Download presentation
2
OPTICAL COHERENCE TOMOGRAPHY IN GLAUCOMA
OCT3 Welcome Clinical Aspects Of OPTICAL COHERENCE TOMOGRAPHY IN GLAUCOMA Presented by Akram Rismanchyin MD Isfahan University 2008 Anatomy 101 for Regional Managers

3
Glaucoma is an optic neuropathy characterized by a Typical parrem of visual field loss and optic nerve damage due to retinal gan'glion cell death caused by a number of different disorders that affect the eye: Most of these disorders are associated with elevated intraocular pressure (lOP), which is the most important risk factOr for glaucomatOus damage.
, which is the most important risk factOr for glaucomatOus damage.")
4
Although clinical examination of the optic nerve head has beenn considered to be the most sensitive test for detecting glaucomatOus damage, evidence suggests that examination of the retinal nerve fiber layer (RNFL)may provide important diagnostic information
may provide important diagnostic information")
5
Standard clinical techniques for assessing glaucOluatous changes, such as optic nerve head and NFL examination or visual fteld testingt lack sensitivity and reproducibility.

6
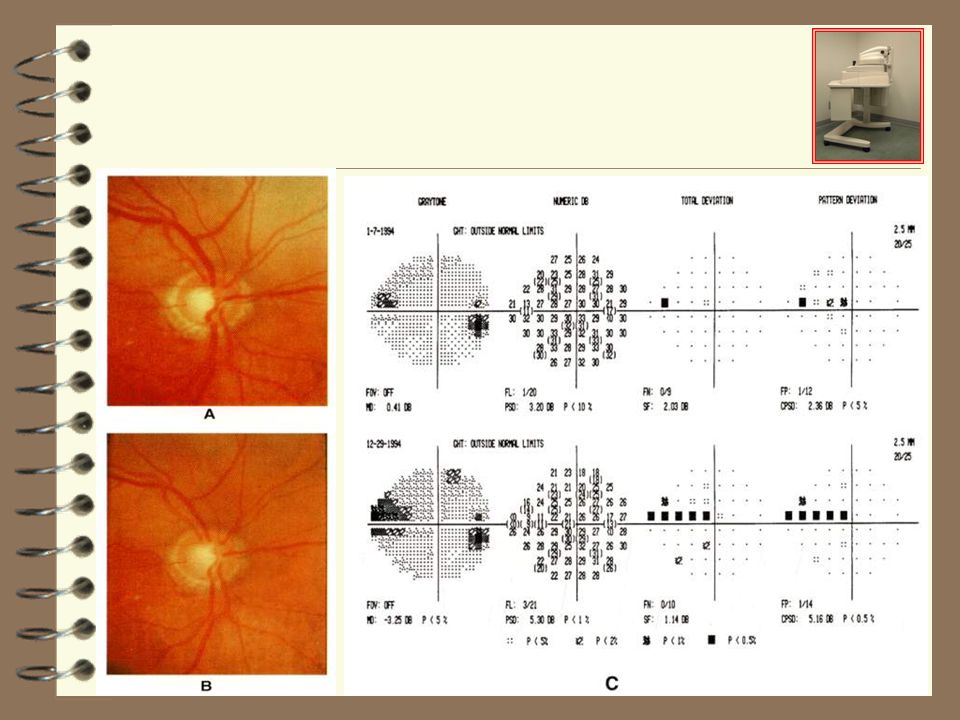
Visual evaluation of the optic nerve head by direct examination or by stereoscopic fundus photography is subjective, and the variability among experienced observers is often great

7
Visual field testing depends on patient cooperation and may also be influenced by non-glaucomatous vision Loss. Additionally) significant retiliainerve fiber layer loss mey precede both the development of visual field defects and identifiable cupping
 significant retiliainerve fiber layer loss mey precede both the development of visual field defects and identifiable cupping.")
8
HRT (cslo) Structural diagnosis GDX (sip) OCT
 Structural diagnosis GDX (sip) OCT")
9
Optical coherence tomography (OCT; Zeiss-Humphrey)
Introduced in 1991 Provides high-resolution cross-sectional imaging of the retina and the NFL. Is analogous to ultrasound B-scan imaging. A short coherence length diode source (850 nm).
.")
10
OCT / B-Scan

