Download presentation
Presentation is loading. Please wait.

1
Melanocytic Nevi and Neoplasms Andrew’s chapter 30 JoAnne M. LaRow, D
Melanocytic Nevi and Neoplasms Andrew’s chapter 30 JoAnne M. LaRow, D.O.

2
Epidermal Melanocytic Lesions
Normal melanocte occurring at the epidermal-dermal junction is a dendritic secretory cell supplying all normal melanin to skin These cells contain pigment granules (melanosomes) Stain with dopa reaction and silver stains Melanocytes of the epidermis transfer the melanosomes through their thin dendritic processes into surrounding keratinocytes Size and number in keratinocytes determine pigmentation of skin and hair
 Stain with dopa reaction and silver stains. Melanocytes of the epidermis transfer the melanosomes through their thin dendritic processes into surrounding keratinocytes. Size and number in keratinocytes determine pigmentation of skin and hair.")
3
Nevus Spilus Pigmented, light brown or tan macule, varied diameter, speckled with smaller, darker-colored macules or papules Lower extremity & trunk frequently May be <1cm or large May follow a dermatomal distribution when large Usually they do not cross the midline

4
Nevus Spilus When these nevi follow a dermatomal distribution they may be referred to as a zosteriform, or sometimes a speckled lentiginous nevus When nevus spilus is present with a nevus flammeus = phakomatosis pigmentovascularis phakomatosis pigmentokeratotica= a syndrome of organoid nevus with sebaceous differentiation, hemiatrophy with muscular weakness & other neurologic findings & speckled lentiginous nevus

5
Nevus Spilus -The darker speckles usually contain nevus cells
-Due to this melanoma may arise in the with greater frequency than in normal skin -However, removal is not necessary -Removal by Q-switched ruby laser has been reported effective

6
Lentigo Simplex Usually arise in childhood but can arise anytime
Sharply defined, rounded, brown or black macules found anywhere on body or mucosa Histologically shows elongation of rete ridges, increase in number of melanocytes in basal layer, increase of melanin in both melanocytes, and basal keratinocytes, and melanophages in the upper dermis No therapy is needed/ there is no predisposition to neoplastic change

7
Solar Lentigines Commonly called “liver spots” Hyperpigmented macules
May evolve into sk’s or lichenoid keratoses Tx=liquid nitrogen, laser May recur, as a lentigo maligna or lentigo maligna melanoma Be aware-oral methoxsalen photochemotherapy or frequent tanning salons may develop lentigines on non-sun-exposed areas and these may show cellular atypia

8
Penile and Vulvar Melanosis
Localized pigmentary alterations Most often show basilar hyperpigmentation May appear in large patches or in smaller, well-demarcated lesions Present on the penis or in women on the labia majora

9
Bannayan-Riley-Ruvalcaba Syndrome
Rare, AD disorder that manifests in childhood 80% of the pts are male Characterized by genital lentiginosis, macrocephaly, motor and speech delay, mental retardation, lipomas, hemangiomas, verruca vulgaris, and many types of facial papules

10
Multiple Lentigenes Syndrome
Lentigines are dark brown macules 1-5 mm. Preponderance on the trunk Multiple generalized lentigines may occur with a number of associated signs as an dominantly inherited syndrome l

11
LEOPARD Syndrome Leopard syndrome = acronym for lentigines, electrocardiographic abnormalities, ocular hypertelorism, pulmonary stenosis, abnormalities of genitalia, retardation of growth, and deafness

12
Moynahan Syndrome Multiple lentigines Congenital mitral stenosis
Dwarfism Genital hypoplasia Mental deficiency

13
Centrofacial Lentiginosis
Characterized by lentigines on the nose, and adjacent cheeks Sometimes associated with status dysraphicus, multiple skeletal anomalies, and CNS disorders Spares the mucous membranes Onset is first years of life

14
Inherited Patterned Lentiginosis in Blacks
AD- reportedly, 10 light-complexioned black patients who developed numerous lentigines in infancy or early childhood Distribution is central face, lips, with variable involvement of dorsal hands and feet, elbows, and buttocks Sparing of mucous membranes and no internal abnormalities

15
Carney’s Syndrome AKA NAME syndrome or LAMB syndrome
Characterized by cardiocutaneous myxomas, lentigines, blue nevi, and endocrine anomalies

