Download presentation
Presentation is loading. Please wait.

1
The kidneys

2
Location -The kidneys are a pair of organs located in the back of the abdomen. - Each kidney is about 4 or 5 inches long -- about the size of a fist.

3
-more specifically in the paravertebral gutter and lie in a retroperitoneal position at a slightly oblique angle. There are two, one on each side of the spine -The left kidney is approximately at the vertebral level T12 to L3 and the right slightly lower. -The right kidney sits just below the diaphragm and posterior to the liver, the left below the diaphragm and posterior to thespleen.

4
The asymmetry within the abdominal cavity caused by the liver typically results in the right kidney being slightly lower than the left, and left kidney being located slightly more medial than the right

5
Anatomy of the Kidney

6
:Functions - The kidney participates in the excretion of the body wastes -regulating acid-base balance, -regulating electrolyte concentrations . -regulating extracellular fluid volume . - regulation of blood pressure. -Hormone secretion (including - erythropoietin( It stimulates (production of red blood cells) in the bone marrow), -the enzyme renin (Part of the renin-angiotensin-aldosterone system , renin is an enzyme involved in the regulation of aldosterone levels. Calcitriol, the activated form of vitamin D, promotes intestinal absorption of calcium and the renal reabsorption of phosphate .
 in the bone marrow), -the enzyme renin (Part of the renin-angiotensin-aldosterone system , renin is an enzyme involved in the regulation of aldosterone levels. -Calcitriol, the activated form of vitamin D, promotes intestinal absorption of calcium and the renal reabsorption of phosphate. .")
7
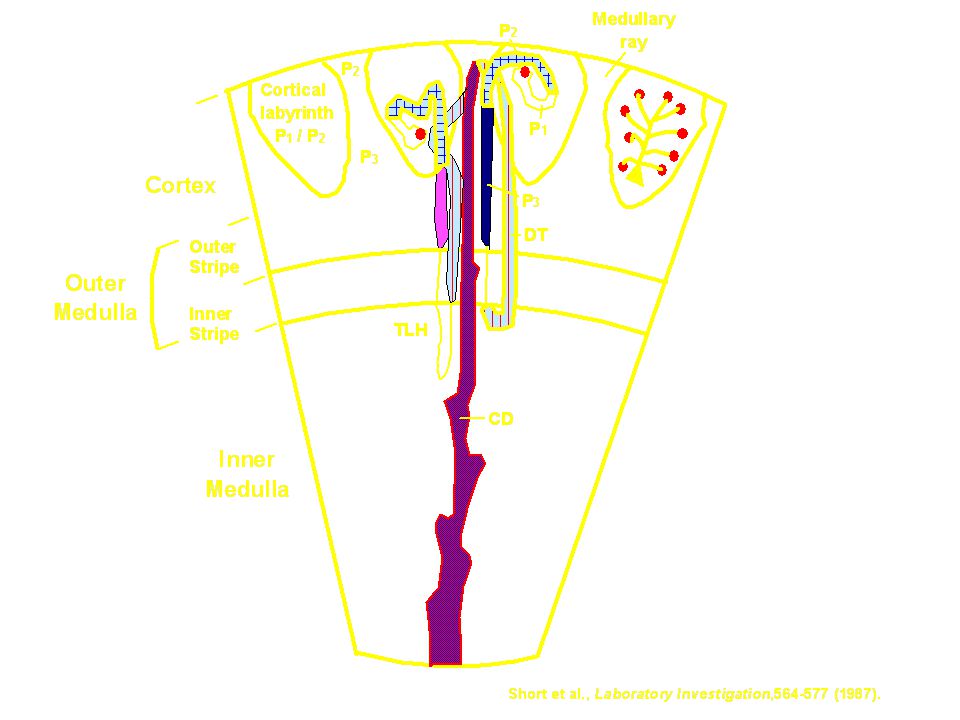
Structure and Function of the Kidney
The functional unit of the kidney is the nephron The major functions of the kidney are to maintain extracellular fluids, to eliminate wastes resulting from normal metabolism, and to excrete xenobiotics and their metabolites Mammalian kidneys have 10,000-1,000,000 nephrons per kidney

8
Renal toxicology

9
Structure and Function of the Kidney (cont)
The glomerulus yields an ultrafiltrate of plasma that represents 20% of the renal blood flow, ie. 2-3% of cardiac output Endothelial surface is negatively charged and contains fenestrae The glomerular basement membrane is sandwiched between the epithelial cells and contains anionic sialoglycoproteins, glycoproteins and collagen IV The mesangium provides support The outer capsule is Bowman’s capsule

