Download presentation
Presentation is loading. Please wait.

1
Outline Musculoskeletal injuries Heat Illnesses
Risks Classification Treatment Heat Illnesses Evaluation of test quality Field tests Anaerobic Aerobic

2
Musculoskeletal Injuries
Risk increases for all levels of participation with increasing Activity, intensity and duration Incidence and severity can be reduced by understanding Risks, preventative measures and care Risks 35-60% of runners report injuries that reduce running or require medical attention Patellar femoral articulation and foot High impact aerobic dance 45 % of students 75% of instructors Lower leg injuries with high frequency (> 3 times per week)
")
3
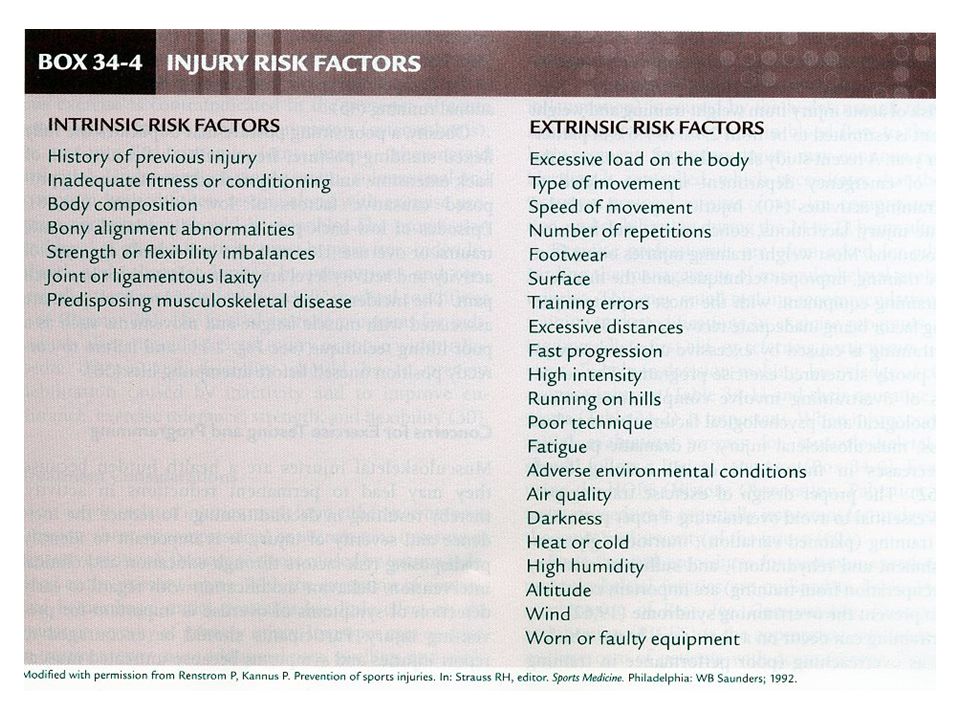
Injuries intrinsic and extrinsic factors interact Box 34.4 ACSM
Poor biomechanics, past physical activity, poor baseline fitness, present level of training and weight load affect incidence of injury

5
Injuries Repetitive bouts of micro trauma leading to overt tissue injury cause overuse injuries Running injury increases exponentially with frequency and total volume of training Beginning jogger - one day rest Progress to low impact activity on off days Training errors are causal in % of running injuries Eg. high progression rates and hill running

6
Warm up / Flexibility Low flexibility is a risk factor
Muscle strain and musculoskeletal injury Research study - most and least flexible had higher risk Improper warm up - inc risk for injury Warmth - inc elasticity of connective tissue, speeds metabolism, inc magnitude and speed of contraction Muscle stretches more and can resist injury at greater force Studies are inconclusive on warm up and injury - may be more important for performance