16
Peutz-Jeghers Syndrome
AD Pigmented macules on the lips, oral mucosa, perioral acral areas Gastrointestinal polyps, especially prominent in the jejunum are seen

17
Melanoacanthoma uncommon lesion, a benign epidermal melanocytic neoplasm, occurring on the head Resembles a pigmented sk or a pigmented BCC Predominantly seen in white men > 60 yrs

18
Cellular Nevi Begins to appear in first yrs of life, increase in prevalence and number over the next two decades, after which there is a steady decline Females tent to have more than males Less common in sun-protected areas Maximum number is at age yrs, the average number is 40 Sun exposure increases the number of nevi in the exposed skin Eruptive nevi are rare, but may occur after severe bullous disease such as TEN, EM, or severe sunburn, Addison’s disease or immunosuppresion

19
Junctional Nevi Nevi begin as small, flat, pigmented macules = junctional nevi A smooth, hairless, light to dark brown macule, varying in size from 1 –6 mm Occurs on any site, especially on palms, soles, scrotum During adolescence some will become compound or intradermal It is characterized by single melanocytes, or theques of them in the lower epidermis

20
Compound Nevus The compound nevus is one that is still manifesting so-called junctional activity( accumulation of melanocytes in theques in the epidermis) but has formed structure of a cellular nevus in the dermis as well
 but has formed structure of a cellular nevus in the dermis as well.")
21
Junctional Nevi Nevi begin as small, flat, pigmented macules = junctional nevi A smooth, hairless, light to dark brown macule, varying in size from 1 –6 mm Occurs on any site, especially on palms, soles, scrotum During adolescence some will become compound or intradermal It is characterized by single melanocytes, or theques of them in the lower epidermis

22
Compound Nevus The compound nevus is one that is still manifesting so-called junctional activity( accumulation of melanocytes in theques in the epidermis) but has formed structure of a cellular nevus in the dermis as well
 but has formed structure of a cellular nevus in the dermis as well.")
23
Compound Nevus An 8-mm, well-circumscribed, symmetric, uniformly colored papule A lesion of this size could be an acquired nevus or a small congenital pattern nevus

24
Compound Nevus Nests of nevus cells in the epidermis overlying a dermal component of orderly nevus cells

25
Compound Nevus Acral type-thickened basket weave stratum corneum shows that it is an acral site Nevus is small and symmetric, and shows both a junctional and superficial dermal component The nests in the papillary dermis are small, orderly, and lack atypia. The epidermal component may show a few pagetoid cells

28
Intradermal Nevus a compound nevus in which junctional activity- that is, theques of melanoctyes in the epidermis or at the dermal epidermal junction- has ceased, and all the nevus cells are in the dermis

29
Intradermal Nevus Low power-as in junctional nevi , dermal nevi contain nevus cells that are recognized at this power by tendency to be arranged in nests High power- at the base of this dermal nevus the melanocytic cells resemble neural structures( neurotization)
")
31
Balloon Cell Nevus A pigmented nevus, varying in size from 1 –5 mm, usually occurring on the head, neck, and trunk. They are clinically indistinguishable from ordinary pigmented or nonpigmented nevus Histologically, the lesions are composed of peculiar vesicular cells that appear to be foamy and form large pale polyhedral balloon cells that may be multinucleated giant cells in addition to nevus cells. Not considered potentially malignant, and treatment is same as other nevi