10
Structure and Function of the Kidney (cont)
The tubule resorbs greater than 99% of the glomerular filtrate The proximal tubule has extensive resorption and selective secretion (convoluted - S1 and S2, straight - S3). S2 is primary site for low MW protein resorption and S3 is primary site for P450. Thin loop of Henle - resorption of fluids Distal tubule - resorption of fluids and acid-base balance Collecting duct - resorption of fluids, antidiuretic hormone and acid-base balance
. S2 is primary site for low MW protein resorption and S3 is primary site for P450. Thin loop of Henle - resorption of fluids. Distal tubule - resorption of fluids and acid-base balance. Collecting duct - resorption of fluids, antidiuretic hormone and acid-base balance.")
12
Structure and Function of the Kidney (cont)
Produces erythropoietin, which regulates RBC production Hydroxylates 25-OH-cholecalciferol (vitamin D metabolite), to promote bone resorption and calcium and phosphorus absorption from the gut Releases renin to regulate the peripheral renin-angiotensin-aldosterone system (juctaglomerular apparatus)
, to promote bone resorption and calcium and phosphorus absorption from the gut. Releases renin to regulate the peripheral renin-angiotensin-aldosterone system (juctaglomerular apparatus)")
13
Assessment of Kidney Function: Morphologic Evaluation
Urinalysis Gross evaluation of the kidney at necropsy Histopathology of the kidney Electron microscopy of the kidney

14
Assessment of Kidney Function: Urinalysis
Proteinuria - indicates glomerular damage Glycosuria - indicates tubular damage Urine volume and osmolarity pH Enzymes - indicates tubular damage Microscopic examination - casts, crystals, bacteria, etc.

15
Assessment of Kidney Function: Blood Chemistries
Blood urea nitrogen (BUN) Creatinine Electrolytes - Ca, Mg, K, P Glomerular filtration rate - determines the clearance of inulin, creatinine and BUN Renal clearance - measures the clearance of p-aminohippuric acid by filtration and secretion
 Creatinine. Electrolytes - Ca, Mg, K, P. Glomerular filtration rate - determines the clearance of inulin, creatinine and BUN. Renal clearance - measures the clearance of p-aminohippuric acid by filtration and secretion.")
16
Glomerular Disease: Toxicities due to Alteration of Anionic Charge
Hexadimethrine - polycationic molecule reduces anionic charge, which permits escape of anionic molecules such as albumin and IgG Polynucleoside of puromycin - damages epithelial foot processes

17
Glomerular Disease: Immune Complex Disease
Anti-GBM mediated glomerulonephritis is induced by heterologous antibodies Antibodies due to exogenous antigens - cationized molecules such as lysozyme, IgG and BSA bind to anionized surfaces; Concanavalin A binds to sugars in the GBM

18
Glomerular Disease: Immune Complex Disease (cont)
Deposition of circulating immune complexes Drug or toxin-induced T-cell dependent polyclonal B-cell activation - mercury in Brown Norway rats Unknown mechanism - gold salts, D-penicillamine, hydralazine Antibodies to heterologous proteins - safety evaluations of recombinant proteins in laboratory animals

19
Nephrosis: Damage to the renal tubule
Halogenated hydrocarbons - chloroform, hexachlorobutadiene, trichloroethylene, dibromochloropropane, & bromobenzene Heavy metals - cadmium, mercury & lead Antibiotics - cephalosporins & aminoglycosides Mycotoxins - ochratoxin A & citrinin Ethylene glycol Antineoplastic drugs - cisplatinum Alpha2u-globulin nephropathy

20
Haloalkane Nephrosis Chloroform is metabolized by P450 to an electrophile, phosgene, which is a potent cytotoxicant. Carbon tetrachloride is metabolized to free radicals and phosgene. P450 is localized in the proximal tubule. This results in nephrosis with necrosis, enzyme, glucose and protein excretion in urine, and increased BUN and creatinine concentrations in serum.

21
Haloalkene Nephrotoxicity
1,1-Dichloroethylene, trichloroethylene and tetrachloroethylene are metabolized by P450 to electrophilic metabolites and or free radicals. These metabolites can be cytotoxic and/or genotoxic. Nephrotoxicity is exacerbated when glutathione is depleted.

22
Glutathione-mediated Nephrosis
Glutathione conjugates of haloalkanes can form episulfonium ions. Primary route for 1,2-dichloroethane, 1,2-dibromoethane and 1,2-dibromo-3-chloro-propane. These can alkylate macromolecules and cause cytotoxicity and genotoxicity.

23
Cystine Conjugate -lyase Activation
Stable cystine conjugates from glutathione can be formed in the liver from trichloro-ethylene, tetrafluoroethylene and hexa-chlorobutadiene and transported to the kidney. They are further metabolized by -lyase in the kidney to generate reactive thiols.

24
Dialysis unit Indications of dialysis in acute renal failure (ARF)
is a process for removing waste and excess water from the blood, and is used primarily to provide an artificial replacement for lost kidney function in people with renal failure Indications of dialysis in acute renal failure (ARF) -Severe fluid overload -Refractory hypertension -Uncontrollable hyperkalemia -Nausea, vomiting, poor appetite, gastritis with hemorrhage Lethargy, malaise, somnolence, stupor, coma, delirium, asterixis, tremor, seizures,
 -Severe fluid overload. -Refractory hypertension. -Uncontrollable hyperkalemia. -Nausea, vomiting, poor appetite, gastritis with hemorrhage. Lethargy, malaise, somnolence, stupor, coma, delirium, asterixis, tremor, seizures,")
25
-Pericarditis (risk of hemorrhage or tamponade)
-bleeding diathesis (epistaxis, gastrointestinal (GI) bleeding and etc.) -Severe metabolic acidosis - Intoxication, that is, acute poisoning with a dialysable drug, such as lithium, or aspirin. -Blood urea nitrogen (BUN) > 70 – 100 mg/dl
 bleeding and etc.) -Severe metabolic acidosis. - Intoxication, that is, acute poisoning with a dialysable drug, such as lithium, or aspirin. -Blood urea nitrogen (BUN) > 70 – 100 mg/dl.")
26
Indications of dialysis in chronic renal failure (CRF)
-Pericarditis - Fluid overload or pulmonary edema refractory to diuretics -Accelerated hypertension poorly responsive to antihypertensives -Progressive uremic encephalopathy or neuropathy such as confusion, asterixis,-myoclonus, wrist or foot drop, seizures -Bleeding diathesis attributable to uremia

