Download presentation
Presentation is loading. Please wait.

1
Risk Communication: An Introduction Baruch Fischhoff University Professor Carnegie Mellon Department of Social & Decision Sciences Department of Engineering & Public Policy Adapted for the SuperCourse from a talk to International Society for Pharmacoepidemiology” April 19-20, 2004

2
Overview Communication research strategies Two case studies medical informed consent public health information management Six brief examples Communication research management

3
Pressure for Lay Participation in Decisions Involving Risks health finance environment national security …

4
Poor Execution Can… undermine effective lay decision making create feelings of helplessness erode public faith in authorities erode authorities’ faith in the public erode the social coordination produced by sharing trusted information sources

5
Research Strategy Choices Begin with formal analysis? Persuasive or non-persuasive? Optimality or mastery? Which individual differences?

6
Research Strategy Choices Begin with formal analysis? Persuasive or non-persuasive? Optimality or mastery? Which individual differences? Also: Do you consider affect? social context? resources? …(potentially important, but outside present talk)
.")
7
Behavioral Decision Research Normative analysis of decision situation Descriptive behavioral research, in terms comparable to normative analysis Prescriptive interventions, closing gaps between normative ideal and descriptive reality

8
Behavioral Decision Research Strategy Choices Begin with formal analysis? yes Persuasive or non-persuasive? Non (default) Optimality or mastery? either Which individual differences? circumstances, values, competence
 Optimality or mastery. either Which individual differences. circumstances, values, competence.")
9
Three Classes of Information Quantitative How big are the risks - and benefits? Qualitative What determines risks - and benefits? Communication process What is social context of message?

10
calculating expected utility assessing the value of new information setting priorities applying a threshold for concern Uses of Quantitative Information

11
making quantitative information credible reconciling competing claims generating options monitoring environment for changes feeling realistically empowered Uses of Qualitative Information

12
establishing source credibility (competence, honesty) assessing source expectations (audience competence, locus of control) identifying conversational context (interpretation, reading between the lines) Uses of Process Information
 assessing source expectations (audience competence, locus of control) identifying conversational context (interpretation, reading between the lines) Uses of Process Information")
13
Surgery can extend life, but lots can go wrong. Patients face flood of information at a stressful time. Physicians face duty to inform. (with Jon Merz, Paul Fischbeck, Dennis Mazur) A Quantitative Information Example: Carotid Endarterechtomy
 A Quantitative Information Example: Carotid Endarterechtomy.")
14
Normative Analysis Value-of-information analysis, using risk analyses of patient - relevant outcomes, formalizing the materiality standard

15
death stroke facial paralysis myocardial infarction lung damage headache resurgery tracheostomy gastrointestinal upset broken teeth ……. Many Possible Side Effects