7
Orthopedic Factors Past injury and low physical activity are associated with risk Excessive weight - acute and overuse injuries - hip and knee Vigorous activity may predispose to osteoarthritis due to mechanical trauma Inc risk with competitive but not recreational running Low back pain risk factors Obesity, poor sitting posture, frequent flexion, loss of back extension and low activity Poor lifting posture and fatigue Usually related to acute trauma or overuse

8
Recommendations Alter predisposing risk factors through education and clinical intervention Early detection of symptoms and overuse - full rehabilitation Do not recommend strenuous exercise for those with: Acute joint injury Chronic joint inflammation (osteoarthritis) Uncontrolled systemic joint disease (rheumatoid arthritis) For those with joint disease; Progression needs to be individualized Prevent debilitation due to inactivity Improve endurance, strength and flexibility and exercise tolerance
 Uncontrolled systemic joint disease (rheumatoid arthritis) For those with joint disease; Progression needs to be individualized. Prevent debilitation due to inactivity. Improve endurance, strength and flexibility and exercise tolerance.")
9
Preventing Injuries Prescreening
Well rounded physical training program Warm up / cool down General and specific Flexibility, strength and aerobic conditioning Follow principles Specificity, overload, progression Proper equipment and techniques

10
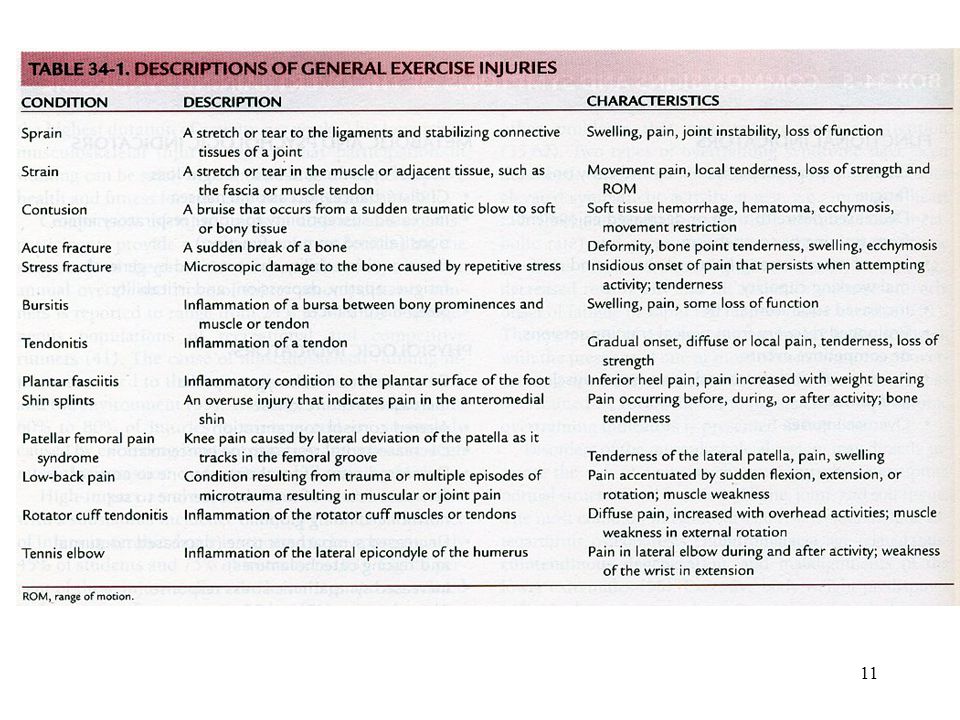
Recognition Exercise professionals will often be asked for advice regarding injuries or the need for referral We are not physiotherapists or doctors but an awareness can help us assist clients in making educated choices when dealing with injury Common injury symptoms and causes ACSM Table 57.4 and 57.5 Runners knee - patellar femoral pain syndrome Shin splints - tibial stress syndrome (periostitis) Plantar fasciitis Achilles tendonitis
 Plantar fasciitis. Achilles tendonitis.")
13
Running Injuries

