Download presentation
Presentation is loading. Please wait.

1
Quality Education for SENiors Marsha Lewis, PhD, RN Bethany Robertson, DNP, RN Gerri Lamb, PhD, RN, FAAN Corrine Abraham, MN, RN

2
It’s been a busy year 100 seniors QSENed - Recognize QI process and tools when they see them - Aware of and can search national quality initiatives: IHI, JCAHO, NQF - Can conduct simple PDSA process using appropriate tools, run charts, fishbone, … 30+ faculty/4 courses - Speak “TeamSTEPPs” language - Experience facilitating QI process - Ask quality-centric questions in clinical

3
“Begin with the end in mind” Covey,1989 Focus our pilot work on the senior spring semester What competencies do our students need to transition from Emory student to practicing RN? Back this up a bit and try some small experiments in the junior year What groundwork do we need to establish to build toward terminal competencies?

4
The timing was perfect “Getting into the habit of quality” Emory Health Sciences Update March 2008 Fred Sanfilippo, MD, PhD Executive VP and CEO Emory Woodruff Health Sciences Center

5
A Comprehensive Model for Teaching QSEN Success in Achieving QSEN Competencies Curriculum Faculty Development Clinical Partners Student Engagement

6
I. Curriculum Quality and safety as central themes Strong connection between classroom and clinical Experience analyzing teamwork, QI, in addition to reflective exercises Role model QI thinking – flexibility, feasibility, always “OFIs”, evidence

7
An Integrated Curriculum Nursing Practice Patient-Centered Care Across the Care Continuum (Clinical Experiences) Classroom Professional Development Classroom & Clinical Seminars Simulations
 Classroom Professional Development Classroom & Clinical Seminars Simulations")
8
Integrating Across PD Class, Seminar and Clinical Groups PD Class PD Seminar Role Transition & Community Clinical Groups PTQS Concepts Principles Tools Students- Mentors practice Concepts & tools Discussion of Clinical Application PTQS Questions

9
Safety – for example QSEN Competency: Discuss impact of national safety initiatives PD Class PD Seminar Role Transition & Community Clinical Groups PTQS Major national safety initiatives e.g. JCAHO, NDNQI, NQF, IHI … Students explore websites related to national initiatives with guided questions QS Question: RT: What quality initiatives affect practice in this setting? What outcomes are being tracked? C: What population-based outcomes are relevant to what you’ve observed this week? How are outcomes from other settings relevant to community practice?

10
Role Transition & Community Clinical Groups Teamwork – for example QSEN Competency: Discuss effective strategies for communicating among members of the interdisciplinary team PD Class PD Seminar PTQS Comm. & Patient safety Tools Pick a process: communicating a change in patient status, (hand-offs). Practice communication tools: SBAR, IPASStheBATON, etc. T Question: RT: What forms of team communication have you seen/been part of this week? Which were effective, not… C: Same plus: how is communication the same/different in community settings? How do community members participate?
. Practice communication tools: SBAR, IPASStheBATON, etc. T Question: RT: What forms of team communication have you seen/been part of this week. Which were effective, not… C: Same plus: how is communication the same/different in community settings. How do community members participate .")
11
II. Faculty Development “Quality and safety: nursing at the turning point” Jan 2008 Keynote Marla Salmon, Dean

12
The Case for Quality Why We Must Improve Susan M. Grant, MS, RN, CNAA Chief Nursing Officer, EHC William A. Bornstein, MD, PhD Chief Quality Officer, EHC III. Clinical Partners III. Clinical Partners Emory Healthcare Quality Academy Office of Quality N

13
IV. Student Engagement “In your efforts to structure connections between courses, don’t overlook important clinical moments and insights.” “It’s important to capitalize on the diversity of the background and expertise of our class.” “You reinforce effective teamwork and leadership modeling at each opportunity.” Comments of Student Advisory Group Members