27
Types of Dialysis -hemodialysis (primary) .
-peritoneal dialysis (primary) . - hemofiltration (primary) . - hemodiafiltration (secondary) . - intestinal dialysis(secondary).
 . - hemofiltration (primary) . - hemodiafiltration (secondary) . - intestinal dialysis(secondary).")
28
Hemodialyzer

29
the patient's blood is pumped through the blood compartment of a dialyzer, exposing it to a partially permeable membrane Blood flows through the dialyzer, dialysis solution flows around the outside of the fibers, and water and wastes move between these two solutions by applying negative pressure ,The cleansed blood is then returned via the circuit back to the body

30
Advantages Disadvantage four dialysis-free days a week.
If you travel to another country, you will have to pre-arrange access to dialysis facilities Facilities are widely available. Trained professionals are with you at all times. You can get to know other patients. You don’t have to have a partner or keep equipment in your home. your diet and the amount of fluid that you drink needs to be restricted You are advised not to drink more than a couple of cups of fluid a day You have to avoid foods that are high in potassium

31
Peritoneal dialyzer

32
In peritoneal dialysis, a sterile solution containing glucose is run through a tube into the peritoneal cavity, the abdominal body cavity around theintestine, where the peritoneal membrane acts as a partially permeable membrane The dialysate is left there for a period of time to absorb waste products, and then it is drained out through the tube and discarded. This cycle or "exchange" is normally repeated 4-5 times during the day, (sometimes more often overnight with an automated system)
")
33
Advantages Disadvantage
- regular visits to a dialysis unit are not required and, in the case of home haemodialysis, there is no need to have a bulky machine installed in your house you need to perform it every day, whereas haemodialysis is usually only performed three days a week. major disadvantage of peritoneal dialysis is that your risk of developing peritonitis (infection of the peritoneum) is increased. more freedom to travel compared with haemodialysis patients. Peritonitis causes symptoms that include: abdominal pain vomiting chills (episodes of shivering and cold) fewer restrictions on diet and fluid intake compared with haemodialys reduction in protein levels, which can lead to a lack of energy and in some cases malnutrition.
 is increased. more freedom to travel compared with haemodialysis patients. Peritonitis causes symptoms that include: abdominal pain. vomiting. chills (episodes of shivering and cold) fewer restrictions on diet and fluid intake compared with haemodialys reduction in protein levels, which can lead to a lack of energy and in some cases malnutrition.")
34
Hemofiltration Hemofiltration is a similar treatment to hemodialysis, but it makes use of a different principle. The blood is pumped through a dialyzer or "hemofilter" as in dialysis, but no dialysate is used. - A pressure gradient is applied; as a result, water moves across the very permeable membrane rapidly, "dragging" along with it many dissolved substances, including ones with large molecular weights, which are not cleared as well by hemodialysis. Salts and water lost from the blood during this process are replaced with a "substitution fluid" that is infused into the extracorporeal circuit during the treatment.

35
Hemodiafiltration Hemodiafiltration is a term used to describe several methods of combining hemodialysis and hemofiltration in one process.

36
Intestinal dialysis In intestinal dialysis, the diet is supplemented with soluble fibres such as acacia fibre, which is digested by bacteria in the colon. This bacterial growth increases the amount of nitrogen that is eliminated in fecal waste An alternative approach utilizes the ingestion of 1 to 1.5 liters of non-absorbable solutions of polyethylene glycol or mannitol every fourth hour.

37
Electric cardioversion
a medical procedure by which an abnormally fast heart rate or cardiac arrhythmia is converted to a normal rhythm, using electricity

38
The purpose of the cardioversion is to interrupt the abnormal electrical circuit(s) in the heart and to restore a normal heartbeat. The delivered shock causes all the heart cells to contract simultaneously, thereby interrupting and terminating the abnormal electrical rhythm (typically fibrillation of the atria) without damaging the heart.
 without damaging the heart.")
39
Indications: two electrode pads are used
These are connected by cables to a machine which has the combined functions of an ECG display screen and the electrical function of a defibrillator Indications: - Synchronized electrical cardioversion is used to treat hemodynamically significant supraventricular tachycardias, including atrial fibrillation and atrial flutter. It is also used in the emergent treatment including ventricular tachycardia, when a pulse is present. -Pulseless ventricular tachycardia and ventricular fibrillation are treated with unsynchronized shocks referred to as defibrillation.

41
Ventialtor a machine designed to mechanically move breatheable air into and out of the lungs, to provide the mechanism of breathing for a patient who is physically unable to breathe, or breathing insufficiently.

