuing care retirement communities

30
RCs in Britain A Retirement Element residents no longer in full-time employment - affecting use of time and space. A Community Element an age-specific population - same geographically bounded area. A degree of Collectivity with which residents identify - may include shared activities, interests and facilities. A sense of Autonomy with Security. (Phillips et al, 2001)
.")
31
Lifetime Homes Originally termed ‘ multi-generational housing ’ A home for life adapts to changing needs over the life course. www.lifetimehomes.org.uk
32
Lifetime Homes contd. Additional considerations: Flexible, not standardised, interiors. Location. Amenities. Services. Transport links. Variety of housing.

33
Benefits Maintain/enhance quality of life Enhance ageing identities – Age homogeneity Combat loneliness Improve morale Engender healthier lifestyles Improve inter-generational relationships

34
Drawbacks Playpens for the elderly (Maggie Kuhn) Often exclude: – Minority groups – Those with mental or physical incapacity. May have difficulty in maintaining intergenerational links.

35
Berryhill Village New lifestyles in old age: health, identity and well-being in retirement communities 2000-2003 Miriam Bernard, Simon Biggs, Bernadette Bartlam & Julius Sim Funded by the Community Fund

36
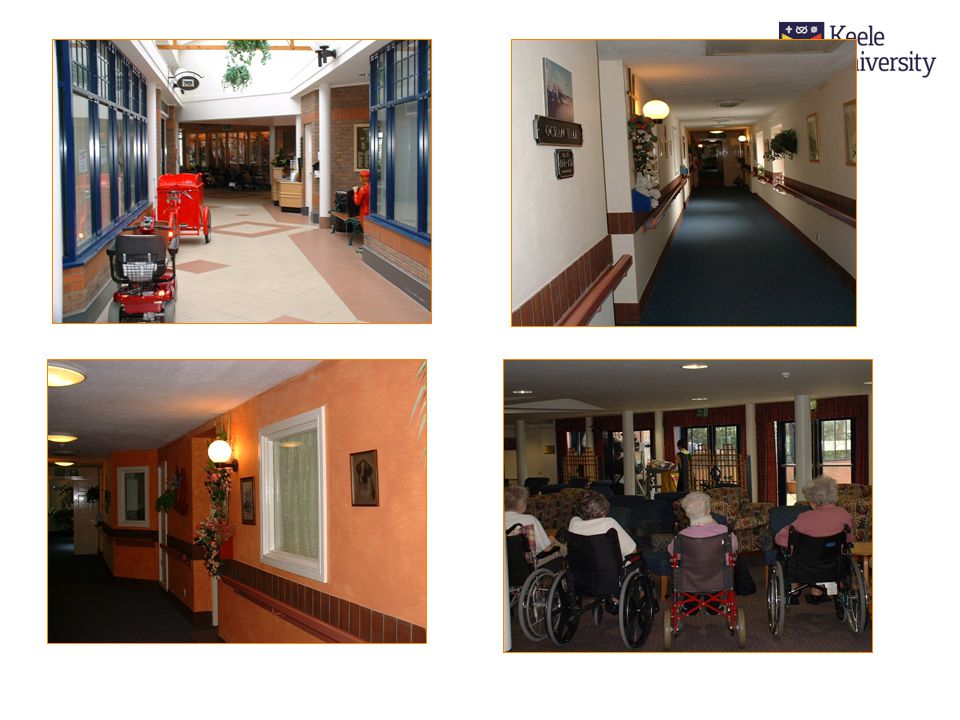
Findings: The Village Opened May 1998. At start of study (June 2000) had 159 people aged 55+. Single, 3-storey building with 148 flats on internal ‘ streets ’. All rented accommodation. Area: Amongst worst 15% nationally on MDR

40
The Villagers cont. 98/159 completed Wave 1 questionnaire (response rate = 62%). The men were either married or widowed. The women were mostly widowed (60%). 9 out of 10 left school at/before 15. ¾ employed in mining, steel and pottery industries. ¼ women had been housewives. All from within a 10 mile radius.
. 9 out of 10 left school at/before 15. ¾ employed in mining, steel and pottery industries. ¼ women had been housewives. All from within a 10 mile radius..")
41
The Villagers cont. Services eg housekeeping, shopping, laundry, pension collection, pop-in for illness. Facilities/amenities eg gym, shop, restaurant, library, computer room, hairdresser, craft and woodwork rooms, greenhouse, dreamscape room. Activities eg dancing, trips, keep fit classes, entertainment, gardening, volunteering opportunities. Communication facilitated by monthly street meetings, village newsletter, in-house television service.