11
Resolution Conventional ultrasound: 150 mic
UBM 20 mic (penetration depth of 4 mm) CTS and MRI several hundred mic OCT I, II : mic OCT III : 8-10 mic Ultra- High resolution OCT : 2-3 mic
 CTS and MRI several hundred mic. OCT I, II : mic. OCT III : 8-10 mic. Ultra- High resolution OCT : 2-3 mic.")
12
Resolution Correlation between OCT and histopathologic examination revealed agreement for RNFL thicknesses within 10 μm OCT may underestimate histological NFL thickness by an average of 37% (Jones et al, 2001)
")
13
The operation of OCT is based on the principle of low coherence interferometry

14
Light is directed onto a partially reflecting mirror and is split into reference and measurement beams.

15
The measurement beam is reflected from the eye with minutely different time delays depending on its internal microstructure..

16
When the two light beams coincide, they produce a phenomenon known as interference, which is measured by a photodetector.

17
Retina - Histology Red Blue/Brown Ganglion Cell INL Nerve fiber layer
ONL (PR) Retinal Pigment Epithelium (RPE) IPL- OPL- PR OS- Choroid -Chorio- capillaris -Large choroidal
 Retinal. Pigment. Epithelium. (RPE) IPL- OPL- PR OS- Choroid. -Chorio- capillaris. -Large. choroidal.")
18
Retina - Histology Ganglion Cell INL Nerve fiber layer ONL (PR)
Retinal Pigment Epithelium (RPE) IPL- OPL- PR OS- Choroid -Chorio- capillaris -Large choroidal vessels
 IPL- OPL- PR OS- Choroid. -Chorio- capillaris. -Large. choroidal vessels.")
19
Retina - Histology RNFL Ganglion Cell Bodies Photo Receptors RPE

20
OCT3 Images In previous OCT images, we were able to see four layers of the retina. Now we are seeing 7, or sometimes 8.

21
We Now Believe That the Best Way to View OCT3 Images is in the B & W Mode. It Appears to Give More Details. OCT3 Images

22
Types of measurment in Glaucoma
NFL thickness in the peripapillary region circular (3.4mm) linear tomogram Optic nerve head profile Macular volume (has a reverse correlation with glaucoma damage)
 linear tomogram. Optic nerve head profile. Macular volume (has a reverse correlation with glaucoma damage)")
23
Other Clinical applications
Corneal thickness (Hoerauf et al. 2000) Anterior chamber depth (Hoerauf et al. 2000) for the diagnosis of angle closure glaucoma. Iris thickness and profile (Hoerauf et al. 2000), potentially useful for plateau iris, pigment dispersion and angle closure glaucoma.
 Anterior chamber depth (Hoerauf et al. 2000) for the diagnosis of angle closure glaucoma. Iris thickness and profile (Hoerauf et al. 2000), potentially useful for plateau iris, pigment dispersion and angle closure glaucoma.")
25
NFL thickness

26
Retinal Nerve Fiber Layer Analysis
Circular scans of 3.4 mm measures RNFL in the peripapillary region

27
Stratus OCT Printout RNFL Thickness Average Analysis RNFL 3.4 mm

28
Patient information scan information

29
Fundus Image To verify scan placement.

30
Scan Image The image with the lowest signal strength or with a data message will be shown to facilitate operator review.

31
Signal Strength Numbers range from 0 (weak) to 10 (strong).
images with a signal strength below 5 should not be used.

32
Sector Averages Quadrant Averages
Comparison to normative data in each sector is indicated with stoplight color scheme. Values are displayed numerically. Quadrant Averages Comparison to normative data in each quadrant is indicated with stoplight color scheme. Values are displayed numerically.