32
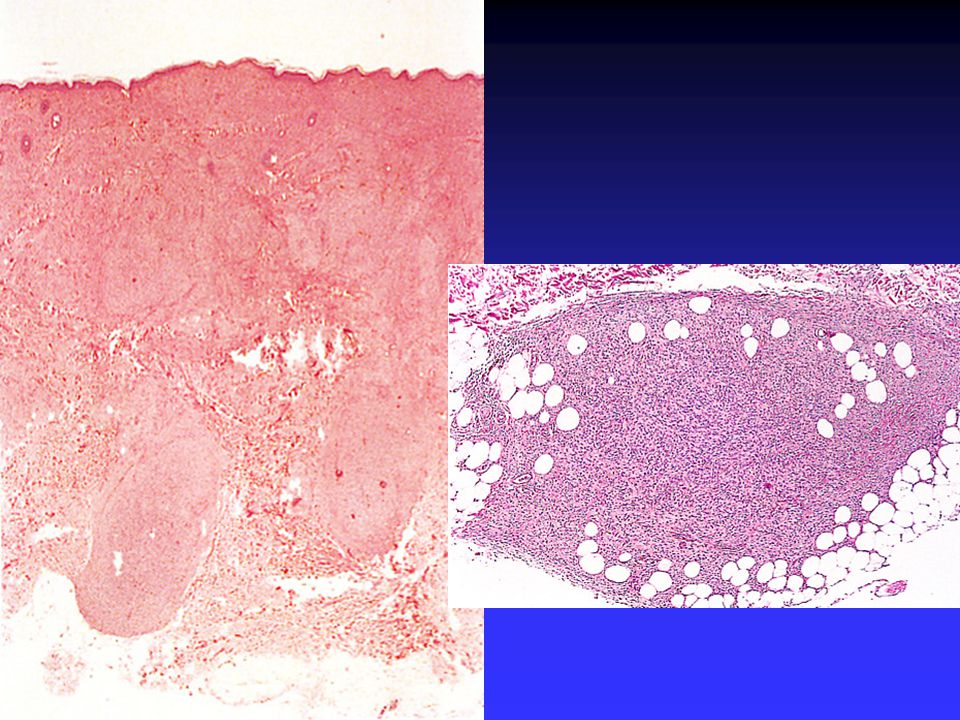
Halo Nevus AKA Sutton’s nevus, perinevoid vitilgo, & leukoderma acquisitum centrifugum A pigmented nevus with surrounding depigmented zone Nevus is usually compound or intradermal May be single or multiple Usually on the trunk Mostly develop in teenagers No tx indicated- central nevus disappears with time leukodermic area will usually repigment with time

33
Halo Nevus The nevus architecture is obscured by a dense lymphocytic infiltrate Lymphocytes infiltrate among the dermal nevus cells, which eventually degenerate and disappear

36
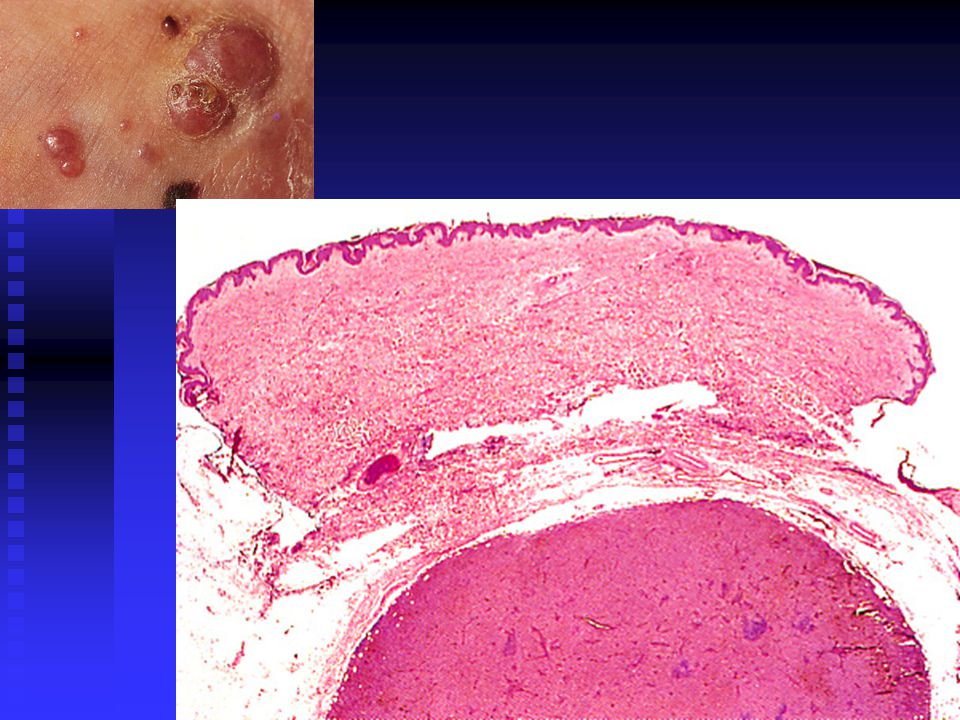
Congenital Nevocytic Nevus
Giant Pigmented Nevus (Giant hairy nevus, bathing trunk nevus) Characterized by a large, darkly pigmented hairy patch in which smaller, darker patches are interspersed or present as small satellite lesions Skin may be thickened or verrucous Has a tendency to follow a dermatome distribution Trunk favored site
 Characterized by a large, darkly pigmented hairy patch in which smaller, darker patches are interspersed or present as small satellite lesions. Skin may be thickened or verrucous. Has a tendency to follow a dermatome distribution. Trunk favored site.")
37
Congenital Nevocytic Nevus
Giant hairy nevi are present at birth and grow proportionally to the site of the body where they are located By definition they are >20cm When a large congenital nevus involves the axial skin, there may be an associated neurocutaneous melanocytosis Incidence of melanoma developing is 3% to 7%