42
Indications : -Acute lung injury (including ARDS, trauma)
- Apnea with respiratory arrest, including cases from intoxication -Chronic obstructive pulmonary disease (COPD) -Acute respiratory acidosis with partial pressure of carbon dioxide (pCO2) > 50 mmHg and pH < 7.25, which may be due to paralysis of the diaphragm due to Guillain-Barré syndrome,Myasthenia Gravis, spinal cord injury, or the effect of anaesthetic and muscle relaxant drugs -Increased work of breathing as evidenced by significant tachypnea, retractions, and other physical signs of respiratory distress Lateral Sclerosis
 -Acute respiratory acidosis with partial pressure of carbon dioxide (pCO2) > 50 mmHg and pH < 7.25, which may be due to paralysis of the diaphragm due to Guillain-Barré syndrome,Myasthenia Gravis, spinal cord injury, or the effect of anaesthetic and muscle relaxant drugs. -Increased work of breathing as evidenced by significant tachypnea, retractions, and other physical signs of respiratory distress. Lateral Sclerosis.")
43
-Hypoxemia with arterial partial pressure of oxygen (PaO2) < 55 mm Hg with supplemental fraction of inspired oxygen (FiO2) = 1.0 -Hypotension including sepsis, shock, congestive heart failure Neurological diseases such as Muscular Dystrophy and Amyotrophic

44
Disadvantages: It carries many potential complications including pneumothorax, airway injury, alveolar damage, and ventilator-associated pneumonia. It is used to support a single failing organ system (the lungs) and cannot reverse any underlying disease process (such as terminal cancer)
 and cannot reverse any underlying disease process (such as terminal cancer)")
45
Cardiac Assist Devices
Wayne E. Ellis, Ph.D., CRNA

46
Types Pacemakers AICDs VADs

47
History First pacemaker implanted in 1958 First ICD implanted in 1980
Greater than 500,000 patients in the US population have pacemakers 115,000 implanted each year

48
Pacemakers Today Single or dual chamber Multiple programmable features
Adaptive rate pacing Programmable lead configuration

49
Internal Cardiac Defibrillators (ICD)
Transvenous leads Multiprogrammable Incorporate all capabilities of contemporary pacemakers Storage capacity Have multiple Tachycardia zones with appropriate therapy Records adverse events and treatment

50
Temporary Pacing Indications
Routes = Transvenous, transcutaneous, esophageal Unstable bradydysrhythmias Atrioventricular heart block Unstable tachydysrhythmias *Endpoint reached after resolution of the problem or permanent pacemaker implantation Transvenous optimal. With transcutaneous AV capture happens simultaneously. With esophageal, possibly only atrial capture .

51
Permanent Pacing Indications
Chronic AVHB Chronic Bifascicular and Trifascicular Block AVHB after Acute MI Sinus Node Dysfunction Hypersensitive Carotid Sinus and Neurally Mediated Syndromes Miscellaneous Pacing Indications

52
Chronic AVHB Especially if symptomatic
Pacemaker most commonly indicated for: Type 2 2º Block occurs within or below the Bundle of His 3º Heart Block No communication between atria and ventricles

53
Chronic Bifascicular and Trifascicular Block
Differentiation between uni, bi, and trifascicular block Syncope common in patients with bifascicular block Intermittent 3º heart block common Block in the conduction systems below the Bundle of His ( in the bundle branches) Right bundle branch, and anterior and posterior fascicles of left bundle branch
 Right bundle branch, and anterior and posterior fascicles of left bundle branch.")
54
AVHB after Acute MI Incidence of high grade AVHB higher
Indications for pacemaker related to intraventricular conduction defects rather than symptoms Prognosis related to extent of heart damage

55
Sinus Node Dysfunction
Sinus bradycardia, sinus pause or arrest, or sinoatrial block, chronotropic incompetence Often associated with paroxysmal SVTs (bradycardia-tachycardia syndrome) May result from drug therapy Symptomatic? Often the primary indication for a pacemaker Chronotropic incompetence is known as a deficient rate response or stress or exercise Symptomology determined with ambulatory monitoring Pacemaker does not necessarily improve survival. Dual chamber pacing improves survival greater than ventricular pacing alone.
 May result from drug therapy. Symptomatic Often the primary indication for a pacemaker. Chronotropic incompetence is known as a deficient rate response or stress or exercise. Symptomology determined with ambulatory monitoring. Pacemaker does not necessarily improve survival. Dual chamber pacing improves survival greater than ventricular pacing alone.")
56
Hypersensitive Carotid Sinus Syndrome
• Syncope or presyncope due to an exaggerated response to carotid sinus stimulation • Defined as asystole greater than 3 sec due to sinus arrest or AVHB, an abrupt reduction of BP, or both Decreased blood pressure due to vasodilation Pure cardioinhibitory response, pacing helps Most people have a mixed response and attention must be given to both components.

