Download presentation
Presentation is loading. Please wait.

1
Direct Cost Survival Analysis of Treatment of Metastatic Colorectal Cancer Yu-Ning Wong 1, Neal J. Meropol 1, Daniel Sargent 2, Richard Goldberg 3, J. Robert Beck 1 1 Fox Chase Cancer Center, Philadelphia, PA; 2 Mayo Clinic, Rochester, MN; 3 University of North Carolina, Chapel Hill, NC

2
Abstract Background: Patients with metastatic colorectal cancer (mCRC) treated with 5Fluorouracil plus leucovorin (5FU/LV) have a median life expectancy (LE) of approximately12 months. The addition of irinotecan, oxaliplatin, bevacizumab and cetuximab has increased LE significantly. Although they have been widely adopted, little is known about the financial impact of these new drugs. Methods: Using published reports and aggregate data from NCCTG 9741, we developed a Markov Model which assumes forward progression through up to three lines of therapy compared to 5FU/LV alone. Patients who do not die of toxicity (tox) transition through supportive care prior to death. State changes are based on progression and dose-limiting toxicity. Drug costs are based on Average Sales Price. No other direct or indirect costs are included. Dose modifications for toxicity are defined as 80% of standard doses. Sensitivity analyses (SA) were performed on key variables. Results: LE, total drug costs, and cost-effectiveness (CE) ratios compared to single line-5FU/LV and FOLFOX for 9 commonly used treatement sequences are presented below. SA show that results are sensitive to progression rates,drug costs and length of time on supportive care. Changes in 1st line tox rates have a greater impact on final results than changes in 2nd or 3rd line therapy tox rates. Conclusions: Using drug costs alone, this model shows sequential combination therapy including all available agents to cost $2000-$2800K/week life gained ($100-$145K/year) compared to both 5FU/LV and FOLFOX. For clarity only 9 strategies are presented, but the model presented will contain multiple sequences consisting of 1-3 lines of therapy. Refined tox data, associated costs and quality of life adjustments are needed for realistic comparisons among specific combinations. Combination therapy may have CE ratios similar to other currently accepted intensive medical interventions. These data can help inform discussions of how the cost of care impacts patients, providers, and societies.
 transition through supportive care prior to death. State changes are based on progression and dose-limiting toxicity. Drug costs are based on Average Sales Price. No other direct or indirect costs are included. Dose modifications for toxicity are defined as 80% of standard doses. Sensitivity analyses (SA) were performed on key variables. Results: LE, total drug costs, and cost-effectiveness (CE) ratios compared to single line-5FU/LV and FOLFOX for 9 commonly used treatement sequences are presented below. SA show that results are sensitive to progression rates,drug costs and length of time on supportive care. Changes in 1st line tox rates have a greater impact on final results than changes in 2nd or 3rd line therapy tox rates. Conclusions: Using drug costs alone, this model shows sequential combination therapy including all available agents to cost $2000-$2800K/week life gained ($100-$145K/year) compared to both 5FU/LV and FOLFOX. For clarity only 9 strategies are presented, but the model presented will contain multiple sequences consisting of 1-3 lines of therapy. Refined tox data, associated costs and quality of life adjustments are needed for realistic comparisons among specific combinations. Combination therapy may have CE ratios similar to other currently accepted intensive medical interventions. These data can help inform discussions of how the cost of care impacts patients, providers, and societies..")
3
Background Since 1996, four new agents have been introduced for the treatment of mCRC Median life expectancy has increased from 12 months to greater than two years Survival of patients has improved due to the availability of treatment with 5FU/LV, irinotecan- and oxaliplatin- containing regimens. 1

4
Possible Treatment Sequences for Metastatic Colorectal Cancer First Line FOLFIRI or IFL + Bevacizumab Second Line FOLFOX Second Line Irinotecan Cetuximab Third Line FOLFOX Third Line Cetuximab+/- Irinotecan First Line FOLFOX Bevacizumab Second Line Irinotecan or FOLFIRI Third Line Cetuximab+/- Irinotecan First Line 5FU/LV + Bevacizumab Second Line FOLFOX Second Line Irinotecan or FOLFIRI Third Line Cetuximab+/- Irinotecan Third Line FOLFIRI or Irinotecan Fourth Line Cetuximab +/- Irinotecan Modified from the 2006 NCCN Guidelines for Treatment of Metastatic Colon Cancer. In addition, the option of single line cetuximab following irinotecan is included as a treatment sequence, in accordance with its FDA indication.

