Download presentation
Presentation is loading. Please wait.

1
Terry Rose PT, MS, DPT, FAAOMPT, Cert. MDT

2
Hando, Gill, Walker, Garber, “Short- and long-term clinical outcomes following a standardized protocol of orthopedic manual physical therapy and exercise in individuals with osteoarthritis of the hip: a case series” Journal of Manual and Manipulative Therapy, 2012, Vol. 20, No. 4. Objectives: Describe short- and long-term outcomes observed in individuals with hip osteoarthritis (OA) treated with a pre-selected, standardized set of best- evidence manual therapy and therapeutic exercise interventions.
 treated with a pre-selected, standardized set of best- evidence manual therapy and therapeutic exercise interventions..")
3
Results: “Numerical Pain Rating Scale (NPRS) scores improved from 4·3(±1·9) to 2·0(±1·9), hip flexion range of motion (ROM) improved from 99 degrees (±10·6) to 127 degrees (±6·3) and hip internal rotation ROM improved from 19 degrees (±9·1) to 31 degrees (±11·5).” “Improvements in HHS, NPRS, and hip ROM measures reached statistical significance (P<0·05) at 8-weeks and remained significant at the 29-week follow-up.” “Mean changes in NPRS and HHS scores exceeded the minimal clinically important difference (MCID) at 8-weeks and for the HHS scores alone at 29 weeks. The 8 and 29 week mean Global Rating of Change scores were 5·1(±1·4) and 2·1(±4·2), respectively.” Discussion: “Improved outcomes observed following a pre-selected, standardized treatment protocol were similar to those observed in previous studies involving impairment-based manual therapy and therapeutic exercise for hip OA. Future studies might directly compare the two approaches.”
 and 2·1(±4·2), respectively. Discussion: Improved outcomes observed following a pre-selected, standardized treatment protocol were similar to those observed in previous studies involving impairment-based manual therapy and therapeutic exercise for hip OA. Future studies might directly compare the two approaches. .")
4
Manual Therapy Protocol Patient supine at the edge of table Therapist next to patient on stool. Optional to place one knee on plinth for leverage. Belt placed around proximal femur of patient and around ischial tuberosities of therapist. Distract hip joint inferiorly by shifting hips posteriorly while using hand to bring patient into hip flexion. Hip Flexion With Caudal (inferior) Glide Improve Hip Flexion
 Glide Improve Hip Flexion.")
5
Manual Therapy Protocol Long Axis Distraction Patient in supine, may hold onto table to avoid sliding Place hip in slight flexion/ abduction. PT grasps pt. with both hands above the malleoli Impart distraction by shifting weight posteriorly Improve all Hip Motions

6
Manual Therapy Protocol Posterior – Anterior Mobilization Pt. prone with hip placed in flexion/ abduction/ external rotation Place towel roll under pt. knee PT kneels on table while using left knee to prevent the pt. LE from internally rotating Impart anterior mobilization through greater trochanter Progress by bringing hip further into flex./ abd./ ER and repeat Improve Hip Extension