57
Neurally Mediated Syncope
10-40% of patients with syncope Triggering of a neural reflex Use of pacemakers is controversial since often bradycardia occurs after hypotension In a recent study, a 85% reduction in risk of recurrent syncope in patients randomized to dual chamber pacing

58
Miscellaneous Hypertrophic Obstructive Cardiomyopathy
Dilated cardiomyopathy Cardiac transplantation Termination and prevention of tachydysrhythmias Pacing in children and adolescents Dual chamber pacemaker with a short atrioventricular delay reduces the magnitude of left ventricular outflow tract obstruction Pacemakers may help by changing the contraction pattern of the ventricle alleviates symptoms Improve hemodynamics using a dual-chamber pacemaker with short atrioventricular delay 2) Timing of atrial contractions, decreases mitral regurgitation High incidence of bradydysrhythmias 8-23% after transplant due to SND A flutter, PSVT, and VT. Pacing in kids for Sinus node dysfunction with symptomatic bradycardia, advanced 2nd or 3rd degree AVHB either congenital or acquired, especially if symptomatic. Consider if rate appropriate for child’s age and consider presence of ventricular dysfunction r/t congenital anomalies. No real rate criteria.
 Timing of atrial contractions, decreases mitral regurgitation. High incidence of bradydysrhythmias 8-23% after transplant due to SND. A flutter, PSVT, and VT. Pacing in kids for Sinus node dysfunction with symptomatic bradycardia, advanced 2nd or 3rd degree AVHB either congenital or acquired, especially if symptomatic. Consider if rate appropriate for child’s age and consider presence of ventricular dysfunction r/t congenital anomalies. No real rate criteria.")
59
Indications for ICDs Cardiac arrest due to VT/VF not due to a transient or reversible cause Spontaneous sustained VT Syncope with hemodynamically significant sustained VT or VF NSVT with CAD, previous MI, LV dysfunction and inducible VF or VT not suppressed by a class 1 antidysrhythmic

60
Device Selection Temporary pacing (invasive vs. noninvasive)
Permanent pacemaker ICD Invasive= epicardial and endocardial or transvenous. Non-invasive= transcutaneous or transesophageal. Temporary a good option to buy time until a permanent pacemaker can be implanted.

61
Pacemaker Characteristics
• Adaptive-rate pacemakers •Single-pass lead Systems • Programmable lead configuration • Automatic Mode-Switching • Unipolar vs. Bipolar electrode configuration

62
ICD selection Antibradycardia pacing Antitachycardia pacing
Synchronized or nonsynchronized shocks for dysrhythmias Many of the other options incorporated into pacemakers

63
Approaches to Insertion
a. IV approach (endocardial lead) b. Subcostal approach (epicardial or myocardial lead) c. Noninvasive transcutaneous pacing Alternative to emergency transvenous pacing
 b. Subcostal approach (epicardial or myocardial lead) c. Noninvasive transcutaneous pacing. Alternative to emergency transvenous pacing.")
64
Mechanics Provide the rhythm heart cannot produce
Either temporary or permanent Consists of external or internal power source and a lead to carry the current to the heart muscle Batteries provide the power source Pacing lead is a coiled wire spring encased in silicone to insulate it from body fluids

65
Unipolar Pacemaker Lead has only one electrode that contacts the heart at its tip (+) pole The power source is the (-) pole Patient serves as the grounding source Patient’s body fluids provide the return pathway for the electrical signal Electromagnetic interference occurs more often in unipolar leads

66
Unipolar Pacemaker

67
Bipolar Pacemaker If bipolar, there are two wires to the heart or one wire with two electrodes at its tip Provides a built-in ground lead Circuit is completed within the heart Provides more contact with the endocardium; needs lower current to pace Less chance for cautery interference

68
Bipolar Pacemaker

69
Indications 1. Sick sinus syndrome (Tachy-brady syndrome)
2. Symptomatic bradycardia 3. Atrial fibrillation 4. Hypersensitive carotid sinus syndrome Second-degree heart block/Mobitz II

70
Indications 6. Complete heart block Sinus arrest/block
Tachyarrhythmias Supraventricular, ventricular To overdrive the arrhythmia

71
Atrial Fibrillation * A fibrillating atrium cannot be paced
* Place a VVI * Patient has no atrial kick

72
Types 1. Asynchronous/Fixed Rate 2. Synchronous/Demand
3. Single/Dual Chamber Sequential (A & V) 4. Programmable/nonprogrammable
 4. Programmable/nonprogrammable.")
73
Asynchronous/Fixed Rate
Does not synchronize with intrinsic HR Used safely in pts with no intrinsic ventricular activity If pt has vent. activity, it may compete with pt’s own conduction system VT may result (R-on-T phenomenon) EX: VOO, AOO, DOO
 EX: VOO, AOO, DOO.")
74
Synchronous/Demand Contains two circuits * One forms impulses
* One acts as a sensor When activated by an R wave, sensing circuit either triggers or inhibits the pacing circuit Called “Triggered” or “Inhibited” pacers Most frequently used pacer Eliminates competition; Energy sparing

75
Examples of Demand Pacemakers
DDI VVI/VVT AAI/AAT Disadvantage: Pacemaker may be fooled by interference and may not fire

76
Dual Chamber: A-V Sequential
Facilitates a normal sequence between atrial and ventricular contraction Provides atrial kick + ventricular pacing Atrial contraction assures more complete ventricular filling than the ventricular demand pacing unit Increase CO 25-35% over ventricular pacing alone