16
death 15.0% stroke 5.0 facial paralysis 3.0 myocardial infarction 1.1 lung damage 0.9 headache 0.8 resurgery 0.4 tracheostomy 0.2 gastrointestinal upset 0.09 broken teeth 0.01 (% that would decline, if they knew of each risk) But knowledge of only a few would affect many patients’ choices
 But knowledge of only a few would affect many patients’ choices")
17
Descriptive Research (anticipated) Patients don’t know probabilities of top risks: death, stroke, facial nerve paralysis Patients don’t know event meaning for facial paralysis
 Patients don’t know probabilities of top risks: death, stroke, facial nerve paralysis Patients don’t know event meaning for facial paralysis")
18
verbal quantifiers (e.g., “likely” threat) experientially unfamiliar events value uncertainty (what do I really want?) but not very low probabilities cumulative risk (from repeated exposure) Prescriptive Design Issues (1) Identify Communication Challenges
 experientially unfamiliar events value uncertainty (what do I really want ) but not very low probabilities cumulative risk (from repeated exposure) Prescriptive Design Issues (1) Identify Communication Challenges")
19
knowledge inferential ability appropriateness of confidence appropriateness of self-efficacy personally rational choices satisfaction (?) Prescriptive Design Issues (2) Choose Performance Measures
 Prescriptive Design Issues (2) Choose Performance Measures")
20
Conclusions Systematically using clinical trial results can: drastically simplify task (for patient & physician) formalize materiality standard set research priorities The adequacy of non-persuasive communication is plausible, but not proven
 formalize materiality standard set research priorities The adequacy of non-persuasive communication is plausible, but not proven")
21
Research Strategy Begin with formal analysis? yes Persuasive or non-persuasive? non Optimality or mastery? ptimality Which individual differences? health status, values (assume competence)
.")
22
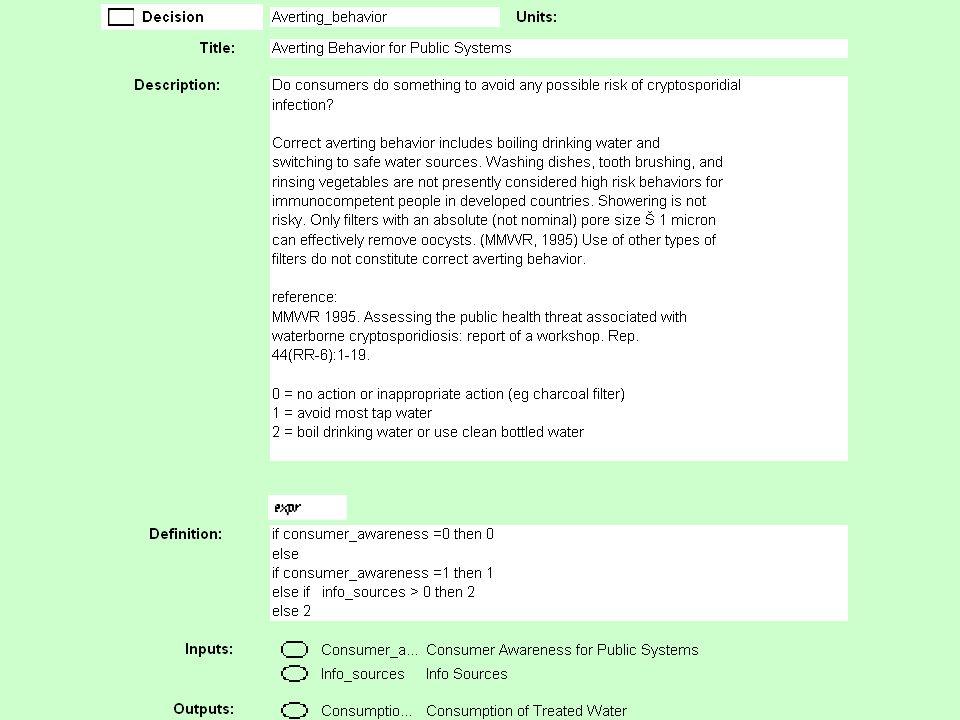
A Qualitative Information (and Communication Process) Example: Emergency Notification for Waterborne Pathogens Cryptosporidium intrusion in domestic water supplies. Special vulnerability for immunocompromised individuals. (Liz Casman, Felicia Wu, Claire Palmgren, Mitch Small, Joan Rose, Hadi Dowlatabadi)
.")
23
Normative Analysis Behaviorally realistic model of system performance, including detection, organizational coordination, and consumer response

26
Descriptive Research “Mental models” interviews (open-ended, structured by model) with: HIV+ individuals: knew a lot, could do little residents of communities with past intrusions: knew little, mildly curious
 with: HIV+ individuals: knew a lot, could do little residents of communities with past intrusions: knew little, mildly curious")
27
Conclusions Abandon emergency communication for crypto (perhaps OK for other contaminants, E. coli, bioterror) Provide bottled water to those at risk Reevaluate communications for other immunocompromised individuals
 Provide bottled water to those at risk Reevaluate communications for other immunocompromised individuals.")
28
Research Strategy Begin with formal analysis? yes Persuasive or non-persuasive? persuasive Optimality or mastery? mastery Which individual differences? health status, values, competence

29
Six Brief Examples Sexual assault prevention advice Teen STI risk Vaccines (anthrax, MMR) Dietary supplements Hazardous chemicals Homeland security
 Dietary supplements Hazardous chemicals Homeland security")
30
Problem: confident, universal, contradictory advice fosters confusion and guilt Normative: inventory of strategies, meta- analysis of effectiveness studies, identification of values Descriptive: nuanced belief structure, exaggerated effectiveness Prescriptive: create realistic expectations, promote research evaluating effectiveness Sexual Assault

31
Problem: flood of repetitious information creates illusion of understanding. Normative: influence diagram summarizing decision-relevant science Descriptive: broad knowledge of HIV/AIDS, with critical “bugs”; little knowledge of other STIs, limited feeling of control Prescriptive: targeted HIV/AIDS messages; DVD on sexual decision making STIs (teens)
.")
32
Problem: mistrust of officials affects trust in medicine Normative: comprehensive model of factors determining health, trust Descriptive: critical issues outside official problem space, terminological confusion Prescriptive: provide context, including “irrelevant concerns”; research as communication Vaccination (anthrax, MMR)
")
33
Problem: commercial-freedom-of-speech policies expanding direct-to-consumer communication Normative analysis: model sensitive to burden of responsibility for consumer/market failure Descriptive analysis: court-mandated labels may erode consumer rationality Prescriptive analysis: standardized, validated labels; legal standard for adequacy Dietary supplements