14
Running Injuries Plantar fasciitis -inflammation of plantar fascia tendon tingling, ripping in AM stiff/hard midsoles (old shoes) poor arch support running in court shoes
 poor arch support. running in court shoes.")
15
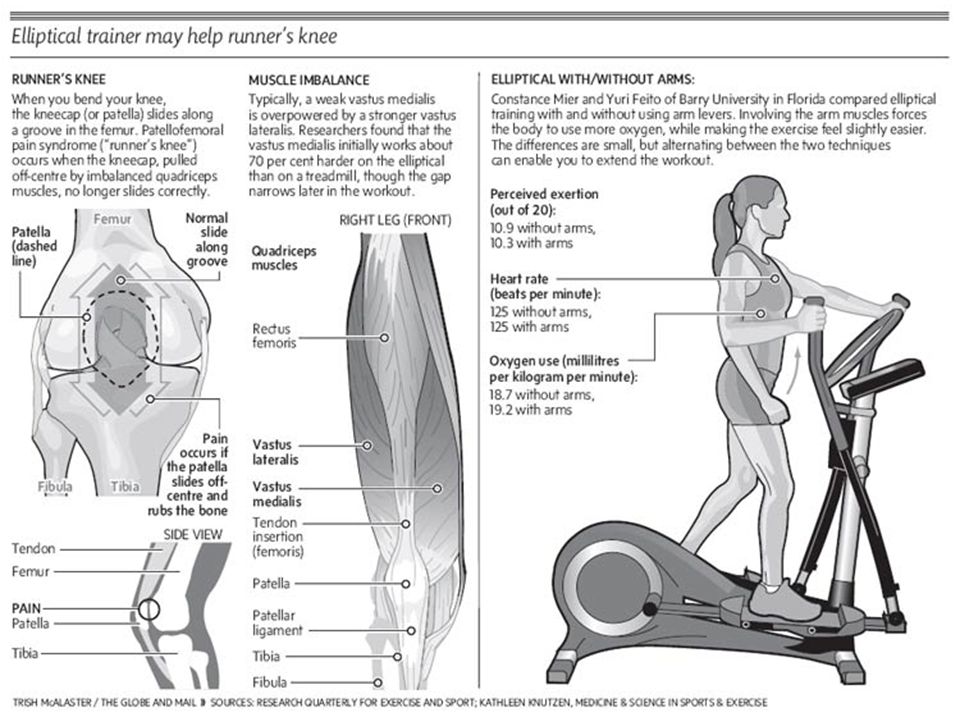
Running Injuries Runner knee - pain around pattelo-femoral joint
excess pronation - increases force holding patella against femur inc. internal rotation - alignment off orthotics - motion control in rear foot Build endurance of vastus medialis

17
Injury Management HOPS Evaluate for Physiology of Injured tissue
History, Observation, Palpation and Special tests Evaluate for Immediate first aid and referral to physician Advice about training and program modifications Physiology of Injured tissue Macro trauma - tension, shear or compression Micro trauma - overuse, cyclic loading Damaged cell unable to process O2, nutrients, waste - leads to cell necrosis Blood vessel damage - hemorrhage, coagulation and decreased blood flow to area Primary injury - direct trauma Secondary injury - additional swelling and tissue damage - more with improper care results from reduced O2 supply adjacent to primary injury further necrosis, swelling - hours after injury

18
RICES Rest Ice Compression Elevation Stabilization
range form complete to relative rest Allows time to control effects of trauma and avoid additional tissue damage Ice Slows cell metabolism - healthy tissue survives diminished blood flow and hypoxia Reduce pain and spasm Apply for minutes every 2 hrs during the day for first 24 hrs post injury Compression Controls edema and prevent fluid accumulation in the injured area Elevation Above level of heart - limits swelling and increases venous return - reducing tissue damage Stabilization Supports injured area allowing musculature to relax - reducing pain-spasm cycle