33
OCT3 Analysis Program The NEW OCT3 Analysis program is a software addition, providing normative data and statistical analysis for both retina and glaucoma applications. Data was collected on over 1200 eyes, at four centers in the US. The protocol of this study enabled Zeiss Humphrey Systems to establish an age-related normative database for Macular thickness and Retinal Nerve Fiber Layer thickness.

34
The mean RNFL thickness alone has a sensitivity of 84% and a specificity of 98% if its value is abnormal at the 5% level. If 1 clock-hours or 1 quadrants are abnormal at the 5% level, the sensitivity for glaucoma is 89% and the specificity is 92% to 95%, respectively

35
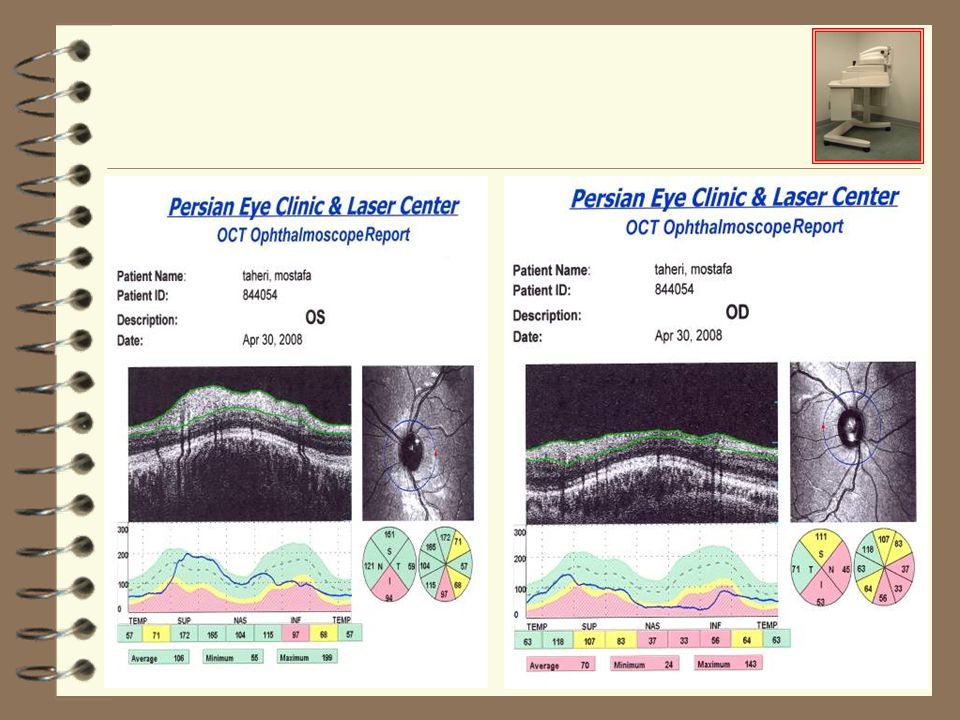
OD/OS Graph TSNIT line graph displays RNFL thickness in both eyes. Asymmetry may be indicative of glaucomatous loss.

36
Legend Normative data is displayed in stoplight color code, described in detail on inside back cover.

37
Best parameters for Sratus OCT
>or=1 quadrants abnormal p<5% >or=1 clock hours abnormal at p<5%

38
OCT RNFL Thickness Analysis – OU Overlay
OD in Blue OS in Green “Normal” eyes = Similar shape Abnormal eyes = Dissimilar shape Loss of RNFL in OS Superior “Hump” May be an Indication of Pathology

39
For each eye, values are compared to normative data and displayed in
Tabular Data For each eye, values are compared to normative data and displayed in stoplight color code, described in detail on inside back cover.