5
Treatment Related Costs have increased with Introduction of New Agents Cost of 6 months of commonly prescribed regimens for a 70 kg, BSA 1.7m2 patient 2 5FU/LV (Mayo Regimen, every 4 weeks)$96 Infusional 5FU/LV (De Gramont, every 2 weeks)$352 Capecitabine 1250 mg/m2 bid daily x14 days every 3 weeks$11,648 Irinotecan 350 mg/m2 every 3 weeks$30,100 Irinotecan 125 mg/m2 weekly x 4 every 6 weeks$21,500 FOLFIRI every 2 weeks$23,572 FOLFOX every 2 weeks$29,989 Bevacizumab every 2 weeks$23,897 Cetuximab, load followed by weekly dosing alone or with irinotecan$52,131
$96 Infusional 5FU/LV (De Gramont, every 2 weeks)$352 Capecitabine 1250 mg/m2 bid daily x14 days every 3 weeks$11,648 Irinotecan 350 mg/m2 every 3 weeks$30,100 Irinotecan 125 mg/m2 weekly x 4 every 6 weeks$21,500 FOLFIRI every 2 weeks$23,572 FOLFOX every 2 weeks$29,989 Bevacizumab every 2 weeks$23,897 Cetuximab, load followed by weekly dosing alone or with irinotecan$52,131")
6
Historical: $50,000/QALY (cost of one year of dialysis in the 1970s) Institute of Medicine Report 2003: Hidden Costs, Value Lost: Uninsurance in America:$160,000 for a year in perfect health NEJM 2005 Analysis of ICDs--$100,000/QALY 3 Issue of Cost Effectiveness is Debated
 Institute of Medicine Report 2003: Hidden Costs, Value Lost: Uninsurance in America:$160,000 for a year in perfect health NEJM 2005 Analysis of ICDs--$100,000/QALY 3 Issue of Cost Effectiveness is Debated")
7
Project Aim To measure the added costs and changes to life expectancy associated with newly developed combination regimens compared to 5FU/LV To examine what variables (ie progression, toxicity, drug costs, have the greatest impact of CE ratios)
")
8
Model Design Stable Disease on Front Line Rx T Stable Disease on Second Line Rx Supportive Care Dead P Stable Disease on Third Line Rx T T P P Change therapy Stylized Markov Model Patients enter at time of choice of front line therapy and transition from state to state at one week intervals. Ovals represent disease states. Rectangles represent decision points. Bold lines represent remaining in the current state for an additional cycle. Dashed lines represents returning to previous line of therapy after developing toxicity, either at current dose or with dose and/or schedule modification. Death is surrounded by multiple arrows to denote that it is possible to enter this stage from any point on the model. P T Legend: Progressive Disease on therapy Toxicity on therapy leading to either discontinuation or resumption of therapy Start Choice of Front Line Therapy

9
Model Assumptions 70 yo male 70 kg, 1.7 m2 Maximum of three lines of therapy Evaluated at weekly intervals Patients alive at the end of each interval get equal “credit” One dose reduction allowed prior to changing therapy Dose reduction/delay are translated into a 20% dose reduction Costs only include drug costs (ASP) Calculation of Probabilities Survival=e -rate*time Rate=(ln(0.5)/-Time in Months)/4.33 Rate=%/Number of weeks Probability=1-e -rate*time
 Calculation of Probabilities Survival=e -rate*time Rate=(ln(0.5)/-Time in Months)/4.33 Rate=%/Number of weeks Probability=1-e -rate*time")
10
Results