19
Healing Inflammation, Repair, Remodeling
Time to fully recover depends on injury and treatment during each phase Inflammation - redness, local heat, swelling, pain and loss of function Sliverthorn table 24.2, Berne and Levy fig 45.19 Protection and prepare for repair Lasts up to 2-3 days Chronic inflammation may occur when cause of injury in not eliminated - delaying rehabilitation process - Treatment goal - prevent damage of healthy tissue, create good environment for new tissue growth - RICE, ultrasound, electrical stimulation - maintain health of rest of body through modified training

20
Healing Repair - within initial hours - depending on resolution of inflammation (2-3 days) Proliferation and regeneration of collagen fiber leads to scar formation - not as structurally sound May last up to two months Treatment goal - prevent excessive atrophy and joint deterioration gradually introduce low load stresses to increase collagen synthesis and prevent loss of joint motion - ultrasound, electrical stimulation and ice Maintain fitness of uninjured areas through modified activity Proprioception and neuromuscular control - stability, vision and speed Remodeling - realignment of collagen according to tensile forces Scar tissue becomes stronger, regeneration of collagen slows With increased loading the collagen fibers begin to hypertrophy and align themselves along the lines of stress Ligament repair can take up to a year Duration of remodeling extended with excessive strain or re-injury Treatment Goal - optimize tissue function through progressive loading Move from general to sport specific, functional exercises

21
Follow up treatment Cold effective in reducing chronic swelling
Heat - should not be applied until after acute inflammation phase After first hours May “flush” injured area by increasing circulation May reduce pain, increasing mobility Contrast baths - anecdotal support Exercise is most important follow-up treatment Treatment should be directed by physician or physiotherapist

25
Evaluation of Test Quality
You must decide if a test is; Valid? Reliable? Objective? Safe? Comparable to Norms? Appropriate? Economically your best choice? Objectivity - accuracy of scoring system - long jump vs figure skating Intra judge (often masks errors, ok test retest) Inter judge - standardization, certification
 Inter judge - standardization, certification.")
26
Validity How well does a test measure what it is intended to measure - most important aspect of test design There are several types of validity Logical Validity degree to which a test measures an underlying attribute based on existing knowledge Old CSTF sit-up test - legs held, hands behind neck, rate of 60 / min Inappropriately tests psoas muscles at high contraction rate Partial curl ups now put focus on endurance of abdominal muscles Construct validity - degree to which a test measures an attribute or trait that cannot be directly measured Athletic ability, anxiety, percent body fat Content validity Is the test battery measuring all the component abilities for performance List ability components for sport, and ensure they are all represented Eg soccer - speed, agility, coordination, kicking power…