40
OCT Differentiates glaucomatous from non-glaucomatous eyes
Normal NFL thickness (with 3.4mm circular) (133+/- 17) Inferior (130+/- 18) Superior (80+/- 18) Nasal (75+/- 17) Temporal (105 +/- 11) mean But the normal and abnormal ranges overlap
 (133+/- 17) Inferior. (130+/- 18) Superior. (80+/- 18) Nasal (75+/- 17) Temporal. (105 +/- 11) mean. But the normal and abnormal ranges overlap.")
41
In new versions of OCT it is evaluated about symmetry of NFL (nerve fiber layer symmetry test)
Superior and inferior half divided to 3 to 5 segment and thickness of NFL compare with each other in each segment

42
ABILITY TO DETECT CHANGE
Change analysis software has recently been introduced However, statistical units of change probability are not provided It is difficult to differentiate true physiologic change from test-retest variability.

43
RNFL Thickness Serial Analysis Comparative analysis of RNFL thickness over time. Can be applied to up to 4 OD and/or 4 OS scan groups

44
Optic Nerve Head Analysis
Objectively finds Margin of Disk using signal from end of Retina Pigment Epithelium Not accurate on: - Peripapilary Atrophy - Staphyloma

45
Optic Nerve Head Analysis
Radial line scans through optic disc provide crosssectional information on cupping and neuroretinal rim area Disc margins are objectively identified using signal from end of RPE Key parameters include cup-to-disc ratio and horizontal integrated rim volume

46
Optic Nerve Head Analysis
Objectively finds Cup and calculates volumes and areas of the ONH User can modify placement of disk Does not require reference plane as with other technologies

47
ONH Indices

48
ONH measurements with OCT
Compared with ONH measurements, RNFL thickness may be a better indicator of retinal ganglion cell function and disease progression.