7
Manual Therapy Protocol Iliopsoas Stretch Place pt. supine with buttocks at edge of table (in Thomas test position) Flex pt. non involved hip while extending the involved side PT holds opposite LE in flexion and while extending other LE until stretch is felt in the hip flexors Improve Hip Extension
 Flex pt. non involved hip while extending the involved side PT holds opposite LE in flexion and while extending other LE until stretch is felt in the hip flexors Improve Hip Extension.")
8
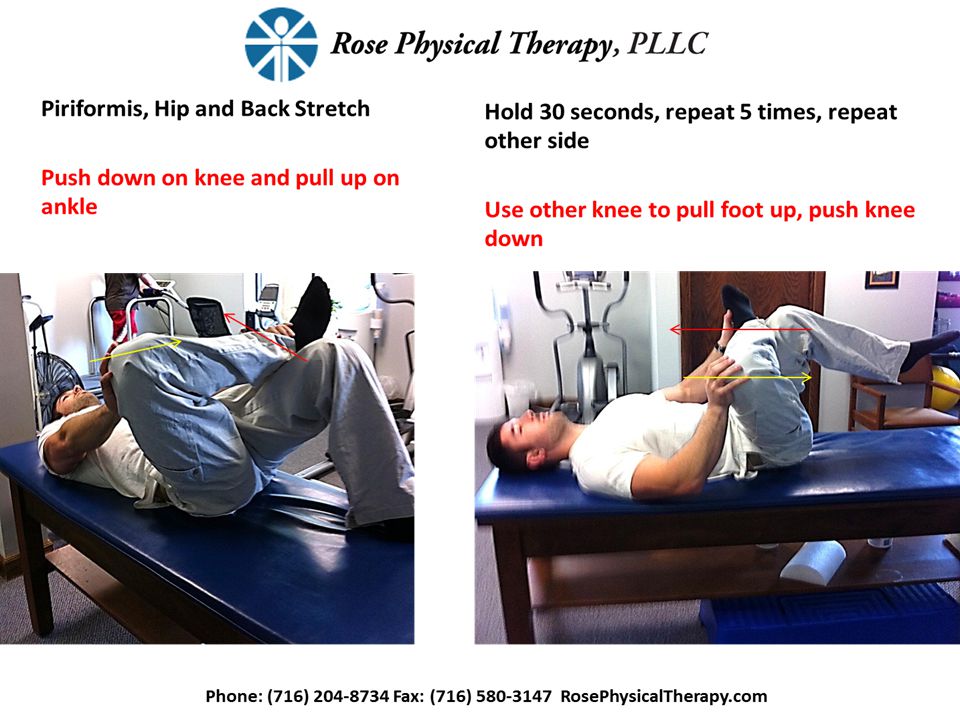
Manual Therapy Protocol Piriformis Stretch Pt. in supine PT flexes and externally rotates pt. involved hip until stretch is felt in the buttocks Progress with increased flex./ ER/ and adduction Improve Hip Internal Rotation and Stretch Hip Joint Capsule

9
Manual Therapy Protocol Internal Rotation with Distraction Pt. placed in supine PT places belt around pt. proximal femur and therapists ischial tuberosities PT flexes pt. hip to 90 Impart lateral distraction by shifting weight posteriorly Following distraction, using AAROM internally rotate pt. hip Improve Hip Internal Rotation

10
Exercise Program Knee to chest stretch Lie supine Grasp the front of your knee as shown. Pull your knee to your chest until you feel a stretch in your buttock and posterior thigh. Hold stretch for 30 seconds or more. Perform every day for 3 sets of 30 seconds. Glute Max and Hip Capsule Stretch

14
Exercise Program Hip Abduction Strengthen Glute Med Lie on your left side. Use your right lateral hip muscles to lift leg towards the ceiling. Do not let pelvis rotate posteriorly. Hold for 1-2 seconds at the top and return to starting position. Perform every other day for 3 sets of 12 reps.

15
Exercise Program Hip Flexor Stretch Stretch Iliopsoas, Rectus Femoris, ITB Lie with your buttock at the edge of the table. Grasp the front of your knee as shown and pull your knee to your chest Let your opposite leg relax and fall towards ground until you feel a stretch in the front of your thigh and groin. Hold stretch for 30 seconds or more. Perform every day for 3 sets of 30 seconds.

17
Selkowitz, Beneck, Powers “Which Exercises Target the Gluteal Muscles While Minimizing Activation of the Tensor Fascia Lata? Electromyographic Assessment Using Fine-Wire Electrodes”J Orthop Sports Phys Ther. 2012 Nov 16 Background: Abnormal hip kinematics (i.e. excessive hip adduction and internal rotation) has been linked to certain musculoskeletal disorders. The TFL is a hip abductor but also internally rotates the hip. As such, it may be important to select exercises that activate the gluteal hip abductors while minimizing activation of TFL. Conclusion: If the goal of rehabilitation is to preferentially activate the gluteal muscles while minimizing TFL activation, then the clam, mini squat side-step with band, unilateral bridge, and both quadruped hip extension (straight leg and bent knee) exercises would appear to be most appropriate
 has been linked to certain musculoskeletal disorders. The TFL is a hip abductor but also internally rotates the hip. As such, it may be important to select exercises that activate the gluteal hip abductors while minimizing activation of TFL. Conclusion: If the goal of rehabilitation is to preferentially activate the gluteal muscles while minimizing TFL activation, then the clam, mini squat side-step with band, unilateral bridge, and both quadruped hip extension (straight leg and bent knee) exercises would appear to be most appropriate.")
Similar presentations