27
Validity (cont.) Criterion-Referenced Validity - includes concurrent and predictive Concurrent Validity Used when a test is proposed as a substitute for another valid test Degree of correlation with a original test should be reported over .8 correlation coefficient is acceptable. eg. Coopers Test and VO2 Max (.897) (see next slide) SEE - standard error of estimation - should also be small However, Cooper used adults who were well trained and motivated ? Applicability to other groups ? Predictive validity - amount by which test score corresponds to future behavior or performance Does prior fitness actually reduce injury in demanding jobs? Do fitness scores relate to sport performance measures? (goals, rebounds, assists)
 (see next slide) SEE - standard error of estimation - should also be small. However, Cooper used adults who were well trained and motivated. Applicability to other groups Predictive validity - amount by which test score corresponds to future behavior or performance. Does prior fitness actually reduce injury in demanding jobs Do fitness scores relate to sport performance measures (goals, rebounds, assists)")
29
Reliability Definition 1 - Consistency or repeatability of a test
a test must be reliable to be valid test can be reliable but invalid Eg. 60 sec sit up test Definition 2 - ability of the test to detect reliable differences between subjects Pass/Fail tells us very little if everyone gets the same result Important when comparing to norms Ensure test is being administered as it was designed Single test, test retest, individual test score vs group of subjects (BMI) Factors influencing reliability Type of test, level and range of ability, Length Consistency of client preparation
 Factors influencing reliability. Type of test, level and range of ability, Length. Consistency of client preparation.")
30
Objectivity Accuracy in scoring a test
Quantitative vs qualitative Long jump vs gymnastics Intrajudge objectivity - errors often masked, Can be ok for test re test situations after months of training Interjudge objectivity - degree to which different testers agree Standardization of training and certification important Sources of error Skill of administrator (eg. skin folds) Calibration of equipment Personality of subject (motivation)
 Calibration of equipment. Personality of subject (motivation)")
31
Referenced Tests Norm-referenced test: Criterion-referenced test:
the test score is compared to a norm so the person can be compared against others in the same age and gender category Criterion-referenced test: the test score is compared to a standard. This target could be set appropriately for the age and gender Eg police and fire fighter standard tests validating a criterion (pass/fail) is a difficult task, while using a normative database and just reporting a percentile ranking is easier. most criterions are based on normative data originally, could also be based on assessment of requirements for successful performance
 is a difficult task, while using a normative database and just reporting a percentile ranking is easier. most criterions are based on normative data originally, could also be based on assessment of requirements for successful performance.")
32
Field-Tests Laboratory Aerobic and Anaerobic Tests
Advantages and Disadvantages allow examiners to test numerous participants at once without the need for sophisticated and expensive equipment. Validity of Field-Tests Field-tests are not as accurate as the original test they are designed to emulate Field-tests are usually used as motivational tools rather than in scientific studies, so the lower level of accuracy is often quite acceptable Care must be taken however to use the field test on the population group it was designed for (may have concurrent validity for a certain age population but not for another)
")
33
Field Test Reliability Normative Databases
If the field-test does not have a skill component they will usually be very reliable e.g. Cooper test requires pacing skill Simple tests of maximal strength, like the grip strength, have very high reliability Objectivity Field-tests usually have excellent objectivity (e.g. timed runs, laps completed in set amount of time) Normative Databases Field-tests often have large databases, in part because so many people can be tested easily Care should be taken to use the appropriate database for the clients whom you have tested
 Normative Databases. Field-tests often have large databases, in part because so many people can be tested easily. Care should be taken to use the appropriate database for the clients whom you have tested.")
34
Safety of Field Tests Most aerobic tests are sub maximal and less likely to put excessive strain on subject 20m aerobic shuttle is maximal Screening during test often difficult ECG, BP Rely on prescreening tests Anaerobic tests require maximal effort - select clients carefully High risk of muscle strain in sprint tests if not fully warmed-up or inexperienced with sprinting