38
About 40% of the malignant melanomas seen in children occur in large congenital nevi -risk is greatest for axial lesions If neurocutaneous melanosis is present (which can be detected by MRI), the risk of dying at a young age is high secondary to hydrocephalus or leptomeningeal melanoma Most recommend total surgical excision and resurfacing autografts Alternative treatments-dermabrasion, curettage, and laser ablation- are designed to eliminate some of the nevus cells, with theoretic lowering of the risk of melanoma CNN
, the risk of dying at a young age is high secondary to hydrocephalus or leptomeningeal melanoma. Most recommend total surgical excision and resurfacing autografts. Alternative treatments-dermabrasion, curettage, and laser ablation- are designed to eliminate some of the nevus cells, with theoretic lowering of the risk of melanoma. CNN.")
39
Small and Medium-sized Congenital Nevocytic Nevus
Small - < 1.5 cm in greatest diameter Medium- > 1.5 cm but < 20 cm Found in 1% of newborns Half eventually become hairy Data to determine the incidence of melanoma are still being gathered Excision is recommended for lesions of the hairy scalp, or those of great cosmetic concern or nevi with unusual clinical features

40
Epitheliod and Spindle-Cell Nevus(benign Juvenile Melanoma, Spitz Nevus)
")
41
Spitz Nevus A smooth-surfaced, raised, round, slightly scaly, firm papule with distinctive pink, brownish red, or purplish red color Typically, firm,rosy papule on the face, especially on the cheek 3 – 10 mm in diameter Female predominance Should be completely excised

42
Spitz Nevus A variant of the compound nevus
Epidermal irregular acanthosis, pseudoepitheliomatous hyperplasia, and thinning of the epidermis Nevus cells are pleomorphic, but mostly spindle-shaped (fusiform), or polygonal (epithelioid) cells
, or polygonal (epithelioid) cells.")
43
Spitz Nevus Giant cells with eosiophilic cytoplasm and a large nucleus may be seen Multinucleated giant cells are seen less frequently No difference between childhood and adult lesions Eosinophilic globules with fibrillar microstructure (Kamino bodies) are found in 60% - 85% of SN May also be present in melanomas (12&) and compound nevi(8%), but are fewer and smaller in SN
 are found in 60% - 85% of SN. May also be present in melanomas (12&) and compound nevi(8%), but are fewer and smaller in SN.")
45
Spitz Nevus * Immunohistochemical staining for MIB-1 and bcl-2 will distinguish most Spitz nevi from melanoma;melanomas are immunoreactive, whereas Spitz nevi are not * Differential diagnosis-pyogenic granuloma, mastocytoma, juvenile xanthogranuloma, or melanoma

46
Dysplastic Nevus Variegated tan, brown, pink coloration
Pink hues seen in macular portion Macular portion always present, may comprise entire lesion, but frequently surrounds a papular center Generally larger than are common nevi, usually 5 – 12mm, with irregular borders