42
Findings: The Villagers Average age is 75. One in ten are aged 85+. Women outnumber men by 2:1. Entirely white population. Majority live alone (70%). More women than men live alone (79% cf 50%).
. More women than men live alone (79% cf 50%)..")
43
Findings: Health and Well-being Own health/health of partner = most important reason for moving in: She was in hospital before she came here and they said then, if we wanted to be together this was the only place to be. So we came here. (Ron) ¾ residents have a limiting long-standing illness. Ill health = worst thing about growing older.
 ¾ residents have a limiting long-standing illness. Ill health = worst thing about growing older..")
44
Health and Well-being cont. Three quarters of people do not feel lonely: one in four do though. Of those who feel lonely, most (92%) live alone. More women than men cite loneliness as one of the worst features about growing older. Loneliness can be ‘ normal ’ : We're all lonely at times. Even if you're in your own house or even in here, you can be lonely. (Bernice)
 live alone. More women than men cite loneliness as one of the worst features about growing older. Loneliness can be ‘ normal ’ : We re all lonely at times. Even if you re in your own house or even in here, you can be lonely. (Bernice).")
45
Health and Well-being cont. Three quarters of people do not feel lonely: one in four do though. Of those who feel lonely, most (92%) live alone. More women than men cite loneliness as one of the worst features about growing older. Loneliness can be ‘ normal ’ : We're all lonely at times. Even if you're in your own house or even in here, you can be lonely. (Bernice)
 live alone. More women than men cite loneliness as one of the worst features about growing older. Loneliness can be ‘ normal ’ : We re all lonely at times. Even if you re in your own house or even in here, you can be lonely. (Bernice).")
46
Incidence of LLI The VillageLocal Community 1 Age/genderLLI n (%) No LLI n (%) LLI n (%) No LLI n (%) 55-64 9 (100)0 (0) 254 (44)317 (56) 65-7431 (86) 5 (14)258 (60) 175 (40) 75+48 (91)5 (9)159 (69) 72 (31) Male20 (83)4 (17)303 (54)257 (46) Female68 (92)6 (8)368 (55)307 (45) 1 10% higher than national average
 No LLI n (%) LLI n (%) No LLI n (%) (100)0 (0) 254 (44)317 (56) (86) 5 (14)258 (60) 175 (40) (91)5 (9)159 (69) 72 (31) Male20 (83)4 (17)303 (54)257 (46) Female68 (92)6 (8)368 (55)307 (45) 1 10% higher than national average")
47
Self-Perceived Health Status The villageLocal community Age band nSF12 PCS SF12 MCS nSF12 PCS SF12 MCS 65–74 37 39.72 (7.8) 43.02 (8.4) 1950 39.45 (12.1) 50.16 (10.9) 75+ 50 36.86 (6.9) 45.30 (7.0) 1483 34.76 (11.1) 47.31 (11.4) Mean (sd)
 (8.4) (12.1) (10.9) (6.9) (7.0) (11.1) (11.4) Mean (sd)")
48
Perceptions of health Angela My health has been better since I ’ ve been in here because I haven ’ t got the worry of being on my own…

49
Autonomy Madge: It's like you've got your own privacy. If you wanted to, you can shut your door and that's your house and you've got your privacy if you want it. If you want a bit of company, like we say,we just come downstairs as opposed to sitting in one another's flats sort of thing. I've never been one for neighbouring like you know, but I've always been friendly with everyone. Jane: You can still keep your own independence, just do what you want.