14
Ferranti/White’s Fine Few

15
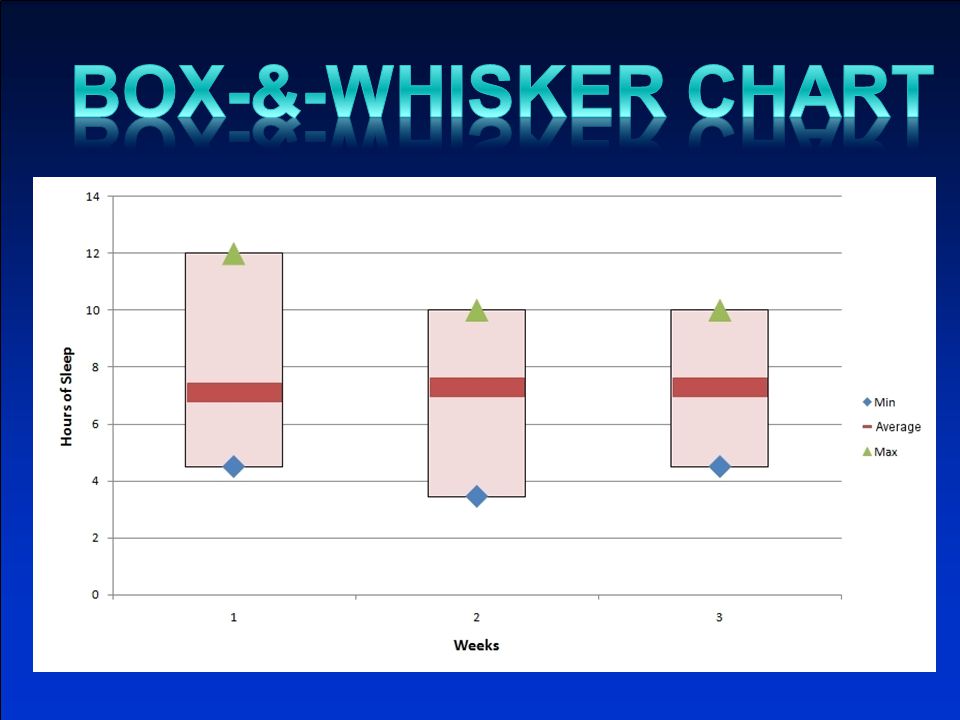
Inadequate sleep was a concern of the entire group Group members expressed feelings of fatigue, difficulty concentration and were aware of the detrimental effects of sleep deprivation on health After initial assessment, an inconsistent sleep duration pattern was noticed, measured in the course of a week

16
Sleep deprivation can lead to or be an aggravating factor in depression, heart disease, hypertension, irritability, slurred speech, slower reaction times, tremors, and weight gain (http://www.sleep-deprivation.com/ articles/effects-of-sleep-deprivation/) Most studies of partial sleep deprivation have suggested that sleeping only 5-6 hours a night can lead to impairment (Weinger & Ancoli-Israel, 2002) The psychomotor effects of going without sleep for 24 hours are similar to that of acute alcohol intoxication (Weinger & Ancoli-Israel, 2002)
 Most studies of partial sleep deprivation have suggested that sleeping only 5-6 hours a night can lead to impairment (Weinger & Ancoli-Israel, 2002) The psychomotor effects of going without sleep for 24 hours are similar to that of acute alcohol intoxication (Weinger & Ancoli-Israel, 2002)")
17
Decreased sleep duration per night SchoolSchool Misc.Misc. Living situation IllnessIllness SocialSocialWork/JobWork/Job Assignments Role Transition Early class time Financial stress Stress r/t school work “Hanging out” late Television Telephone Computer Eating/CaffeineStress Hours Allergies Medication TemperatureInsomnia Noise Trouble falling asleep Light