35
Field Tests Virtually all field-tests are very inexpensive to run
test numerous subjects at the same time, reducing personnel costs minimal equipment is required There are numerous field-tests available so finding an appropriate test for your client(s) should not be a problem.
 should not be a problem.")
36
Lab Organization Warm Up (done in the 10 min prior to test participation) 2 laps of 400m track Stretching (optional) 2 X 50 m sprints at % max (optional) Purpose to have you complete, administer and/or observe some common filed tests Decide after outline which you will participate in as a subject one aerobic one anaerobic if you are used to sprinting
 Purpose. to have you complete, administer and/or observe some common filed tests. Decide after outline which you will participate in as a subject. one aerobic. one anaerobic if you are used to sprinting.")
37
Anaerobic Lactic acid and Alactic Systems
Usually reserved for specific sports groups does not contribute to cardiovascular/respiratory fitness can be associated with muscle strain 600 m and 100 m shuttle tests norms are for elite athletes useful on test/retest basis only require good warm up/stretching T-Test Test of agility (approximately seconds) Two trials
 Two trials.")
38
Anaerobic cont. 600m Run 100m shuttle 50 yard sprint
Lactic acid System 2 trials (one in 343) 4 runners max. use inside lane warm up essential 100m shuttle alactic/lactic acid systems sprint 5 times between 20m lines practice trial at 75 % 50 yard sprint alactic system
 4 runners max. use inside lane. warm up essential. 100m shuttle. alactic/lactic acid systems. sprint 5 times between 20m lines. practice trial at 75 % 50 yard sprint. alactic system.")
39
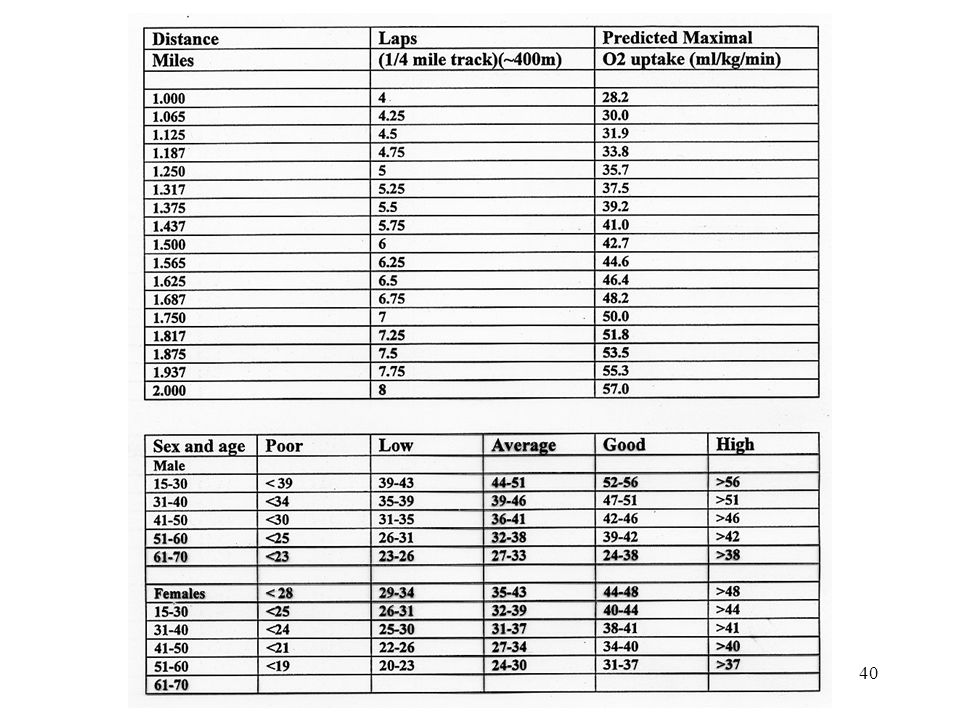
Aerobic System Coopers Test
Target subjects - large groups, assumed to be healthy, experience running as pacing is important Normative data for Swim and Bike Coopers tests are also available warm up important 12 minutes around 400 m track pacing is important (experience) up to 30 runners, keep to inside lane use table p. 12 for miles and VO2 max estimates administrator calls out times and records completed laps - to nearest quarter or tenth good correlation to VO2 max test results
 up to 30 runners, keep to inside lane. use table p. 12 for miles and VO2 max estimates. administrator calls out times and records completed laps - to nearest quarter or tenth. good correlation to VO2 max test results.")
41
Aerobic cont. 20 m Aerobic shuttle Target subjects warm up in protocol
Healthy subjects of any age warm up in protocol avoids pacing problem pace increases progressively from brisk walk If subject fails to keep pace by two steps on two consecutive laps the last number called out is their stage level MET estimated by stage and age MET is Metabolic Equivalent 1 MET = 3.5 ml O2 kg-1 min-1

42
Aerobic cont. Rockport Fitness Walking Test Target group
sedentary, older individuals, those not accustomed to running walk at fast, comfortable pace record time for four laps timer can use lap function for more than one subject record 10 second heart rate at finish using stop watch Compare results to age and gender specific graphs in lab book

43
Aerobic Tests (cont) 1.5 mile run Target subjects
Large groups Prior experience running this test distance as pacing is important Timed test - 6 laps of 400 m track Moderate warm up and stretch One administrator can time up to four subjects, keeping track of completed laps Compare time to age and gender specific fitness scale

Similar presentations