47
Dysplastic Nevus Syndrome
Around 1978 Lynch et al recognized an autosomal dominant inheritance pattern in families with unusual nevi and multiple melanomas-initially described by Clark et al as B-K mole syndrome- then named familial atypical multiple mole-melanoma syndrome Now termed dysplastic nevus syndrome (DNS) Pts with dysplastic nevi send at least two blood relatives with dysplastic nevi and melanoma have the worst prognosis with possibly 100% lifetime risk of melanoma
 Pts with dysplastic nevi send at least two blood relatives with dysplastic nevi and melanoma have the worst prognosis with possibly 100% lifetime risk of melanoma.")
48
Dysplastic Nevus Syndrome-Genetics
25% -33% of pts have germline mutations on chromosome 9p in the CDKN2A tumor-suppressor gene-which encodes for an inhibitor of a cyclindependent kinase 4 (CDK4) that functions to suppress proliferation In these pts with mutations that impair the function of the p16 suppressor protein, referred to as the p16M alleles, there is a concomitant predisposition to pancreatic cancer
 that functions to suppress proliferation. In these pts with mutations that impair the function of the p16 suppressor protein, referred to as the p16M alleles, there is a concomitant predisposition to pancreatic cancer.")
49
Dysplastic Nevus Syndrome
Dysplasic nevi occur commonly in pts without a personal or family history of melanoma-5% -20% of pts having at least one clinically dysplastic nevus This is important for (1) histologic evaluation is neede (2) a careful history and evaluation of family members (3) they provide another risk factor for melanoma predisposition
 histologic evaluation is neede (2) a careful history and evaluation of family members (3) they provide another risk factor for melanoma predisposition.")
50
Dysplastic Nevus Syndrome
Histologic features as per an NIH consensus- basilar melanocytic hyperplasia with elongation of rete ridges; spindle-shaped or occasionally, epithelioid melanocytes arranged horizontally and aggregating in nests that fuse with adjacent rete ridges; lamellar and concentric superficial dermal infiltrate; cytologic atypia, usually present but not essential for diagnosis

51
Dysplastic Nevi Patients with dysplastic nevi and a positive family or personal history of melanoma, physician examination every 3 – 6 months Excision of those nevi that change clinically Photographs with measured scale is useful

52
Melanoma Originate from melanocytes at epidermal-dermal junction
Half will develop in preexisting nevi Prolonged, non invasive, horizontally oriented growth phase When tumor nodule develops the vertical growth phase is occurring and the risk of metastatic disease increases dramatically

53
Melanoma One in 80 Americans will develop melanoma
Incidence is low until after puberty Children may present with congenital melanoma or acquired melanoma Congenital melanoma may occur because of transplacental transmission, as a primary intrauterine lesion, as a melanoma from a congenital nevus in utero, or as prenatal metastatic lesions from neurocutaneous melanosis all of these have a poor prognosis Melanoma

54
Diagnosis of Melanoma - surgical excision is the best method
-for larger lesions an incisional or punch biopsy, deep enough is considered good practice -when melanoma is suspected in a melanotic freckle or a giant pigmented nevus, biopsy should be done through the thickest and most atypical area and multiply sectioned to find thickest area of involvement

55
Histologic diagnosis:
-presence of mitoses -inflammatory reaction composed of lymphocytes and possibly plasma cells -dermoepidermal junctional activity -absence of dermal stroma

56
Histologic diagnosis:
-a moderately brisk tumor-infiltrating lymphocyte response is present around the nodule - the cells in the nodule are large epithelioid melanoma cells that have abundant cytoplasm and large irregular nuclei with prominent nucleoli with numerous mitoses

58
Melanoma Metastasis-usually manifested by pigmented nodules appearing around the site of the excision Early remote metastases occur via lymphatics and regional lynphadenopathy may be the first sign

60
Melanoma > 50 benign nevi Presence of large congenital nevus
Presence of clinically dysplasic nevus Mutations in the p16-CDK4 Immunodefiency syndromes-acquired or genetic PUVA treatments Xeroderma pigmentosum Use of tanning lamps Levodopa therapy for Parkinson’s disease has been implicated in 19 case reports by Rampen

61
Melanoma There are four recognized clinicohistologic types:
1.) Lentigo maligna (melanoma in situ, noninvasive melanoma) 2.) Superficially spreading melanoma 3.) Acral-lentiginous melanoma 4.) Nodular melanoma
 Lentigo maligna (melanoma in situ, noninvasive melanoma) 2.) Superficially spreading melanoma. 3.) Acral-lentiginous melanoma. 4.) Nodular melanoma.")
62
Melanoma *Pedunculated, polypoidal melanomas, inflammatory melanomas, amelanotic melanomas, and hyperkeratotic and verrucous melanomas are clinical findings *At a microscopic level-desmoplastic, neurotropic, myxoid, balloon cell, and signet cell patterns are seen