18
Increase in stress level correlates to a decrease in perceived sleep quality (Daon et al., 2004) People who use problem-based coping strategies to deal with stress have an increase in sleep (Daon et al., 2004) Both the amount and quality of sleep should be considered when it comes to getting enough sleep (Blachowicz & Letizia, 2006) One recommendation is to adjust the environment in a way that is favorable to sleeping (Blachowicz & Letizia, 2006) Exposure to bright light in the evening can shift the circadian rhythm to a later time, thus increasing sleep latency (Cajochen et al., 1998) Exposure to bright light upon waking shifts the circadian rhythm to an earlier time, which in turn improves sleep latency in the evening (Cajochen et al., 1998)
 People who use problem-based coping strategies to deal with stress have an increase in sleep (Daon et al., 2004) Both the amount and quality of sleep should be considered when it comes to getting enough sleep (Blachowicz & Letizia, 2006) One recommendation is to adjust the environment in a way that is favorable to sleeping (Blachowicz & Letizia, 2006) Exposure to bright light in the evening can shift the circadian rhythm to a later time, thus increasing sleep latency (Cajochen et al., 1998) Exposure to bright light upon waking shifts the circadian rhythm to an earlier time, which in turn improves sleep latency in the evening (Cajochen et al., 1998)")
19
Week 1 Intervention – Limiting TV, cell phone, computer use prior to bedtime Week 2 Intervention – Dim lights in home at least 30 minutes prior to bedtime; attain exposure to bright light within 10 minutes after awakening

21
Group members gained further awareness on the consequences of inconsistent sleep duration patterns Group members became more aware of ways to improve sleep duration Sleep consistency amongst the group members did not improve significantly Group members were motivated to discuss methods to improve the interventions

22
It is important to look at the data findings from all perspectives, to avoid any misleading conclusions It may be necessary to delete, revise or combine interventions to reach maximum effectiveness The interventions might have been more effective if there was more control regarding certain other influences, i.e. school factors Change is difficult, even when one has the best of intentions

23
QSEN Competencies in QI Project (Examples) Safety Analyze the usefulness of national quality and safety resources and initiatives for guiding clinical practice Teamwork Analyze how professional and clinical team performance affects quality of patient care and safety Identify and practice a set of effective strategies for communication and resolving conflict Quality Improvement Design a small test of change Describe processes for identifying opportunities for improving quality and safety. Describe processes and tools for analyzing quality and safety problems and implementing and evaluating improvements.

24
Faculty Experience “ I initially thought Role Transition (clinical course) already incorporated QSEN competencies – but once the concepts were highlighted consistently and clearly by framing them in a common language and reinforcing them between Role Transition and Professional Development, it became obvious (in group discussion and journaling) that students were noticing quality and safety indicators in clinical practice in more specific and meaningful ways.” “Clinical preceptors involved in QI in practice settings were enthusiastic that students knew about QI and were able to engage students in meaningful dialogue about specific initiatives on their units.” Corrine Abraham, MN, RN Coordinator, Role Transition
 already incorporated QSEN competencies – but once the concepts were highlighted consistently and clearly by framing them in a common language and reinforcing them between Role Transition and Professional Development, it became obvious (in group discussion and journaling) that students were noticing quality and safety indicators in clinical practice in more specific and meaningful ways. Clinical preceptors involved in QI in practice settings were enthusiastic that students knew about QI and were able to engage students in meaningful dialogue about specific initiatives on their units. Corrine Abraham, MN, RN Coordinator, Role Transition")
25
Lessons Students: “QI exercise was great!” Important to build awareness – what you will see, what it means e.g. Students did not recognize PDSA and tools in clinical practice until we brought it to their attention Pick points of intersection carefully and efficiently - too much intersection can get confusing especially in the beginning Need to move some QSEN KSAs earlier in curriculum – quality & safety, teamwork Recognize need for incremental growth, eg. Communication, conflict management

26
Critical Success Factors Comprehensive Model Curriculum Design, Student Involvement, Faculty Development, Clinical Partners Faculty enthusiasm - willing to experiment - willing to learn along with students Clinical course coordinators Lead coordinator role - keep all the pieces integrated

27
Outcomes 100 graduates with basic competencies in teamwork, QI and knowledge of national quality initiatives. 30+ faculty familiar with QSEN competencies; practice with many Experience with integrated framework for teaching QSEN Closer collaboration with Clinical Partners, shared curriculum materials, potential for IHI projects

28
Next Steps Curriculum Refinement Small modifications to junior year curriculum with similar model Experiment with earlier introduction to teamwork and quality Integration of simulation, team training Faculty Development and Ownership Shared strategies to embed QSEN in faculty thinking and culture

Similar presentations





 “.. Occurs when two or more professions learn with, from, and about each other to improve collaboration and the quality.>")












 October 14, 2011.>")