77
A-V Sequential Disadvantage: More difficult to place More expensive
Contraindication: Atrial fibrillation, SVT Developed due to inadequacy of “pure atrial pacing”

78
Single Chamber Atrial Ventricular

79
“Pure Atrial Pacing” Used when SA node is diseased or damaged but AV conduction system remains intact Provides atrial kick Atrial kick can add 15-30% to CO over a ventricular pacemaker Electrode in atrium: stimulus produces a P wave

80
Problems with Atrial Pacing
Electrode difficult to secure in atrium Tends to float Inability to achieve consistent atrial “demand” function

81
Ventricular Pacemakers
If electrode is placed in right ventricle, stimulus produces a left BBB pattern If electrode is placed in left ventricle, stimulus produces a right BBB pattern

82
Programmability Capacity to noninvasively alter one of several aspects of the function of a pacer Desirable since pacer requirements for a person change over time Most common programmed areas Rate Output AV delay in dual chamber pacers R wave sensitivity Advantage: can overcome interference caused by electrocautery

83
3-Letter or 5-Letter Code
Devised to simplify the naming of pacemaker generators

84
First letter Indicates the chamber being paced A: Atrium V: Ventricle
D: Dual (Both A and V) O: None
 O: None.")
85
Second Letter Indicates the chamber being sensed A: Atrium
V: Ventricle D: Dual (Both A and V) O: Asynchronous or does not apply
 O: Asynchronous or does not apply.")
86
Indicates the generator’s response to a sensed signal/R wave
Third Letter Indicates the generator’s response to a sensed signal/R wave I: Inhibited T: Triggered D: Dual (T & I) O: Asynchronous/ does not apply
 O: Asynchronous/ does not apply.")
87
Fourth Letter Indicates programming information O: No programming
P: Programming only for output and/or rate M: Multiprogrammable C: Communicating R: Rate modulation

88
Fifth Letter This letter indicates tachyarrhythmia functions B: Bursts
N: Normal rate competition S: Scanning E: External O: None

89
Table of Pacer Codes

90
Types of Pulse Generators

91
Examples AOO A: Atrium is paced O: No chamber is sensed
O: Asynchronous/does not apply VOO V: Ventricle is paced

92
Examples VVI V: Ventricle is the paced chamber
V: Ventricle is the sensed chamber I: Inhibited response to a sensed signal Thus, a synchronous generator that paces and senses in the ventricle Inhibited if a sinus or escape beat occurs Called a “demand” pacer

93
Examples DVI D: Both atrium and ventricle are paced
V: Ventricle is sensed I: Response is inhibited to a sensed ventricular signal For A-V sequential pacing in which atria and ventricles are paced. If a ventricular signal, generator won’t fire Overridden by intrinsic HR if faster

94
Examples DDD DOO VAT Greatest flexibility in programming
Best approximates normal cardiac response to exercise DOO Most apparent potential for serious ventricular arrhythmias VAT Ventricular paced, atrial sensed Should have an atrial refractory period programmed in to prevent risk of arrhythmias induced by PACs from ectopic or retrograde conduction AV interval is usually milliseconds

95
Other Information Demand pacer can be momentarily converted to asynchronous mode by placing magnet externally over pulse generator in some pacers Dual chamber pacers preferable for almost all patients except those with chronic atrial fibrillation (need a working conduction system) Asynchronous pacer modes not generally used outside the OR OR has multiple potential sources of electrical interference which may prevent normal function of demand pacers
 Asynchronous pacer modes not generally used outside the OR. OR has multiple potential sources of electrical interference which may prevent normal function of demand pacers.")
96
Other Information VVI: Standard ventricular demand pacemaker
DVI: AV pacemaker with two pacing electrodes Demand pacer may be overridden by intrinsic HR if more rapid Demand pacer can be momentarily converted to asynchronous mode by placing magnet externally over pulse generator

97
Sensing Ability of device to detect intrinsic cardiac activity
Undersensing: failure to sense Oversensing: too sensitive to activity

98
Undersensing: Failure to sense
Pacer fails to detect an intrinsic rhythm Paces unnecessarily Patient may feel “extra beats” If an unneeded pacer spike falls in the latter portion of T wave, dangerous tachyarrhythmias or V fib may occur (R on T) TX: Increase sensitivity of pacer
 TX: Increase sensitivity of pacer.")
99
Oversensing Pacer interprets noncardiac electrical signals as originating in the heart Detects extraneous signals such as those produced by electrical equipment or the activity of skeletal muscles (tensing, flexing of chest muscles, SUX) Inhibits itself from pacing as it would a true heart beat
 Inhibits itself from pacing as it would a true heart beat.")
100
Oversensing On ECG: pauses longer than the normal pacing interval are present Often, electrical artifact is seen Deprived of pacing, the patient suffers CO, feels dizzy/light-headed Most often due to sensitivity being programmed too high TX: Reduce sensitivity