11
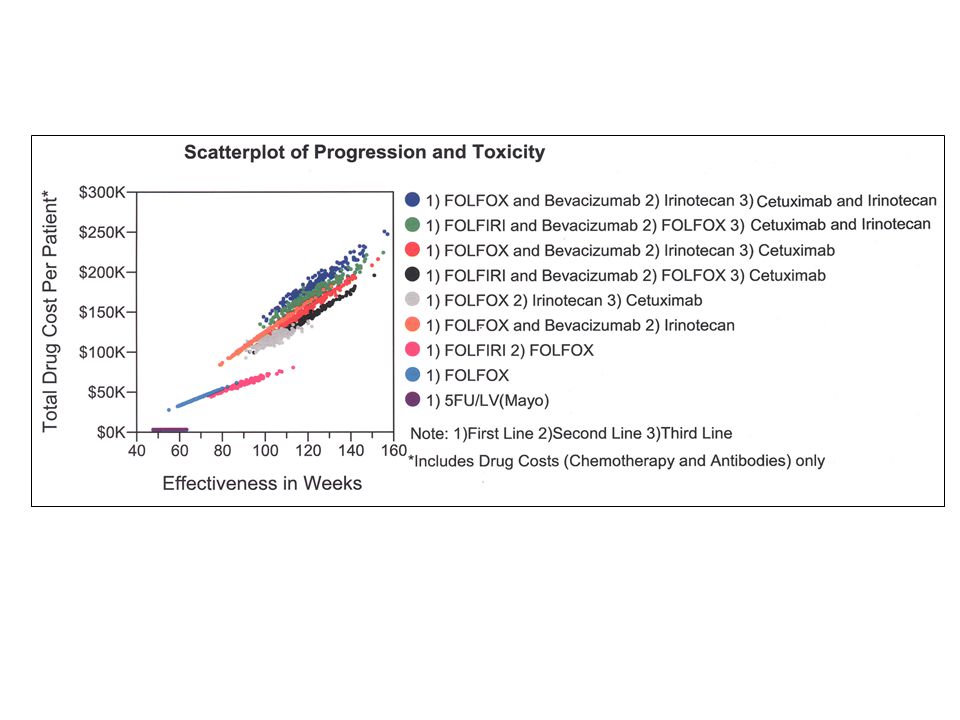
Cost Per Line of Therapy $96,200 $88,200 $96,200 $88,200 $41,300 $94,500 $33,600 $27,500 $17,600 $25,500 $17,600 $25,500 $16,700 $13,700 $19,300 $45,000 $41,800 $14,400 $13,700 $45,100 $184 $0$20,000$40,000$60,000$80,000$100,000$120,000$140,000$160,000$180,000 Regimen Drug Cost 1st Line2nd Line3rd LineSupp Care 1) FOLFOX and Bevacizumab 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 3) Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Cetuximab 1) FOLFOX 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 1) FOLFIRI 2) FOLFOX 1) FOLFOX 1) Mayo (5FU/LV) Relationship between life expectancy and cost of therapy
 FOLFOX and Bevacizumab 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 3) Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Cetuximab 1) FOLFOX 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 1) FOLFIRI 2) FOLFOX 1) FOLFOX 1) Mayo (5FU/LV) Relationship between life expectancy and cost of therapy")
12
Time on Treatment By Regimen 50 52 50 52 38 48 39 37 21 19 22 19 22 19 14 17 16 8 7 17 31 29 37 33 32 33 31 33 020406080100120140 Regimen Time on Treatment in Weeks 1st Line2nd Line3rd LineSupp Care 1) FOLFOX and Bevacizumab 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 3) Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Cetuximab 1) FOLFOX 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 1) FOLFIRI 2) FOLFOX 1) FOLFOX 1) Mayo (5FU/LV)
 FOLFOX and Bevacizumab 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 3) Cetuximab 1) FOLFIRI and Bevacizumab 2) FOLFOX 3) Cetuximab 1) FOLFOX 2) Irinotecan 3) Irinotecan and Cetuximab 1) FOLFOX and Bevacizumab 2) Irinotecan 1) FOLFIRI 2) FOLFOX 1) FOLFOX 1) Mayo (5FU/LV)")
13
Sensitivity Analyses (Two Way) This scenario varies cost of all four drugs with the toxicity of front line FOLFIRI/ Bevacizumab compared to baseline. This demonstrates that the incremental cost per life week gained compared to 5FU/LV is more sensitive to drug costs than toxicity profile of front line therapy.