49
Macular Thickness Analysis `
Thinning of the macula may reflect glaucomatous loss

50
Stoplight Color Scheme

52
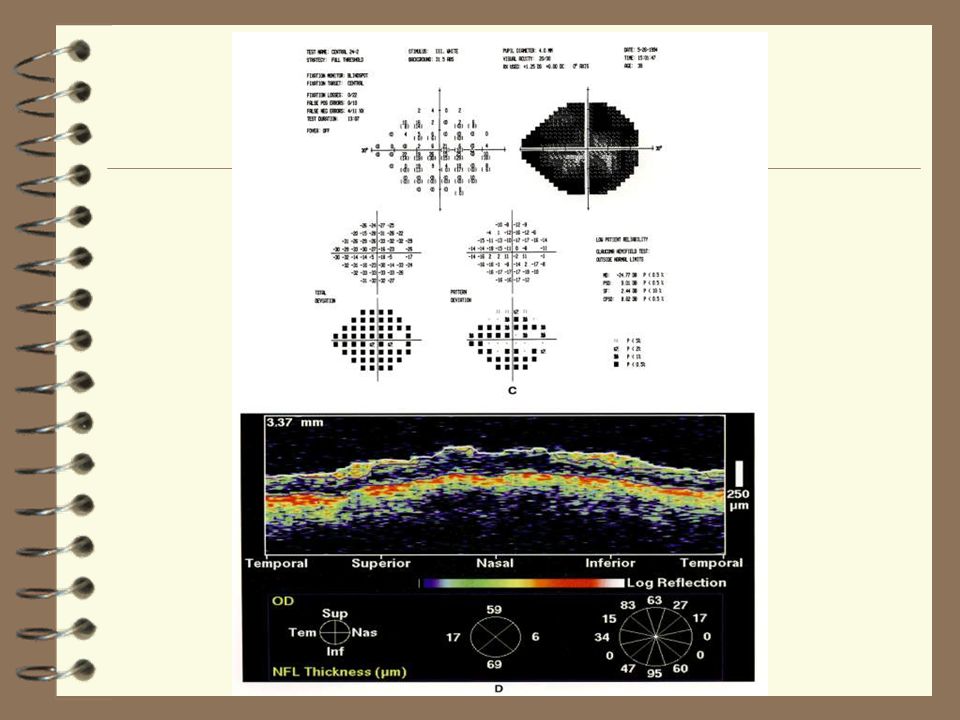
Healthy eye The anterior and posterior highly reflecting layers (shown in red), representing the RNFL and RPE
, representing the RNFL and RPE.")
53
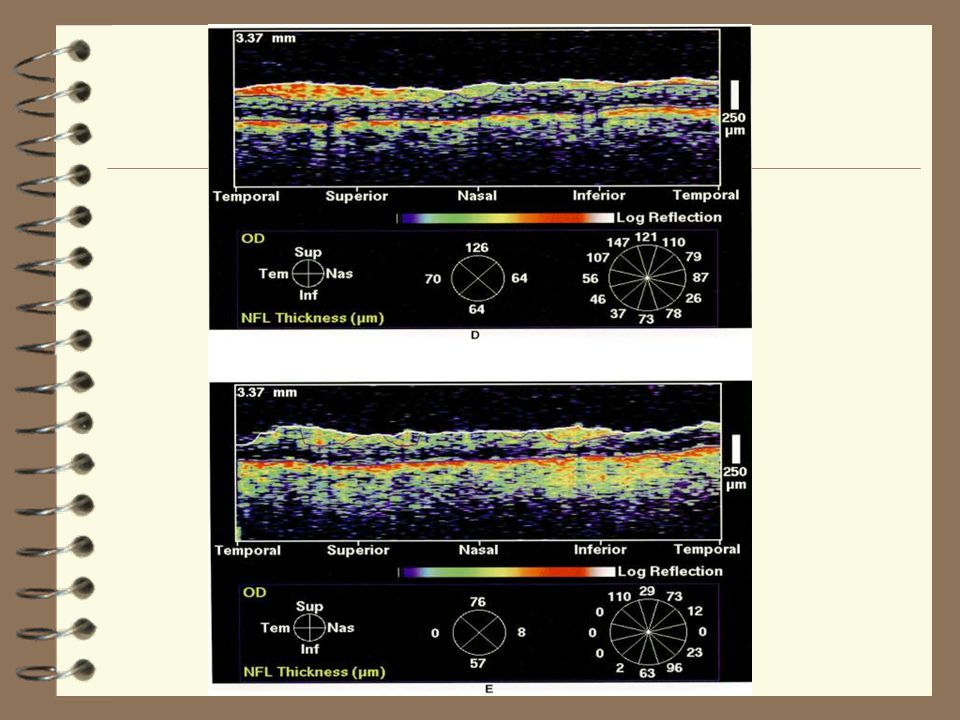
Glaucomatous eye A broad focal defect in the superotemporal quadrant with thinning of the RNFL to less than 50 μm.

55
Shows a baseline and follow-up image of an uncontrolled glaucomatous eye after a 16-month interval.
Thinning of the RNFL in the inferotemporal quadrant

56
Superior Arcuate Scotoma

57
GLAUCOMA NORMAL

69
OCT Advantages Noninvasive Non-contact High resolution
High sensitivity Not affected by axial length and refraction Not affected by moderate nuclear sclerotic cataracts.

70
ADVANTAGES Objective, quantitative, reproducible
In contrast with other imaging techniques, direct measurements of the RNFL An anterior segment compensator is unnecessary and structural information is independent of a reference plane.

71
DISADVANTAGES High cost
Posterior subcapsular and cortical cataracts impairs performance Currently change analysis software lacks statistical units of change probability, making it difficult to differentiate biological change from measurement variability.

72
Imaging versus examination
The quantitative methods HRT, SLP, and OCT were no better than qualitative assessment of ONH by experienced observers at distinguishing normal eyes from those with early to moderate glaucoma.

73
In Summary It is not recommended that clinical decisions be based on the results of any single imaging test, as with visual field testing. Clinical correlation is essential and management must be tailored to each individual patient.

74
Thank You
















 0.005% qd – Travatan®(travoprost) 0.004% qd – Lumigan® (bimatoprost)>")




 A presentation courtesy of Zeiss.>")






 is an upcoming new technology that allows non-invasive, optical medical diagnostic.>")