101
Capture Depolarization of atria and/or ventricles in response to a pacing stimulus

102
Noncapture/Failure to Capture
Pacer’s electrical stimulus (pacing) fails to depolarize (capture) the heart There is no “failure to pace” Pacing is simply unsuccessful at stimulating a contraction ECG shows pacer spikes but no cardiac response CO occurs TX: threshold/output strength or duration
 fails to depolarize (capture) the heart. There is no failure to pace Pacing is simply unsuccessful at stimulating a contraction. ECG shows pacer spikes but no cardiac response. CO occurs. TX: threshold/output strength or duration.")
103
Pacer Failure A. Early B. Failure > 6 months
electrode displacement/breakage B. Failure > 6 months Premature battery depletion Faulty pulse generator

104
Pacer Malfunctions per ECG
Failure to capture Failure to sense Runaway pacemaker

105
Pacer Malfunction SX 1. Vertigo/Syncope 2. Unusual fatigue
*Worsens with exercise 2. Unusual fatigue 3. Low B/P/ peripheral pulses 4. Cyanosis 5. Jugular vein distention 6. Oliguria 7. Dyspnea/Orthopnea 8. Altered mental status

106
EKG Evaluation Capture: Should be 1:1 (spike:EKG complex/pulse)
*Not helpful if patient’s HR is > pacer rate if synchronous type

107
EKG Evaluation Proper function of demand pacer
Confirmed by seeing captured beats on EKG when pacer is converted to asynchronous mode Place external converter magnet over generator Do not use magnet unless recommended

108
CAPTURE Output: amt of current (mAmps) needed to get an impulse
Sensitivity: (millivolts); the lower the setting, the more sensitive
; the lower the setting, the more sensitive.")
109
Anesthesia for Insertion
MAC To provide comfort To control dysrhythmias To check for proper function/capture Have external pacer/Isuprel/Atropine ready Continuous ECG and peripheral pulse Pulse ox with plethysmography to see perfusion of each complex (EKG may become unreadable)
")
110
Pacemaker Insertion

111
Interference Things which may modify pacer function:
Sympathomimetic amines may increase myocardial irritability Quinidine/Procainamide toxicity may cause failure of cardiac capture K+, advanced ht disease, or fibrosis around electrode may cause failure of cardiac capture

112
Anesthesia for Pt with Pacemaker
a. Continuous ECG and peripheral pulse b. Pulse ox with plethysmography to see perfusion of each complex (EKG may become unreadable) c. Defibrillator/crash cart available d. External pacer available e. External converter magnet available
 c. Defibrillator/crash cart available. d. External pacer available. e. External converter magnet available.")
113
Anesthesia for Pt with Pacemaker
If using Succinylcholine, consider defasciculating dose of MR Fasciculations may inhibit firing due to the skeletal muscle contractions picked up by generator as intrinsic R waves Place ground pad far from generator but close to cautery tip Cover pad well with conductive gel Minimizes detection of cautery current by pulse generator If patient has a transvenous pacemaker, increased risk of V. fib from microshock levels of electrical current

114
Anesthesia for Pt with Pacemaker
Cautery may interfere with pacer: May inhibit triggering (pacer may sense electrical activity and not fire) May inadvertently reprogram May induce arrhythmias secondary to current May cause fixed-rate pacing
 May inadvertently reprogram. May induce arrhythmias secondary to current. May cause fixed-rate pacing.")
115
Automatic Implantable Cardiac Defibrillators

116
AICD

117
Parts of AICD Pulse generator with batteries and capacitors
Electrode or lead system Surgically placed in or on pericardium/myocardium Monitors HR and rhythm Delivers shock if VT or Vfib

118
Placement of AICD Pulse Generator

119
AICD Indications Risk for sudden cardiac death
caused by tachyarrhythmias (VT, Vfib) Reduces death from 40% to 2% per year
 Reduces death from 40% to 2% per year.")
120
Defibrillator Codes First letter: Shock Chamber A: atrium V: ventricle
D: dual O: none

121
Defibrillator Codes Second letter: Antitachycardia Chamber
A: atrium V: ventricle D: dual O: none Third letter: Tachycardia Detection E: EKG H: Hemodynamics

122
Defibrillator Codes Fourth letter: Antibradycardia Pacing Chamber
A: atrium V: ventricle D: dual O: none

123
Settings Gives a shock at 0.1-30 joules Usually 25 joules
Takes 5-20 seconds to sense VT/VF Takes 5-15 seconds more to charge second delay before next shock is administered Total of 5 shocks, then pauses If patient is touched, may feel a buzz or tingle If CPR is needed, wear rubber gloves for insulation

124
Tiered Therapy Ability of an implanted cardioverter defibrillator to deliver different types of therapies in an attempt to terminate ventricular tachyarrhythmias EX of therapies: Anticardiac pacing Cardioversion Defibrillation Antibradycardia pacing

125
Anesthesia MAC vs General Lead is placed in heart
Usually general due to induction of VT/VF so AICD can be checked for performance Lead is placed in heart Generator is placed in hip area or in upper chest

126
VADs Ventricular assist devices
Implantable pumps used for circulatory support in pts with CHF Blood fills device through a cannulation site in V or A Diaphragm pumps blood into aorta or PA Set at predetermined rate (fixed) or automatic (rate changes in response to venous return)
 or automatic (rate changes in response to venous return)")
127
Electromagnetic Interference on Pacers and AICDs
Electrocautery May inhibit or trigger output May revert it to asynchronous mode May reprogram inappropriately May induce Afib or Vfib May burn at lead-tissue interface