63
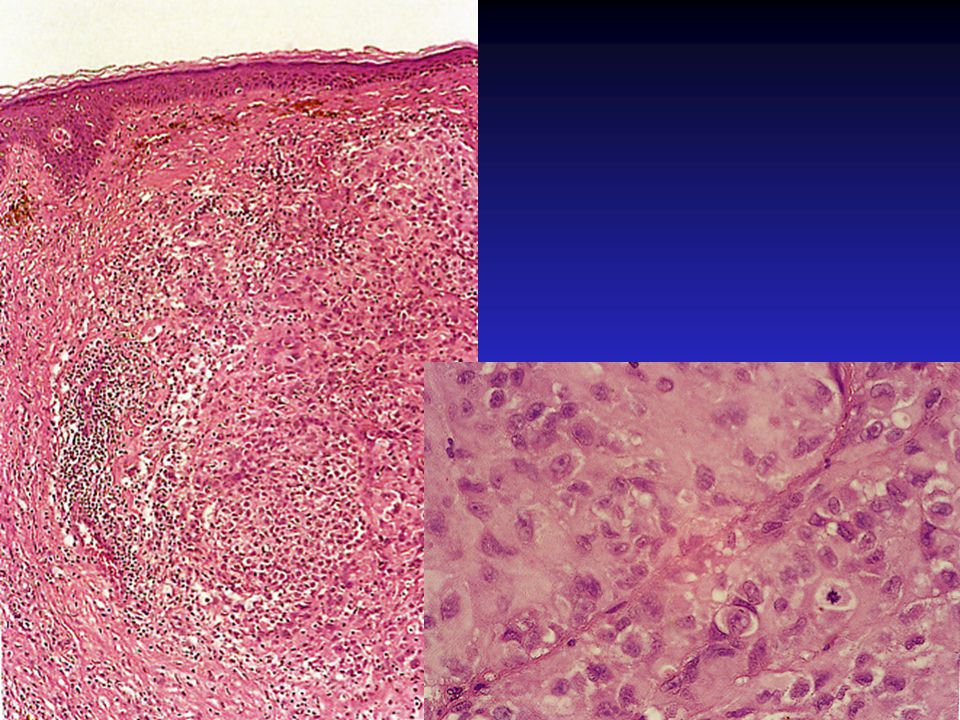
Lentigo maligna(melanoma in situ, noninvasive melanoma)
Begins as a tan macule that extends peripherally, with gradual uneven darkening, over several years After a radial growth of 5 to 20 years, vertically growing melanoma usually develops within it A palpable nodule within the original macule is the best evidence that a lentigo maligna melanoma has occurred Equal incidence in men and women Usually yrs Usually on chronically sun-damaged skin, most often on the face Accounts for 5% of all melanomas

64
Lentigo maligna(melanoma in situ, noninvasive melanoma)
")
65
Superficially spreading melanoma
In a study by Bolognia et al 5% of lesions with an eccentric foci of hyperpigmentation(a roundish area of brown or black 3mm or< and located peripherally) are melanomas arising from within a nevus It is necessary to ensure that the pathologist sections through the black dot to make this early diagnosis
 are melanomas arising from within a nevus. It is necessary to ensure that the pathologist sections through the black dot to make this early diagnosis.")
66
Acral-lentiginous melanoma
Acral-lentiginous melanoma lies midway between the lentigo maligna and the superficially spreading melanoma in respect to speed of horizontal growth into adjacent epidermis Subungual and mucosal lesions are in this category Account for 10% of all melanomas The most common type among Japanese, African American, Hispanics, and Native Americans Median age is 50 yrs with equal sex distribution

67
Melanoma- workup and follow-up
-establish a family history -thorough review of systems physical exam A consensus conference in 1992 concluded that a staging workup was not indicated for melanomas below 1.0 mm thickness Many physicians obtain a CXR and an LDH As in the initial workup, more information and a consensus statement would help to establish indications for testing Consultation with an oncologist is worthwhile

68
Melanoma-treatment -early diagnosis and excision
-margin of 0.5 to 1.0 cm for melanoma in situ -1.0 cm margin for melanomas < 2.0 cm thick -3.0 cm margin for those thicker than 2.0 mm -Zitelli et al recommended wider margins for melanomas of the head, neck, hands, and feet- they recommend a minimum surgical margin of 1.5 cm, unless Mohs’ micrographic surgery is use - ELND is controversial and therefore intraoperative lymphatic mapping is used