34
Problem: Can voluntary controls substitute for regulatory controls? Normative: diffusion/uptake model, including effects of behavior Descriptive: ineffective measures intuitively appealing (e.g., gloves, in- room breaks) Prescriptive: standardized, validated labels; legal standard for adequacy Hazardous Chemicals
 Prescriptive: standardized, validated labels; legal standard for adequacy Hazardous Chemicals.")
35
Problem: Plans without behavioral input Normative: Behaviorally realistic emergency response model Descriptive: Simple facts not transmitted; unfounded belief in panic; specific fears decline, general anxiety stable Prescriptive: Communication to experts, interdisciplinary teams, preemptive messages Homeland Security

36
Also… BSE SARS HRT GMOs Xenotransplantation smallpox (vaccination) …
 …")
37
General Conclusions Effective risk communication requires continuing collaboration among domain specialists, risk analysts, risk communicators, practitioners, and patients (or their representatives) -- with each willing to have its assumptions challenged.
 -- with each willing to have its assumptions challenged.")
38
Why doesn’t everyone adopt behavioral decision research?

39
Possible Professional Reasons need for specialization separation of research worlds isolation of researchers from practitioners predisposition to persuasion predisposition to sweeping generalizations …

40
Possible Management Reasons focus on single outcome narrow reviewing of proposals and products favor method application over development mandate to persuade difficulty of evaluating non-persuasive communications

41
Persuasive communication can inappropriately undermine credibility of public and experts alienate audience overlook critical audience goals & constraints impose bureaucratic priorities

42
Non-persuasive communication can inappropriately assume nonexistent abilities deny people needed protections muddle value issues leave wrong priorities unchallenged

43
Non-persuasive communication is needed when: No single, clear optimal choice multiple values, situations large uncertainties No clear advisory role experts distrusted shared decision-making option desired

44
The Empirical Question How competent are lay people to participate?

45
Many Strong Opinions, Drawn from assertion selected research evidence anecdotal observation small, unrepresentative samples speculative interpretation ambiguity regarding decision frame

46
technocratic control paternalistic regulation irrational public free markets popular democracy hyper-rational public “conservative” “liberal” Political predisposition: Behavioral assumption: Common Rhetorical Answers

47
The Empirical Question (reformulated) How competent are lay people to participate? -- when facing specific decisions -- and given half a chance

48
A (Complex) Working Hypothesis People often do sensible things if: They get relevant information in a concise, credible form with adequate context, and without distractions They have control over their environment and are judged by their own goals They have some minimal decision- making competence
 Working Hypothesis People often do sensible things if: They get relevant information in a concise, credible form with adequate context, and without distractions They have control over their environment and are judged by their own goals They have some minimal decision- making competence")
49
Lita Furby, Marcia Morgan, Julie Downs, Wändi Bruine de Bruin, Sara Eggers, Matt Dombroski, Donna Riley, Mitch Small, Steve Risotto, Dan Kovacs, Paul Fischbeck, Claire Palmgren, Robyn Dawes, Rebecca Parkin, Gordon Butte, Sarah Thorne, Martha Embrey, Jenn Lerner, Roxana Gonzalez, Deb Small, Gabriel Silverman, Lisa Schwartz, Steve Woloshin… Collaborators

50
Eggers, S.L., & Fischhoff, B. (in press). A defensible claim? Behaviorally realistic evaluation standards. Journal of Public Policy and Marketing. Fischhoff, B. (1992). Giving advice: Decision theory perspectives on sexual assault. American Psychologist, 47, 577-588. Fischhoff, B. (1994). What forecasts (seem to) mean. Intl Journal of Forecasting, 10, 387-403. Fischhoff, B. (1995). Risk perception and communication unplugged: Twenty years of process. Risk Analysis, 15, 137-145. Fischhoff, B. (1999). Why (cancer) risk communication can be hard. Journal of the National Cancer Institute Monographs, 25, 7-13. Fischhoff, B. (2000). Scientific management of science? Policy Sciences, 33, 73-87. Sources
. Giving advice: Decision theory perspectives on sexual assault. American Psychologist, 47, Fischhoff, B. (1994). What forecasts (seem to) mean. Intl Journal of Forecasting, 10, Fischhoff, B. (1995). Risk perception and communication unplugged: Twenty years of process. Risk Analysis, 15, Fischhoff, B. (1999). Why (cancer) risk communication can be hard. Journal of the National Cancer Institute Monographs, 25, Fischhoff, B. (2000). Scientific management of science. Policy Sciences, 33, Sources.")
Similar presentations