50
Security George: I think I’m more relaxed here than out there: I've got no pressures in here as I had there. I was worrying about whether the house was big enough to carry on, "Where are we going to go?" you know, "What is going to happen to her? Are we going to be split up?", and things like that. But here we won't, so we can get on with living. It has taken a lot of pressure off. Barbara:You feel safe at night with that bit of security round the building, and because somebody is next to you.

51
Sociability Jennifer: All being in this one building but having your own flats: you can come down and talk to one another. That's the difference as opposed to living in your house before where you were just on your own. It’s a different way of life, isn't it? Pat: I think, if you keep on taking an interest in things and talking to people and mixing, whereas if they live in a house on their own, it just stops, doesn't it? They've got no conversation with anybody and they get older, and they don't go doing things. So I think this sort of place changes all that.

52
Death and dying Margaret: You see the problem here is when somebody dies we all know. Now if we lived in a street or round the block as we used to call it, you wouldn ’ t notice it so much… Kathleen: And when you live outside, there isn ’ t just old people, there ’ s young ones and everyone, so it doesn ’ t seem as bad…

53
Peer Support Dora: I don't think I could have coped on my own. But because I was in here, and I had got Kathleen next door to me who came into me everyday, and loads of other people, I had a lot of support. Ethel: That's one of the joys of being in here, when you don't see as much of your family but then you've got people your own age, you've got the company.

54
A home for life? Mary: Up to now, I mean I am so far fine, but with my sight gone… I would have to go in a residential home, if my sight went. I ’ m comfortable at the moment, but just how far it will go I don ’ t know. But I ’ d rather be here than there as things are. I ’ d rather be here than there in any case.

55
Brenda: I don ’ t want to be shut away… I don ’ t want to wait for them to bring me down, and come for me… I feel I want something different… my sister ’ s mother-in-law is in there (Silverton nursing home) and I thought the set-up was ideal. She ’ s in a small ward with about four bed with their own wash-hand basis… she could see what was going on… she wasn’t shut away.

56
A New Lifestyle in Old Age? Rachel: My life was pretty restricted before I came in because I had a sick husband, we didn't get to go out, not that I'm grumbling. But now I go to the theatre, I paint, we have friends we talk to in a morning, we have entertainment - not every day - and I seem to have a more open life now.

57
Alice: My youngest daughter rings up and says, “ When can I make an appointment to see my mother? ” (laughter) Celia: Well, it ’ s true. Yes, we do seem to be getting busier. Kate: I mean, I ’ d love to go to the art class on a Monday and I ’ d like to go to the sewing class and bingo on a Tuesday… but we ’ re out so much. Alice: I haven ’ t got time! I ’ ve got less time now than I had when I was working full-time… Bernard: I think you get a lot of things in here… when I came in I said I shall come out in a box.
 Celia: Well, it ’ s true. Yes, we do seem to be getting busier. Kate: I mean, I ’ d love to go to the art class on a Monday and I ’ d like to go to the sewing class and bingo on a Tuesday… but we ’ re out so much. Alice: I haven ’ t got time. I ’ ve got less time now than I had when I was working full-time… Bernard: I think you get a lot of things in here… when I came in I said I shall come out in a box..")
58
What We Don ’ t Know: implications for policy and practice Definitions Philosophy Independence/inter-dependence Social cohesion – Diversity – Local communities

59
Implications for policy and practice 2 Accommodating different/changing needs – Gender – BME groups – Sexual orientation – Age A ‘ Home for Life ’ – Quality of build – Costs Staffing Sustainability

60
Acknowledgements Residents and Staff of Berryhill Village The ExtraCare Charitable Trust

Similar presentations





 Student Learning Experiences : stories from BME students in a North East University HE Academy Research.>")









 Disability.>")





![The Urban Infrastructure Challenge in Canada: Focusing on Housing Affordability and Choice Presentation by CHBA – [Name] to The Municipal Council of [Name]](/17/5358765/big_thumb.jpg "The Urban Infrastructure Challenge in Canada: Focusing on Housing Affordability and Choice Presentation by CHBA – [Name] to The Municipal Council of [Name]>")