69
Melanoma-treatment -high-dose interferon alfa-2b therapy has been used, however efficacy is equivocal and toxicity high -adjuvant interferon alfa-2a treatment has been reported to diminish the occurrence of mets and prolong disease free survival in pts with melanoma > 1.5 mm thick -chemotherapy is not effective -Adoptive immunotherapy with lymphokine-activated killer cells + interleukin-2, or high –dose into leukin-2 alone is also toxic, some patients are responsive -perfusion chemotherapy has been used for extremity melanoma and has almost eliminated the need for amputation

70
Dermal Melanocytic Lesions
At birth, melanocytes may be present in the dermal portion of the skin of the scalp, the backs of the hands, and the sacrum These are large ameboid cells that normally disappear shortly after birth

71
Mongolian Spot Bluish gray macule of varying size from 2-8 cm
Occurs typically in the sacral area of the newborn 80-90% of Asians, Southern Europeans, American blacks, and Native Americans Multiple spots may be situated in other locations

72
Mongolian Spot Multiple spots occurring in a widespread distribution have been termed generalized dermal melanocytosis or dermal melanocytic hamartomas If associated with a nevus flammeus- phakomatosis pigmentovascularis

73
Nevus of Ota Aka nevus fuscocerulleus opthalmaomaxillaris
Usually present at birth , especially if the patient is going to have ocular involvement May have involvement of the conjunctiva and the skin about the eye On the skin brown, slate gray, or blue-black macules grow slowly larger and deeper in color 80% occur in women; 5% are bilateral Usually a benign lesion malignant melanoma may occur Most common location is the choroid Glaucoma may occur

74
Nevus of Ito Aka nevus fuscoceruleus acromiodeltoideus
Has the same features as nevus of Ota except that it occurs in the distribution of the posterior supraclavicular and lateral cutaneous brachial nerves It involves the shoulder, side of the neck, and supraclavicular areas Tx –Q-switched ruby laser are dramatic

75
Blue Nevus Two types: 1.) Blue nevus of Jadassohn-Tiche (common blue nevus) 2.) Cellular blue nevus
 Blue nevus of Jadassohn-Tiche (common blue nevus) 2.) Cellular blue nevus.")
76
Blue Nevus Within the dermis there is a poorly defined but symmetric spindle cell proliferation that is dark brown in color No significant change in the overlying dermis The spindled heavily pigmented cells encircle collagen bundles in the reticular dermis, a pattern also seen in dermatofibromas The lesion is composed of elongate cells that are heavily pigmented and show prominent pigmented dendrites

77
Blue Nevus of Jadassohn-Tiche
The typical common blue nevus or nevus ceruleus Steel-blue nodule that begins early in life Slow growing Rarely reaches 2-10mm Occurs most frequently on the dorsal hands, feet, forearms, shins, face, and the buttocks

78
Cellular Blue Nevus Large, firm, blue or blue-black nodule
Frequently seen on the buttock and sacrococcygeal region Occasionally present at birth Seen in women 2.5 times as frequently as men Average age is 40 Uncommonly these invade underlying structure such as the skull in scalp lesions

79
Cellular Blue Nevus Frequently large and involve a good part of the dermis and extending deeply as tonguelike aggregates of tumor cells at the base of the lesion Involvement of the subcutaneous fat is common and does not imply a malignant diagnosis

81
Cellular Blue Nevus The cellular areas are composed of uniform spindled melanocytic cells with mor cytoplasm and larger nuclei than what is seen in common blue nevus. There are irregularly distributed collections of course melanin pigment within the cells

83
Epithelioid Blue Nevus
Newly described lesion Strong association with Carney’s complex (myxomas, spotty skin pigmentation, endocrine over activity, and schwannomas) Occur frequently on the head and neck, and are at times multiple They are darkly pigmented, domed, and less than 1 cm
 Occur frequently on the head and neck, and are at times multiple. They are darkly pigmented, domed, and less than 1 cm.")
84
Malignant Blue Nevus -Cellular blue nevus may rarely undergo malignant transformation into malignant melanoma -clinically increase in size, suddenly and ulceration -histologically, pleomorphism of nuclei, mitotic figures, and invasion of clusters of malignant cells into the deep dermis and fatty tissue -excision has been mainstay of treatment -Q-switched ruby laser has been reported to be successful - treatment of the malignant variety is the same as MM

Similar presentations