128
Electromagnetic Interference on Pacers and AICDs
Defibrillation May cause permanent damage to pulse generator May burn at lead-tissue interface Radiation Therapy May damage metal oxide silicon circuitry May reprogram inappropriately

129
Electromagnetic Interference on Pacers and AICDs
PET/CT (Contraindicated) May damage metal oxide silicon circuitry May reprogram inappropriately MRI (Contraindicated) May physically move pulse generator May give inappropriate shock to pt with AICD PNSs May cause inappropriate shock or inhibition Test at highest output setting
 May damage metal oxide silicon circuitry. May reprogram inappropriately. MRI (Contraindicated) May physically move pulse generator. May give inappropriate shock to pt with AICD. PNSs. May cause inappropriate shock or inhibition. Test at highest output setting.")
130
Deactivating a Pacemaker
Deactivate to prevent inappropriate firing or inhibition Can be deactivated by a special programmer/wand or by a magnet placed over generator for 30 seconds Put in asynchronous mode or place external pacer on patient

131
If Pt has a Pacemaker/AICD
Not all models from a certain company behave the same way with magnet placement ! For all generators, call manufacturer Most reliable method for determining magnet response ! !

132
Coding Patient If patient codes, do not wait for AICD to work
Start CPR & defibrillate immediately Person giving CPR may feel slight buzz A 30-joule shock is < 2 j on pt’s skin External defibrillation will not harm AICD Change paddle placement if unsuccessful attempt Try A-P paddle placement if A-Lat unsuccessful

133
Pts with Pacemakers/AICDs/VADs
Obtain information from patient regarding device Ask how often patient is shocked/day High or low K+ may render endothelial cells more or less refractory to pacing A properly capturing pacemaker should also be confirmed by watching the EKG and palpating the patient’s pulse

134
Anesthetic Considerations
Avoid Succinylcholine Keep PNS as far from generator as possible Have backup plan for device failure Have method other than EKG for assessing circulation Have magnet available in OR

135
Electrocautery Use Place grounding pad as far from generator as possible Place grounding pad as near to surgical field as possible Use bipolar electrocautery if possible Have surgeon use short bursts of electrocautery (<1 sec, 5-10 seconds apart) Maintain lowest possible current
 Maintain lowest possible current.")
136
Electrocautery Use If cautery causes asystole, place magnet over control unit & change from inhibited to fixed mode Change back afterwards Be alert for R on T phenomenon

137
Postoperative Considerations
Avoid shivering Have device checked and reprogrammed if questions arise about its function

138
Examples of Rhythms Sensing
Patient’s own beat is sensed by pacemaker so does not fire

139
Examples of Rhythms Undersensing
Pacemaker doesn’t sense patient’s own beat and fires (second last beat)
")
140
Examples of Rhythms Oversensing
Pacemaker senses heart beat even though it isn’t beating. Note the long pauses.

141
Examples of Rhythms Capture
Pacemaker output (spike) is followed by ventricular polarization (wide QRS).
 is followed by ventricular polarization (wide QRS).")
142
Examples of Rhythms Noncapture
Pacer stimulus fails to cause myocardial depolarization Pacer spike is present but no ECG waveform Oversensing-Fails to fire Undersensing- Fails to sense ECG Fires but fails to capture Pacer spikes after theQRS

143
Examples of Rhythms 100 % Atrial Paced Rhythm with 100% Capture

144
Examples of Rhythms 100% Ventricular Paced Rhythm with 100% Capture

145
Examples of Rhythms 100% Atrial and 100% Ventricular Paced Rhythm with 100% Capture

146
Examples of Rhythms 50% Ventricular Paced Rhythm with 100% Capture

147
Examples of Rhythms 25% Ventricular Paced Rhythm with 100% Capture (Note the sensing that occurs. Pacer senses intrinsic HR and doesn’t fire).
.")
148
Examples of Rhythms AICD Shock of VT Converted to NSR

149
Examples of Rhythms

150
Examples of Rhythms

151
Examples of Rhythms DDD Pacemaker

152
References Moser SA, Crawford D, Thomas A. AICDs.
CC Nurse. 1993;62-73. Nagelhaut JJ, Zaglaniczny KL. Nurse Anesthesia. Philadelphia: Saunders.1997. Ouellette, S. (2000). Anesthetic considerations in patients with cardiac assist devices. CNRA, 23(2), 9-20. Roth, J. (1994). Programmable and dual chamber pacemakers: An update. Progress in anes thesiology, 8, chapter 17. WB Saunders.
. Anesthetic considerations in patients with cardiac assist devices. CNRA, 23(2), Roth, J. (1994). Programmable and dual chamber pacemakers: An update. Progress in anes thesiology, 8, chapter 17. WB Saunders.")
153
Pacemaker a medical device that uses electrical impulses, delivered by electrodes contacting the heart muscles, to regulate the beating of the heart , and maintain an adequate heart rate, either because of the heart's native pacemaker is not fast enough, or there is a block in the heart's electrical conduction system

Similar presentations

















 System>")