14
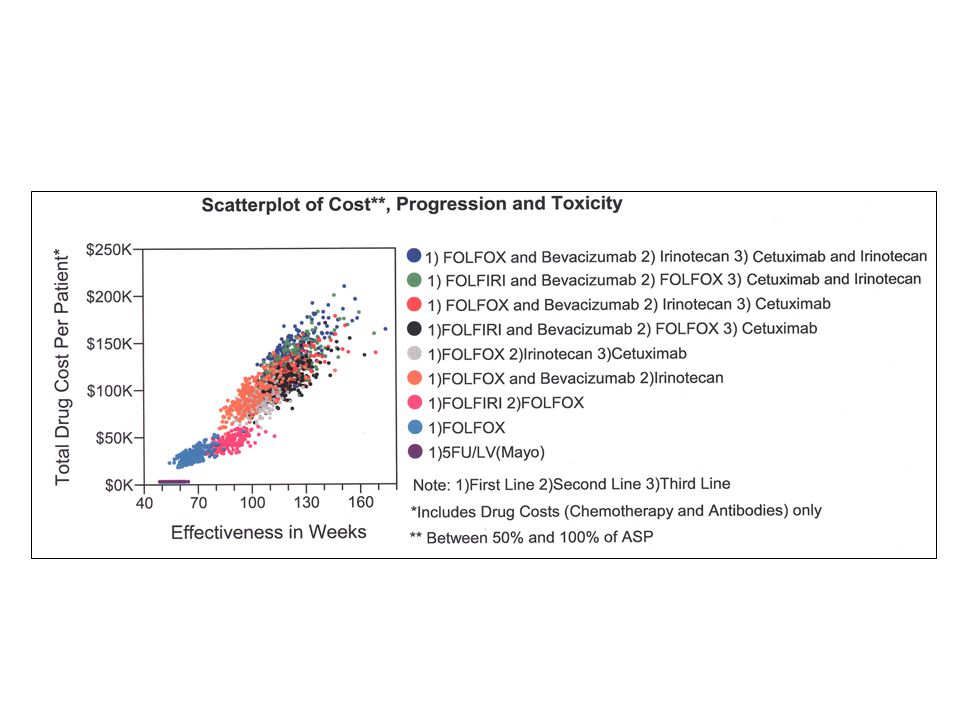
Two Dimensional Sensitivity Analyses –Probabilistic Toxicity and Progression varied over beta distribution Cost varied over continuous distribution (between 20% and 100% of ASP) –Microsimulation Trials (200 hypothetical patients)
 –Microsimulation Trials (200 hypothetical patients)")
17
Model uses aggregate data from multiple studies rather than patient level data –Results in inconsistent toxicity data –Only one dose reduction/delay Capecitabine-containing regimens are not yet incorporated (upcoming) Limitations
 Limitations")
18
Conclusions Our model suggests that the survival advantage afforded by new therapies comes at treatment related costs that may exceed currently accepted societal thresholds of cost effectiveness The CE ratios are more sensitive to changes in drug costs rather than improvement in clinical parameters (ie decrease in toxicity or increase in TTP) Cost effectiveness ratios may be improve with better methods of treatment selection for individual patients Cost effectiveness ratios may be improved if treatment with these agents in the adjuvant setting prove to be effective in preventing relapse
 Cost effectiveness ratios may be improve with better methods of treatment selection for individual patients Cost effectiveness ratios may be improved if treatment with these agents in the adjuvant setting prove to be effective in preventing relapse")
19
Acknowledgements Dr.Wong is supported by R25 CA 057708 (FCCC) and an ASCO Young Investigator Award References 1.Grothey A, Sargent D, Goldberg RM, Schmoll HJ. Survival of patients with advanced colorectal cancer improves with the availability of fluorouracil- leucovorin, irinotecan, and oxaliplatin in the course of treatment. J Clin Oncol. Apr 1 2004;22(7):1209-1214. 2.http://www.cms.hhs.gov/McrPartBDrugAvgSalesPrice / 3.Sanders GD, Hlatky MA, Owens DK. Cost-Effectiveness of Implantable Cardioverter-Defibrillators. N Engl J Med October 6, 2005 2005;353(14):1471- 1480
: / 3.Sanders GD, Hlatky MA, Owens DK. Cost-Effectiveness of Implantable Cardioverter-Defibrillators. N Engl J Med October 6, ;353(14):")
Similar presentations
 vs FOLFIRI plus bev>")




 versus FOLFOX4 in Patients with Advanced Colorectal Carcinoma Previously Treated.>")








: investigational agents TTP = median time to disease progression OS = median overall survival.>")




